
Abstract
Purpose:
The purpose of this study was to evaluate the current trends in the treatment of supracondylar humerus fractures as well as the preferred post-operative follow-up protocol among members of the European Paediatric Orthopaedic Society.
Methods:
The survey was composed by four main domains and 26 items: (1) surgeon information (3 items); (2) treatment (8 items); (3) post-operative treatment (3 items); and (4) factors influencing the outcome (12 items). All active members of European Paediatric Orthopaedic Society were invited by email to answer an electronic questionnaire.
Results:
The survey was submitted to 397 European Paediatric Orthopaedic Society active members; 184 members answered (46.3%) the questionnaire. Among respondents, 64.1% declared >10 years of experience and 55.4% declared to treat >20 supracondylar humerus fractures per year. Closed reduction, percutaneous pinning, and supine position were the preferred treatment option for Gartland type II and III supracondylar humerus fractures by 79.9%, 95.5%, and 84.8% of respondents, respectively. Supracondylar humerus fractures are treated within 24 h from trauma by 33.2% of respondents. Pins are removed 4 weeks from index procedure by 58.2% of respondents. Fracture type (72.3%), surgeon experience, and (71.2%) are of “crucial importance” for expected outcome of supracondylar humerus fractures treatment.
Conclusion:
Surgeon experience, type of fracture, treatment modality, and pins configuration were considered the main factors potentially influencing the outcome of supracondylar humerus fractures. European Paediatric Orthopaedic Society members agreed on the treatment modality of Gartland type II and III supracondylar humerus fractures, patient positioning, and timing of hardware removal. Other important issues such as timing of surgery, pins configuration, surgical approach, and post-operative protocol are still debated.
Level of evidence:
level II.
Keywords
Introduction
Supracondylar humerus fractures (SHFs) are the most prevalent injures affecting the child’s elbow, and represent the most common indication for surgery in children. 1 In particular, SHFs account for one-third of all fractures diagnosed in children younger than 8 years of age, and for up to one-fourth of all pediatric orthopedic surgical procedures. 2
Despite the frequency of SHFs in children, today there are no consensual guidelines, and often the choice of the type of treatment and fixation, the positioning of the patient, the timing of surgery and hardware removal, the length of post-operative immobilization, as well as clinical and radiographic follow-up, and the need of post-operative physiotherapy (PT) are reported to the individual surgeon.3–7 In addition, the treatment of SHFs can be challenging even in the hands of experienced surgeons, and the rate of complications related to this type of injury is not negligeable. 2
The modified Gartland’s classification is nowadays considered a useful guide for treatment of SHFs in children even though controversy still exists about the optimal approach for subtype IIA and IIB of SHFs.8–10 The difference between type IIA and IIB SHFs is related to the amount of rotation and translation of the distal fragment. In particular, type IIA SHFs are characterized by a displacement of 2–15 mm on the lateral or the anterior–posterior (AP) view and a 15°–20° retro-tilt on the lateral view with a partially intact posterior cortex, while type IIB SHFs, in addition to displacement and retro-tilt, also have a rotatory malalignment.11,12 Most type II SHFs fractures have been traditionally managed surgically. However, some authors agree that conservative treatment may be a valuable option in type IIA SHFs.11,12 The purpose of this study was to evaluate the current trends in the treatment of SHFs as well as the preferred post-operative follow-up protocol among members of the European Paediatric Orthopaedic Society (EPOS).
Material and methods
A web-based survey was designed by three EPOS members (V.P., G.T., and A.V.) and was distributed to all EPOS active members in October 2020, following EPOS Research & Scientific Committee and EPOS Board approval (see Appendix 1).
An email with a link to the survey, hosted by https://forms.office.com , was sent to 397 EPOS active members; moreover, at least one reminder email was sent to members not having responded to the questionnaire after the initial submission. The survey was composed by four main domains, for a total of 26 items: (1) surgeon information (3 items); (2) treatment (8 items); (3) post-operative treatment (3 items); and (4) factors influencing the outcome (12 items). In order to evaluate surgeons’ experience, the respondents were asked to specify the number of years in practice, number of SHFs treated per year, and the country of practice.
