
Abstract
Purpose:
Hoffa fractures are uncommon intra-articular fractures of femoral condyle in coronal plane. The purpose of our study is to assess radiologic and functional outcome in operatively treated Hoffa fractures.
Methods:
We retrospectively reviewed 32 patients of isolated Hoffa fracture from January 2010 to March 2015. All were treated with open reduction and internal fixation using lateral approach for lateral Hoffa and medial approach for medial Hoffa fracture. Cancellous screws in lag mode and/or antiglide plate were employed for fixation in accordance with fracture anatomy. All patients were subjected to aggressive physical therapy postoperatively. Knee Society Score (KSS), International Knee Documentation Committee Score (IKDC), and Knee range of motion (ROM) were documented at final follow-up for functional evaluation.
Results:
All fractures united by mean time of 11.56 ± 1.5 weeks. No evidence of subsequent displacement or fixation failure, arthritis, Avascular necrosis (AVN) of femoral condyle was elicited in any of the patients. Documented mean KSS and mean IKDC Score at final follow-up were 83.19 ± 8.43 and 81.62± 6.95, respectively. ROM at final follow-up was ranging from 0° to mean 116.41° ± 13.98°. Complications included stiffness of the involved knee in four patients, including one patient who developed infection and had to undergo implant removal after fracture union.
Conclusion:
Operative treatment of Hoffa fractures yields fairly good functional outcome. One must endeavor to achieve adequate intraoperative exposure and stable congruous articular reconstruction. Early aggressive physical therapy is a harbinger of optimal outcome.
Introduction
Hoffa fracture, described by Albert Hoffa in 1904, is an intra-articular fracture affecting either femoral condyle in coronal plane. 1 Although there is preponderance for lateral condyle, medial condyle involvement is not as uncommon as previously suspected. These uncommon coronal fractures have not been accorded due interest in past, which is evident by the fact that only few case reports and case series describing the nature of this fracture and its management have been presented. 2 –8 Hence, there is a lack of concrete evidence in literature regarding these fractures. The management has come a long way from nonoperative treatment to anatomical reduction and internal fixation of these fractures. Herein, we describe our treatment results of a large retrospective analysis of 32 consecutive patients with isolated Hoffa fracture who presented to our level 1 trauma center and review the existing literature regarding the injury pattern, surgical treatment options, and outcomes.
Materials and methods
We retrospectively identified 45 patients with Hoffa fractures operated at our level 1 Trauma center between the study period of January 2010 and March 2015. Isolated Hoffa fractures in adults were included in the study, whereas patients with open physes, pathological fractures, concomitant supracondylar or intercondylar involvement, associated ipsilateral tibial fracture, or preexisting knee arthritis were excluded. Thirty-four patients met the inclusion criteria and were called telephonically for final follow-up, but two patients did not show up. After exclusion, 32 patients with isolated Hoffa fractures were studied for retrospective evaluation.
The patient’s preoperative sociodemographics and clinical data were obtained from hospital’s electronic database and documented on a proforma. Preoperative anteroposterior (AP) and lateral X-rays of the involved knee and computed tomography (CT) scan of the knee with three-dimensional (3-D) reconstruction were assessed and findings were documented.
All the procedures were done by an open approach with the patients placed in supine position on radiolucent table and under tourniquet control. Operations were performed either by senior consultant (first author) or by trained trauma residents. All surgeries were performed under the supervision of senior consultant after thorough deliberations and preoperative planning. Standard lateral incision (Figure 1) was given for lateral condylar fractures and exposure made between iliotibial tract and biceps femoris, while a medial incision (Figure 2) was used in case of medial condyle fractures. After thorough joint inspection, the fracture surfaces were identified and the presence of any comminution, meniscal injury, or collateral ligament injury was noted. The fracture surfaces were debrided, reduced anatomically, and fixed provisionally with Weber bone clamps and/or K wires. For placement of lateral screw, knee was flexed to approximately 90° and 6.5-mm or 4-mm partially threaded cancellous screw was placed in AP direction perpendicular to fracture line, starting proximal to patellofemoral joint. In cases where articular cartilage was violated by screw insertion, screw head was countersunk. Similarly, medial side fixation was done with 6.5-mm or 4-mm cancellous screw in AP direction perpendicular to fracture line, and screw head was buried into the cartilage. A minimum of two screws were used to gain rotational control. AP screw positioning was facilitated by small stab incisions placed anteriorly (Figure 2). The usage of different screw diameter and number was based on fracture configuration. The decision regarding choice of implant was done by the senior author (VT) based on the fracture pattern, bone morphology, and patient general profile. The presence of comminution, osteoporosis, and metaphyseal extension prompted us to use an antiglide plate in addition to the lag screw. Image intensifier was used to control reduction and screw placement. Care was taken to protect fat pad and meniscal attachments. Stability of knee was checked routinely after fracture fixation. Meticulous hemostasis was achieved after tourniquet deflation, and standard wound closure was done after placing a drain.

