
Abstract
Background:
Developmental dysplasia of the hip (DDH) is one of the prevalent musculoskeletal conditions in young adults and is a leading cause of hip osteoarthrosis in this age group. The optimum age for surgical intervention when needed is not well established in the literature and the lack of management guidelines and standard practice of DDH leads to different practices worldwide. This study aims to investigate the current practice of paediatric orthopaedic surgeons in diagnosing and treating DDH worldwide and identify points of agreement and disagreement.
Methods:
A cross-sectional study utilizing an online questionnaire was designed to examine the different points of view and current practice of paediatric orthopaedic surgeons worldwide regarding DDH diagnosis and treatment.
Results:
Ninety-one surgeons responded, with an overall response of 45.5%. The vast majority of respondents use ultrasonography in children less than 3 months of age and pelvic radiography in over 3 months to diagnose DDH. Pavlik harness is the most popular DDH treatment for children younger than 6 months. For older children, closed reduction with hip spica cast is the most preferable treatment. The maximum duration of first-line treatment has a broad range. The treatment of bilateral DDH varies widely among surgeons.
Conclusion:
This study shows clearly that paediatric orthopaedic surgeons do not agree on the diagnosis and treatment protocol of DDH, hence different approaches to this common disease are practised. The lack of an international guideline should motivate paediatric orthopaedic surgeons to discuss and formulate a uniform and evidence-based protocol for the diagnosis and treatment of DDH.
Introduction
Developmental dysplasia of the hip (DDH) encompasses a broad spectrum of anatomical hip abnormalities ranging from fixed irreducible dislocation to subtle dysplasia. 1 DDH is one of the most prevalent musculoskeletal conditions in young adults and is the leading cause of hip osteoarthrosis in this age group. 2 The worldwide incidence of DDH ranges from 1 to 34 cases per 1000 births. 3 The wide range of incidence can be attributed to different methods of diagnosis, timing of evaluation, definition of DDH, clinical experience of reporting physicians and the true variation in incidence that is attributed to genetics and environmental factors. 3,4 In addition, lack of agreement in the screening regimes of neonates worldwide contributes to the wide variation in incidence. 5
All newborns should be screened for DDH by neonatal hip screening physical examination. 6,7 If physical examination is doubtful or if there is an associated risk factor, ultrasonography should be used to confirm or exclude the diagnosis in children younger than 3 months and pelvic radiographs for older children. 8,9 The goal of DDH treatment is to obtain and maintain a safe concentric reduction of the hip in order to provide an optimal environment for the development of the femoral head and acetabulum, avoid avascular necrosis (AVN) and reduce the risk of early osteoarthrosis. 10 –12 Initially, DDH is treated conservatively with the use of Pavlik harness in children younger than 6 months. 13 If reduction was not attained or the infant presented late, surgical intervention (including closed or open reduction with or without pelvic osteotomy) followed by hip spica cast may be required. 3
The lack of uniformly accepted guidelines or standard practice for diagnosis and treatment of DDH is a major deficiency in DDH management. 14 The objective of this study is to investigate the current practice of paediatric orthopaedic surgeons in DDH management worldwide and identify points of agreement and disagreement.
Methods
This is an online cross-sectional study where a questionnaire was distributed to 200 paediatric orthopaedic surgeons who were identified by searching relevant literature on PubMed search engine. The participants were sampled using electronic survey tool (Survey Monkey). The electronic questionnaire composed of 28 close-ended multiple-choice questions. The electronic questionnaire was sent to the participants by e-mail. Non-responders were reminded by e-mail then post.
The questionnaire focused mainly on three aspects: demographics, diagnosis and treatment. For demographic aspects: We asked about the duration of practice as a paediatric orthopaedic staff and place of current practice, which was categorized into four geographical regions: Arabian Gulf, North America, Europe and others (mainly Asia and Africa). We also asked about the duration of surgical practice and the type of hospital they work in.
Regarding diagnosis, we asked about the imagining of choice for children of different age groups. We also asked about the tools and measurements they use to determine the need for pelvic osteotomy with the possibility of choosing more than one answer.