Concerning the treatment of SHFs, respondents were requested to specify their preferred treatment option for a given SHF, timing of surgery, patient positioning, and preferred surgical approach. The follow-up preferences were recorded in the post-operative treatment domain.
In the final section of the questionnaire (factors influencing the outcome), the respondents were asked to score each item from zero (least important) to three (most important): with zero figure corresponding to “not important at all,” one to “low importance,” two to “average importance,” and three to “crucial importance.” The questionnaire used for the survey is presented in Appendix 1 (see Appendix 1).
Statistical analysis
Responses were collected and entered into an Excel spreadsheet (Microsoft, Redmond, WA, USA). Statistical analysis was performed using the statistics package SPSS 27.0 (SPSS, Chicago, IL, USA). Data are expressed as numerical variables, frequencies and percentages, with the mean values and standard deviations. The threshold for statistical significance was set to a p-value less than 0.05.
Results
The survey was successfully submitted to 397 EPOS active members; 383 out of 397 EPOS members read the email (receivers; 96.5%), 214 clicked the link (readers; 53.9%), and 184 answered the questionnaire (respondents; 46.3%).
Demographics
According to the number of years in practice (YiP), respondents divided into three groups: Group 1: less than 5 years of practice (n = 35; 19.0%), Group 2: between 6 and 10 years of practice (n = 31; 16.8%), and Group 3: more than 10 years of practice (n = 118; 64.1%).
According to the number of SHFs treated per year (SHFpY), the responders were divided into four groups: Group A: less than 10 SHFs/year (n = 34; 19%), Group B: between 11 and 20 SHFs/year (n: 48; 26.1%), Group C: between 21 and 30 SHFs/year (n: 51; 27.7%), and Group D: 31 or more SHFs/year (n: 51; 27.7%). Overall, 79.3% (n = 146) of the respondents practice Pediatric Orthopedic Surgery in Europe, Israel, and Turkey, 7.1% in Asia (n = 13), 4.9% in Africa (n = 9), 8.2% in North and South America (n = 15), and 0.5% in Oceania (n = 1).
Treatment options
Concerning the treatment modality of Gartland II SHFs, 79.9% of the respondents (n = 147) preferred “closed reduction and percutaneous pinning” while the 15.2% answered “closed reduction and casting” (n = 28) (YiP: p = 0.97; SHFpY: p = 0.86) (Table 1).
Gartland’s type II and III treatment preferences.
SHFs: supracondylar humerus fractures.
Concerning the treatment modality of Gartland III SHFs, 95.5% (n = 175) of the respondents selected “closed reduction and percutaneous pinning” as preferred treatment option (YiP: p = 0.33; SHFpY: p = 0.52) (Table 1); 33.2% (n = 61), 26.1% (n = 48), and 20.1% (n = 37) designated of “within 24 h,” “within 12 h,” and “within 6 h” as the best timing for the surgical management of neurovascularly intact SHFs (YiP: p = 0.82; SHFpY: p = 0.31) (Table 2). The 59.2% of respondents (n = 109) perform surgery before midnight while they postpone it to the following morning if SHFs are admitted after midnight; however, 20.7% of respondents (n = 38) do surgery at any time of the night shift while 20.1% of participants (n = 37) delay surgical treatment of SHFs to the following morning (YiP: p = 0.64; SHFpY: p = 0.98). When surgery is postponed, 71.1% of respondents splint the patient, while 26.6% attempt to realign the fracture before splinting (YiP: p = 0.06; SHFpY: p = 0.86).
Surgical timing preferences.
SHFs: supracondylar humerus fractures.
If surgical treatment is required, patients are placed in supine position by 84.4% of respondents (n = 156) while prone positioning of the patient is preferred by 6% of respondents (n = 11) (YiP: p = 0.3; SHFpY: p = 0.15); 9.2% of respondents use both positions indifferently (n = 17). If open reduction is needed, 40.8% (n = 75), 25.5% (n = 47), and 14.7% (n = 27) perform a lateral, anterior, and posterior approach, respectively (YiP: p = 0.61; SHFpY: p = 0.001) (Table 3).
Patient position, pinning configuration, and surgical approach preferences.