Anteroposterior (a) and lateral (b) radiograph of knee showing lateral condyle Hoffa fracture (white arrow). Open reduction done through lateral approach and fixed with two AP partially threaded cancellous screws (c and d). AP: anteroposterior.

Anteroposterior (a) and lateral (b) radiograph of knee of a case of medial condyle Hoffa fracture appearing quite unimpressive, whereas axial (c) and sagittal (d) reformatted CT scan clearly delineating fracture. Postoperative AP (e) and lateral (f) radiograph showing anatomic reconstruction with two 4-mm cancellous screws through medial approach. Anteroposterior screws were placed percutaneously through small incision anteriorly (white arrow). CT: computed tomography; AP: anteroposterior.
Postoperatively, active range of motion (ROM) exercises were commenced immediately. Initial toe touch weight bearing was allowed which graduated to full weight bearing by 10–12 weeks. Initial postoperative radiograph was assessed by an independent observer in radiology department for accuracy of reduction, which was graded as acceptable (<2 mm step) and poor (≥2 mm step). All patients had regular clinical and radiological follow-up. The final radiograph was assessed for any subsequent displacement, fixation failure, and evidence of union. Union was defined as no pain with weight bearing and trabeculae crossing fracture site in standard radiographs. Clinical evaluation measures included documenting the Knee Society Clinical Score (KSS), International Knee Documentation Committee (IKDC) subjective scores, and knee range of motion at final follow-up. Accuracy of data collection was ascertained by reviewing patient’s file, hospital’s electronic database and radiologic database, and by blinding of the data analyst.
Statistics
Statistical analysis was performed using SPSS version 16 software. Continuous variables were described as means and standard deviation. Categorical data were described as absolute and relative frequencies. Assessment of differences between groups were performed by independent t-test, and level of significance was set at p value <0.05.
Results
A total of 32 patients comprising of 25 (78.1%) males and 7 (21.9%) females with a mean age of 34.72 ± 7.26 years (range 22–48 years) constituted the study group. All patients had minimum follow-up of 1-year postinjury (range 1–5 years). Road traffic accident (81.25%) was the most common mode of injury followed by fall from height (18.75%). Most of the patients (62.5%) were driving or were pillion riders in a two wheeler at the time of accident. The fracture involved the right knee in 18 (56.3%) patients and left knee in 14 (43.8%) patients. All the injuries were closed except in three patients (9.38%) who had a grade I open injury. Twenty-one (65.63%) patients had lateral condyle involvement, and 11 (34.38%) had medial condyle involvement. No vascular or neurological injury was documented in any of the patient. No subluxation or dislocation of the knee joint or concomitant ligament injury was noted in any of the patient. All the patients underwent surgery after a mean delay of 1.47 ± 1.08 days (range 0–7 days) after injury.
The mean tourniquet time was 71.69 ± 23.68 min (range 40–120 min), and mean blood loss was found to be 191.25 ± 60.63 ml (range 100–300 ml). Most of the patients were treated with 6.5-mm (20 patients) or 4-mm (11 patients) partially threaded cancellous screw used in lag mode in AP direction. Antiglide plate was used in seven patients. The documented knee ROM at final follow-up was ranging from 0° to mean 116.41° ± 13.98° (Figure 3). Among four patients (12.5%) who developed stiffness of the involved knee, two were noncompliant and did not show up for regular follow-up, one patient had infection, and in other elderly patient in view of severe fracture comminution and osteoporosis, physical therapy was delayed which led to mild stiffness. All the patients had progressive improvement in their knee functions; documented mean KSS and IKDC scores at final follow-up were 83.19 ± 8.43 and 81.62 ± 6.95, respectively.