Regarding treatment, we asked about mode of treatment they would use as a first-choice treatment for dysplasia, subluxation and dislocation in children less than 6 months and between 6 months and 12 months of age and the maximum duration of use for the first-choice treatment. We also asked about the maximum age that they would surgically treat a child with unilateral or bilateral DDH. Moreover, we asked about the preferred age to do hip open reduction, pelvic osteotomy and femoral shortening. Finally, we asked about their approach to bilateral DDH cases that need open reduction and/or pelvic osteotomy.
Statistical analysis was performed using Statistical Package for the Social Sciences (SPSS) version 24 (IBM Corp., Armonk, NY, USA). Descriptive statistics were presented using percentages and frequencies. Chi-square and Fisher’s exact tests were used to assess differences in categorical data between different groups (geographical regions). Two-sided p values less than 0.05 were considered statistically significant.
Results
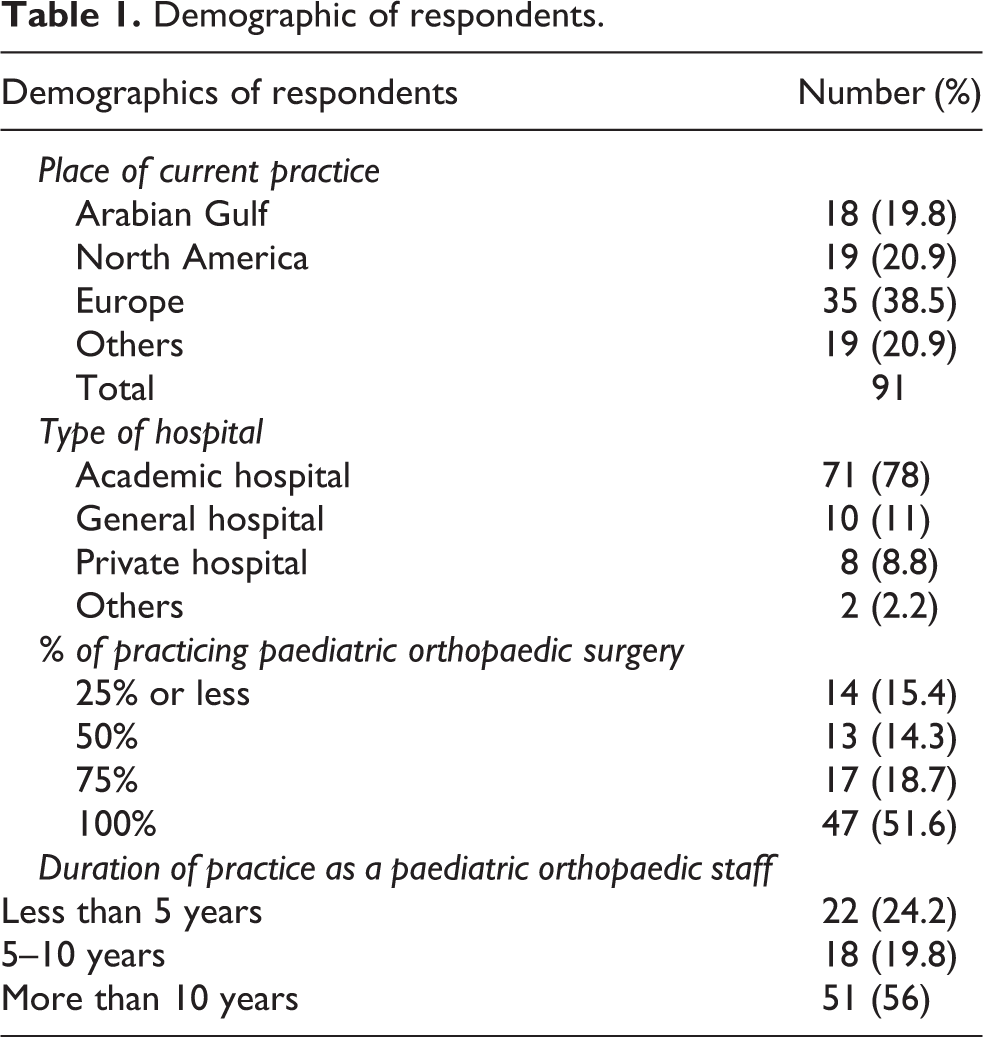
There were 91 respondents with a response rate of 45.5%. They were from the four regions: Arabian Gulf (n = 18), North America (n = 19), Europe (n = 35) and others (n = 19). Out of the 91 respondents, 64 (70.3%) treat children 75% or more of their time. More than half of respondents (56%) have more than 10 years of experience in paediatric orthopaedic surgery. Of the respondents, 71 (78%) were employed by an academic hospital (Table 1).