SHFs: supracondylar humerus fractures.
Displaced SHFs requiring surgery are stabilized by two crossed pins in 33.7% of cases (n = 62), by two divergent lateral pins in 23.9% of cases (n = 44), by three lateral pins in 11.4% of cases (n = 21), and by one medial pin and two lateral pins in 15.8% of cases (n = 29) (YiP: p = 0.6; SHFpY: p = 0.4) (Table 1).
Post-operative protocol and follow-up
The survey recorded a maximum of four post-operative AP and lateral elbow radiographs during follow-up period (range = 1–4); in particular, 64.13% (n = 118) of the respondent perform AP and lateral elbow radiographs once, 29.9% (n = 55) twice, 5.4% (n = 10) three times, and 0.5% (n = 1) four times during follow-up (YiP: p > 0.05; SHFpY: p > 0.05) (Figure 1). The first set of radiographs is performed at 1 week post-operative in 46.2% (n = 85) of cases, while the second radiographic check is performed at 2 and 3 weeks post-operative by 15.2% (n = 28) and 14.1% (n = 26) of respondents, respectively. Two percent (n = 4) perform a third radiographic evaluation at 6 weeks post-surgery.
Post-operative X-ray follow-up schedular: (a) weeks for the first follow-up, (b) N weeks for the second follow-up, (c) weeks for the third follow-up, and (d) weeks for the fourth follow-up.
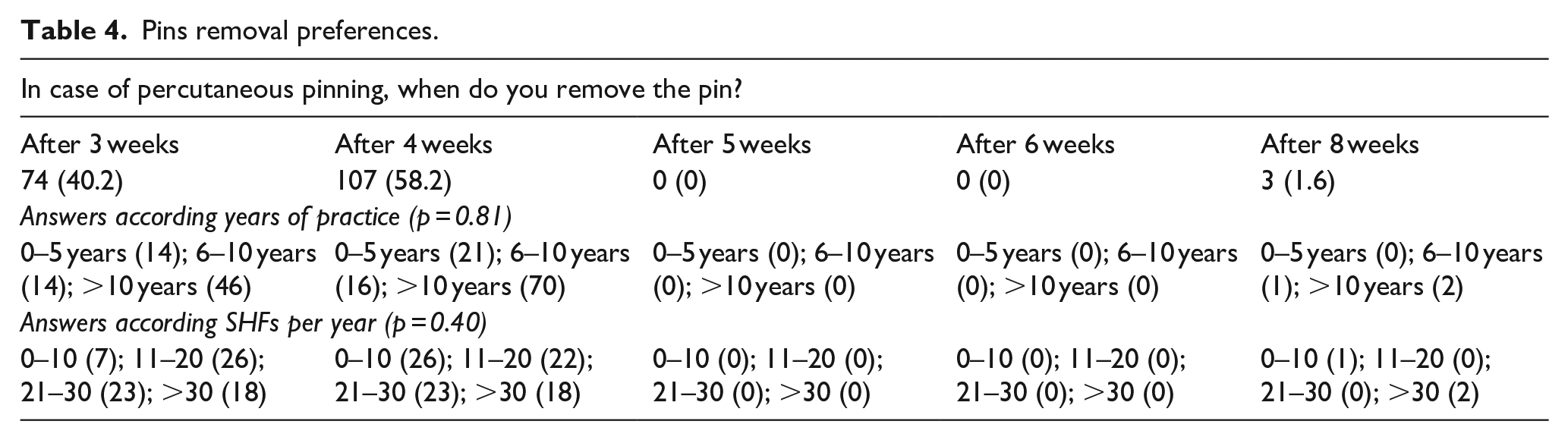
Pins are removed 4 weeks after the index procedure in 58.2% of cases (n = 107) while the 40.2% (n = 14) of respondent remove the hardware 3 weeks after the surgery (Table 4) (YiP: p = 0.81; SHFpY: p = 0.4). Following pins removal, all respondents require a radiographic assessment of the elbow; 9.8% (n = 18) and 6% (n = 11) of the respondents perform a second and third radiographic check during follow-up, respectively (YiP: p > 0.05; SHFpY: p > 0.05) (Figure 2).