All patients had acceptable reduction of the fracture (<2 mm step) with no evidence of articular incongruity, except for three patients (9.38%) who had articular step of ≥2 mm, which was partly because of severe comminution at fracture site in two patients. The third patient had delayed presentation and intervention was done after 8 days postinjury. There was no loss of subsequent reduction or fixation failure noted in any of the patients. No evidence of post-traumatic arthritis of the involved knee or AVN of femoral condyle was found in any of the patients at final follow-up. All patients had radiographic evidence of union at follow up; mean time to union was 11.56 ± 1.5 weeks. There was no evidence of superficial or deep infection noted in any of the patients, except for one patient who had a preoperative stiff knee from previous infection. He developed deep infection in the postoperative period and had to undergo implant removal after fracture union at 4 months. At 1 year, that patient was free from any active infection, but final range of motion was 20°–70°. Age, sex, site of fracture, and fixation method used did not bear any significant influence on functional outcome in our study. At final follow-up, average ROM, KSS, and IKDC score were relatively better, and complications were less in case of medial condyle Hoffa fractures as compared to lateral condyle Hoffa fractures; however, differences were not statistically significant (p > 0.05). Patients’ demographic data and results are summarized in Tables 1 and 2.
Summarized patients’ demographics and results.

M: male; F: female; R: right; L: left; MC: medial condyle; LC: lateral condyle; ROM: range of motion; AP: anteroposterior; PA: posteroanterior; KSS: Knee Society Clinical Score; IKDC: International Knee Documentation Committee.
Comparison between medial and lateral condyle Hoffa fractures.
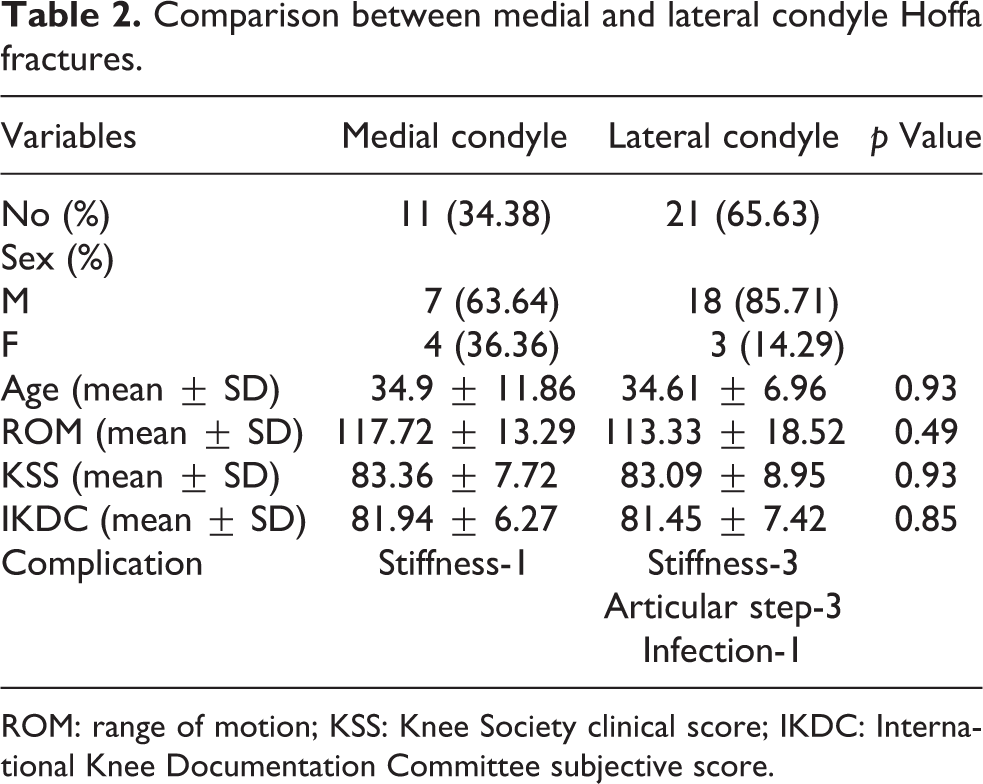
ROM: range of motion; KSS: Knee Society clinical score; IKDC: International Knee Documentation Committee subjective score.