Demographic of respondents.
Ultrasonography is used by 83.5% of respondents and pelvic radiographs by 2.2%, while 14.3% use both ultrasonography and pelvic radiographs to diagnose DDH in children less than 3 months of age. For children over 3 months, pelvic radiographs are used by 42.9%, ultrasonography by 17.6% and both ultrasonography and pelvic radiographs by 39.6%.
As it was possible to answer with more than one imaging modality, 98.9% of respondents use pelvic radiographs as the imaging modality of choice to determine the need for pelvic osteotomy. Less than half (38.5%) use hip arthrogram. Few surgeons use advanced imaging modalities such as computed tomography (CT) (13.2%) or magnetic resonance imaging (MRI) (6.6%). With the ability to choose more than one answer, 94.5% of respondents use acetabular index (AI) as the imaging index of choice when interpreting hip imaging to determine the need for pelvic osteotomy, while 42.9% use centre edge angle, 36.3% use general morphology and 38.5% use disturbed Shenton’s line.
Pavlik harness was found to be the treatment of choice in children younger than 6 months of age with hip dysplasia (79.3%), while in older children, 40.7 and 37.4% of respondents use closed reduction with hip spica cast and rigid hip abduction, respectively (Table 2). Pavlik harness is used by 68.1% of respondents as the first-line treatment for subluxation in children younger than 6 months of age. In older children, closed reduction with hip spica cast is considered the first-line treatment for hip subluxation by 78% of respondents. Pavlik harness is considered the treatment modality of choice for hip dislocation in infants younger than 6 months by 65.9% of respondents. Closed reduction with hip spica cast is used as the first-line treatment for older children with hip dislocation by 78% of respondents. Almost half of the respondents wait maximally 3 months or less for the first-line treatment regardless of the severity of the condition (Tables 3 and 4).
Options of treatment in regards to the type of DDH and age of the patient.

DDH: Developmental dysplasia of the hip.
Maximum duration of use first choice mode of treatment in child <6 months of age with DDH.

DDH: Developmental dysplasia of the hip.
Maximum duration of use for first choice mode of treatment in a child 6–12 months of age with DDH.

DDH: Developmental dysplasia of the hip.
Respondents were asked up to which age they would use Pavlik harness in case of hip dislocation. More than half of respondents (60.4%) use Pavlik harness till 6 months of age, 20.5% till 3 months and surprisingly 8.8% till 1 year or more.
Half of the respondents (52.7%) would surgically intervene beyond the age of 7 years to treat a child with unilateral DDH, while 13.2 and 29.7% will stop operating at 5 and 7 years of age, respectively. In case of bilateral DDH, 39.6% of respondents will not operate after 5 years of age, while 31.9% will stop at 7 years and 25.3% at more than 7 years.
Regarding the earliest age at which hip open reduction and pelvic osteotomy are performed, only 7.7% of respondents would do them at 12 months of age, while 44% at 18 months and 48.4% at more than 18 months. Regarding the earliest age at which hip open reduction, pelvic osteotomy and femoral shortening are performed, almost half of the respondents (49.5%) stated that the decision is clinical and not based on age while 18.7% start at 2 years, 11% at 2.5 years and 19.8% at 3 years.