Discussion
Hoffa fractures are rare injuries postulated to occur as a result high-energy mechanism, usually affecting young adults. 2 They usually occur as an isolated injury but bilateral involvement 3 and unilateral bicondylar Hoffa fractures 4 have also been reported. In addition, substantial prevalence of Hoffa fractures in association with supracondylar–intercondylar distal femur fractures has been documented. 9
Mechanism of injury continues to remain elusive. The usual mechanism is postulated to be a combination of vertical shearing and twisting forces. 4 Lewis et al. 2 argued that with the knee flexed to just beyond 90°, the lateral femoral condyle is the leading part of the knee to receive an oblique or lateral impact. Direct trauma to this area, possibly with an element of abduction, results in the typical Hoffa fracture. The physiological genu valgum may be the underlying basis for the predominant lateral condyle involvement in these fractures. 5 However, no corroborative biophysical study exists favoring this hypothesis and hence the dilemma behind the mechanism of injury. Similar to the study by Lewis et al., 2 most of our patients were in a two wheeler at the time of accident which is the most common mode of personal travel in our country.
A high index of suspicion is needed to diagnose these fractures. Standard AP radiograph may appear unimpressive owing to intact anterior part of condyle; moreover, undisplaced fracture may not be apparent in lateral radiograph (Figure 2). Oblique radiographs and CT scans have been recommended to facilitate the diagnosis of these injuries. CT scan with 3-D reconstruction helps in identifying the exact site of fracture, presence of comminution and assists in preoperative planning. 9 In view of the rarity of the fracture, very few classification systems exist for this fracture. AO/OTA classification identifies these fractures as 33-B3 but provides little information about prognosis or treatment. 6 The most common and widely accepted classification was described by Letenneur et al., 10 based on the orientation of fracture line, integrity of soft tissues attached to the fracture and predictability of developing avascular necrosis; three types were described. However, the predictability has been not corroborated by clinical studies. 2,8 In our study, no cases of AVN were reported, which further adds to this conundrum.
Conservative management is generally associated with suboptimal results; 2,7 therefore, the management has evolved into open reduction and internal fixation at present, which is stemmed from the fact that like any intra-articular fractures, anatomic reduction, and stable fixation are cornerstones for optimal outcome. However, no clear and straightforward dependable treatment rationale has been formulated due to dearth of specific information in literature. Substantial debate is going on concerning surgical approach, fixation methods. A midline incision with a medial/lateral parapatellar arthrotomy is the most common approach reported. 2,6,8 Direct lateral approach between iliotibial tract and biceps femoris has also been favored by many. 2,4,5 Liebergall et al. 11 recommended the straight lateral parapatellar approach, with osteotomy of Gerdy’s tubercle and reflection of the iliotibial tract. They argued that this provides excellent exposure of the lateral femoral condyle and permits anatomic reduction of the fragments without violating the articular surface. It also allows the harvest of a local bone graft from the tibial metaphysis. Papadopoulos et al.4 favored an additional medial incision for fixation of medial fragment. We feel that individualized approach for either condyle Hoffa fracture gives ample direct exposure of the fractured region. It is also less invasive compared to medial/lateral parapatellar approach as it spares the extensor mechanism. Moreover, antiglide plate placement was found to be easier than parapatellar approach as enough exposure of posterolateral and posteromedial aspect can be obtained through direct approach (Figures 3 and 4). The screws may be placed in AP direction percutaneously with separate small incisions in this approach. Judicious use of separate medial and lateral approach for medial and lateral condyle Hoffa fractures, respectively, has yielded encouraging results in our hands with regard to articular reduction, screw placement, and, if necessary, plate positioning. However, accurate delineation of fracture is paramount before embarking on this individualized approach. Preoperative planning with CT scan is crucial in this regard, as standard radiographs cannot be relied solely. Reports of arthroscopic-assisted reduction and internal fixation of femoral condyle have also appeared in recent times citing advantages of reduced soft tissue dissection, blood loss, operative time, and a faster recovery time. 12 However, no long-term trial exists comparing the outcomes of arthroscopic and open procedures. Whatever approach is used as per surgeon’s preferences, adequate visualization of fracture fragments is paramount to aid congruous reduction of articular surfaces and hence optimize the outcome.

Anteroposterior (a) and lateral (b) radiograph of knee showing lateral condyle Hoffa fracture reconstructed with a 3.5-mm L-antiglide plate in addition to AP 4-mm cancellous screws. Clinical photographs (c and d) of the same patient 1 year after operation demonstrate excellent result of the involved knee. AP: anteroposterior.

Standard radiograph (a) and 3-D CT scan (b) of knee depicting displaced medial condyle Hoffa fracture (white arrow). Postoperative radiograph (c) depicts congruous articular reduction and stable fixation with an antiglide plate. CT: computed tomography.
The type of implant and the direction of screw insertion are also point of substantial debate. In a cadaveric study, Jarit et al. 13 concurred that lag screws placed posterior to anterior provide more stable fixation of Hoffa fractures than anteroposteriorly placed lag screws. However, this technique requires that the screw heads be recessed beneath the articular surface which invariably leads to large articular surface defect. Moreover, risk of injury to the common peroneal nerve or popliteal vessels is present using this method. 14 A probable solution to this problem is the use of headless compression screws which can minimize the cartilage damage. 15 Since they need to be put perpendicular to the fracture line which leads to more soft tissue violation, this approach was not used by us. Moreover, the biomechanical strength of these screws needs to be evaluated to promulgate their regular use. Another cadaveric study evaluated the stiffness and load to failure of 3.5-mm cortical lag screws, 4.5-mm cortical lag screws, and 6.5-mm cancellous screws and found no difference in stiffness between any of the groups, but the load to failure was significantly higher for 6.5-mm screws compared with 3.5-mm screws. However, the authors were pragmatic about their results and opined that smaller screws, such as 3.5-mm cortical screws, may be much easier to fit around a rigid implant if such fixation is necessary. 16 Similarly, in a biomechanical evaluation, Hak et al. 17 concluded that two 6.5-mm screws are more rigid than either single or double 3.5-mm screws. The use of a second screw marginally increases the rigidity of fixation. In our study, we used 6.5-mm or 4-mm partially threaded cancellous screws in AP direction depending on the fracture pattern and had fairly good results. The use of antiglide plate for comminuted Hoffa fracture has to be considered, 18 which we had used in seven of our cases. We believe that in the presence of substantial fracture comminution, where adequate screw purchase is questionable; the additional support given by the plate would enhance the stability of fracture fixation and prevent collapse or loss of reduction. Apart from this, Hoffa fracture with metaphyseal extension and osteoporotic bone also warrant consideration for plate support.
Our results are comparable to other published series. 2,6,8 Results emanating from our series point toward relatively better outcome in operatively treated medial condyle Hoffa fractures than lateral condyle involvement, albeit it failed to reach statistical significance. Few complications were seen, mostly in case of lateral condyle involvement, and we speculate delay of surgery, poor articular reduction, comminution, and osteoporosis portend poor functional outcome. To the best of our knowledge, this is the largest retrospective case series described of this rare fracture with an adequate follow-up. The strength of our study lies in the fact that we had used standardized surgical approach and employed validated objective and subjective scoring systems. However, we recognize our limitations. Apart from being retrospective study design, lack of control cohort, which is partly because of the rare nature of fracture, and use of nonhomogenous group of patients and fixation methods precluded us from drawing definitive conclusions. In addition, we also take cognizance of the fact that this result from our level 1 Trauma center may not represent the fracture pattern seen in other centers. A comparative trial with longer follow-up period would answer the lingering questions.
In conclusion, Hoffa fractures are uncommon intra-articular fractures that demand careful evaluation and precise planning. Open reduction with congruous restoration of articular surface and stable fixation is critically important to accomplish. This rational approach combined with unrestricted immediate range of motion of the joint is paramount to envisage optimal outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.