More than half of respondents (57.1%) stated that they would perform both hips open reduction at one stage for children with bilateral DDH. Of those who preferred to do open reduction at two stages (42.9%), 27.5% would do them at 2–4 weeks interval, 9.9% at 3 months interval and 5.5% at 6 months or more interval. Similarly, in regard to hip open reduction and pelvic osteotomy for a child with bilateral DDH, only 28.6% respondents preferred to perform both hips at one stage, while the majority (71.4%) preferred to perform them at two stages; 31.9% at 2–4 weeks interval, 27.5% at 3 months interval and 12.1% at 6 months or more interval.
Discussion
There is a general consensus that early diagnosis of DDH improves treatment results and decreases the risk of complications. 15 –17 The diagnosis and treatment options of DDH are not governed by internationally accepted guidelines or algorithm, also there is a substantial uncertainty regarding the method, timing and duration of treatment of DDH. 18 Lack of evidence-based studies, personal conviction and tradition play a major role in the variation of opinions in DDH diagnosis and treatment. 19
Literature reports that ultrasonography is the most reliable tool in describing the anatomical features of children’s hips younger than 3 months of age. 8,20 This fact was clearly shown in the response of the surgeons to this study as the majority of respondents (97.8%) use ultrasonography with/without pelvic radiography to diagnose DDH in children less than 3 months of age. However, pelvic radiography is still considered the most important imaging modality for children older than 3 months of age due to the fact that the ossification centres of normal femoral heads only appear at the age of 4–6 months. 21 This was also noted in the response of surgeons in this study as 82.5% of respondents use pelvic radiography with/without ultrasonography to diagnose DDH in children older than 3 months. This may explain why the vast majority of surgeons use radiography (98.9%) and AI (94.5%) as the most important radiological tool and measurement, respectively, to determine the need for pelvic osteotomy. Interestingly, 36.6% of respondents use general morphology (acetabular morphology) as an indication for surgery. Few surgeons use CT (13.2%) and MRI (6.6%) as the most important tools to determine the need for pelvic osteotomy although their advantages are not well established. 22,23 However, this may be explained by the fact that CT scan can help in localizing the location and magnitude of acetabular deficiency, hence determining the best osteotomy type (Pemberton or Salter osteotomy for anterior-superior deficiency and Dega osteotomy for superior or posterosuperior deficiency). 22,24 However, CT scan carries high radiation burden that can be avoided with other imaging techniques. On the other hand, MRI is an attractive imaging modality as it visualizes soft tissue structures (acetabular rim, cartilage and labrum) and it is radiation free. The main disadvantages of MRI are the need for sedation, the high cost and usually a long waiting list. 24
Considerable uncertainty is found in the literature regarding the optimal treatment of DDH. However, an accepted sequence of treatment options with gradual increase in invasiveness has been followed largely worldwide. Pavlik harness remains the most commonly used device to treat DDH in children younger than 6 months with high success rates. 25 If Pavlik harness failed to achieve stable reduction, closed reduction and hip spica cast application under general anaesthesia should be performed with or without arthrogram. If closed reduction failed, surgical options including open reduction alone or with pelvic osteotomy and with or without femoral shortening should be considered. 3 However, this study shows that not all surgeons are following this sequence. Almost one-third of respondents do not apply Pavlik harness as the first-line treatment modality for children less than 6 months of age with any grade of DDH spectrum. Likely, children between 6 months and 12 months of age are being treated differently. Only 40.7% of respondents treat children with dysplasia with closed reduction; being more inclined to treat these children less invasively in comparison to 78 and 70.3% with subluxation and dislocation, respectively. The use of the Pavlik harness after the age of 6 months is not recommended by most authors. 26 Surprisingly, this study shows that 39.6% of respondents will still use Pavlik harness after the age of 6 months in case of hip dislocation. However, few studies reported that the use of Pavlik harness after the age of 6 months could be a successful and safe treatment for older children with mild hip dislocation (<Graf type IV, <Tönnis type 3), 27,28 though practically children of this age are usually stronger than the harness and keeping them in the harness is cumbersome. Traction was not considered as a first-line treatment for children older than 6 months of age except by 4.4% of respondents for all forms of DDH spectrum, it is clearly going out of fashion with time, as if this question was asked 20 years back the numbers would be much more. However, Kaneko et al. reported that gradual hip reduction using over-head traction is associated with high success rate and low risk of AVN for children older than 6 months of age. 29 In addition, there is a great variability regarding the maximum duration of use of first-line treatment of all types of DDH. However, almost 50% of respondents wait for 3 months or less for the first-line treatment for all forms of DDH spectrum before they proceed to the next option. Though it is not advisable to continue using Pavlik harness if reduction of a dislocated hip was not achieved by 3 weeks.
Typically, open reduction is often considered for children older than 18 months of age. 30 However, open reduction should be considered for all children who failed to achieve a stable concentric reduction of the hip joint by less invasive techniques regardless of the age. 31 More than half of the respondents (58.3%) prefer to do open reduction before the age of 18 months. Consistent with the literature, this study shows that the vast majority of the respondents (92.4%) start doing open reduction and pelvic osteotomy at the age of 18 months or more.
Literature shows a substantial variability regarding the age beyond which surgical treatment is contraindicated. 32,33 Subasi et al. 34 reported that surgical intervention before the age of 8 years for unilateral DDH and 5.5 years for bilateral DDH have better results than surgery after that age. Interestingly, this study shows that 47.3% of respondents do not surgically treat children with unilateral DDH beyond the age of 7 years. In addition, more than half of the respondents (57.2%) treat bilateral DDH at the age of 7 years or even older. Though it makes sense, if it was the opposite as unilateral cases are more disfiguring to the patient than bilateral cases, and in bilateral cases, there is always a risk of attaining different quality of reduction in the two sides, which leads to abnormal gait.
Generally, surgical treatment of bilateral DDH is more difficult and challenging than unilateral cases. For bilateral cases that need pelvic osteotomy, surgeons usually determine which hip is more severely affected through clinical examination and imaging to treat that hip first. After 2 months of immobilization in a hip spica cast, the contralateral hip is treated. 35 Unexpectedly, 28.6% of respondents prefer to do open reduction and pelvic osteotomy for bilateral DDH as one-stage surgery. This may be supported by few studies that suggested single-stage surgery has comparable outcomes to two-stage surgery with less duration of hospitalization, cost, anaesthetic exposure and blood transfusion volume. 32,36,37 However, 71.4% of respondents still prefer to perform them as two-stage surgery but they varied significantly in the interval duration between the two surgeries. Of the surgeons who would perform them as two-stage surgery, 55.4% wait 3 months or more between the two stages. The results of this study show the controversy regarding the treatment of DDH in the absence of evidence-based and well-studied guidelines and consensus.
Limitations
As any questionnaire-based study, this study has several limitations. Low response rate of 45.5% may increase the potential of response bias. The questionnaire is exclusively composed of close-ended questions without adding open fields for personal comments; leading to low level of details. However, this was considered as the best way to insure complete responses, which was clearly evident in the low number of incomplete responses (n = 15). Moreover, the sample was limited to paediatric orthopaedic surgeons whose e-mails were identified by searching relevant literature on PubMed search engine and with whom we were able to establish a contact. However, we were able to achieve a good worldwide variation with an acceptable overall number of respondents. A critical limitation can be noted when discussing operative treatment. Surgeons were asked what they would do, not what they did; as some hospitals’ protocols may limit their treatment choices.
Conclusion
The diagnosis and treatment of DDH is not subjected to an international consensus. This study shows clearly that worldwide paediatric orthopaedic surgeons do not agree on the diagnosis methods and treatment of DDH, hence different approaches are there for this one common disease. The lack of an internationally accepted guideline should motivate paediatric orthopaedic surgeons to discuss and formulate a uniform and evidence-based protocol for the diagnosis and treatment of DDH. It is clear that there is a need for more systematic reviews in all aspects of DDH management to come out with the guidelines.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.