Pins removal preferences.
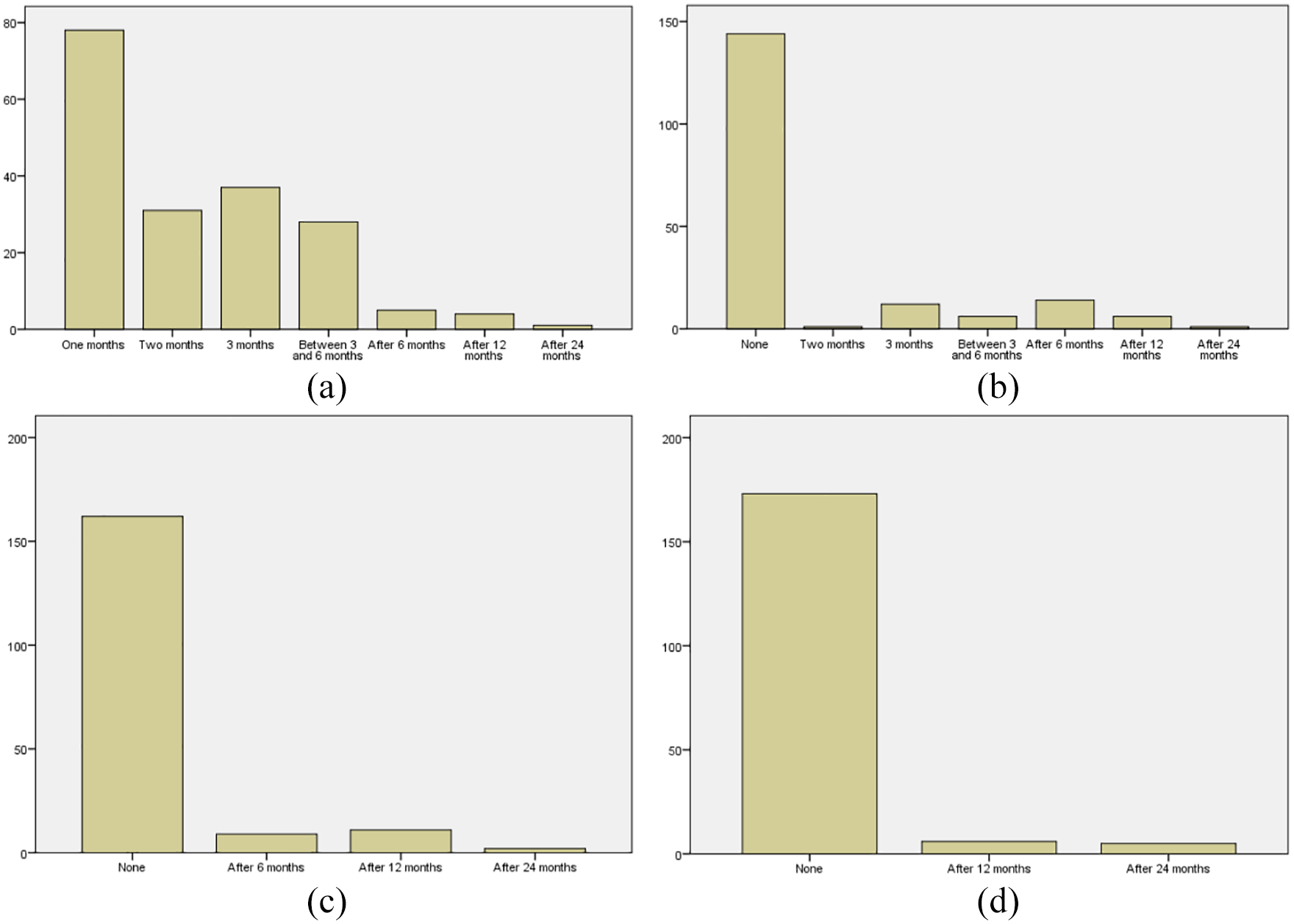
Post-pins removal X-ray follow-up schedular: (a) weeks for the first follow-up, (b) N weeks for the second follow-up, (c) weeks for the third follow-up, and (d) weeks for the fourth follow-up.
Factors influencing the outcome
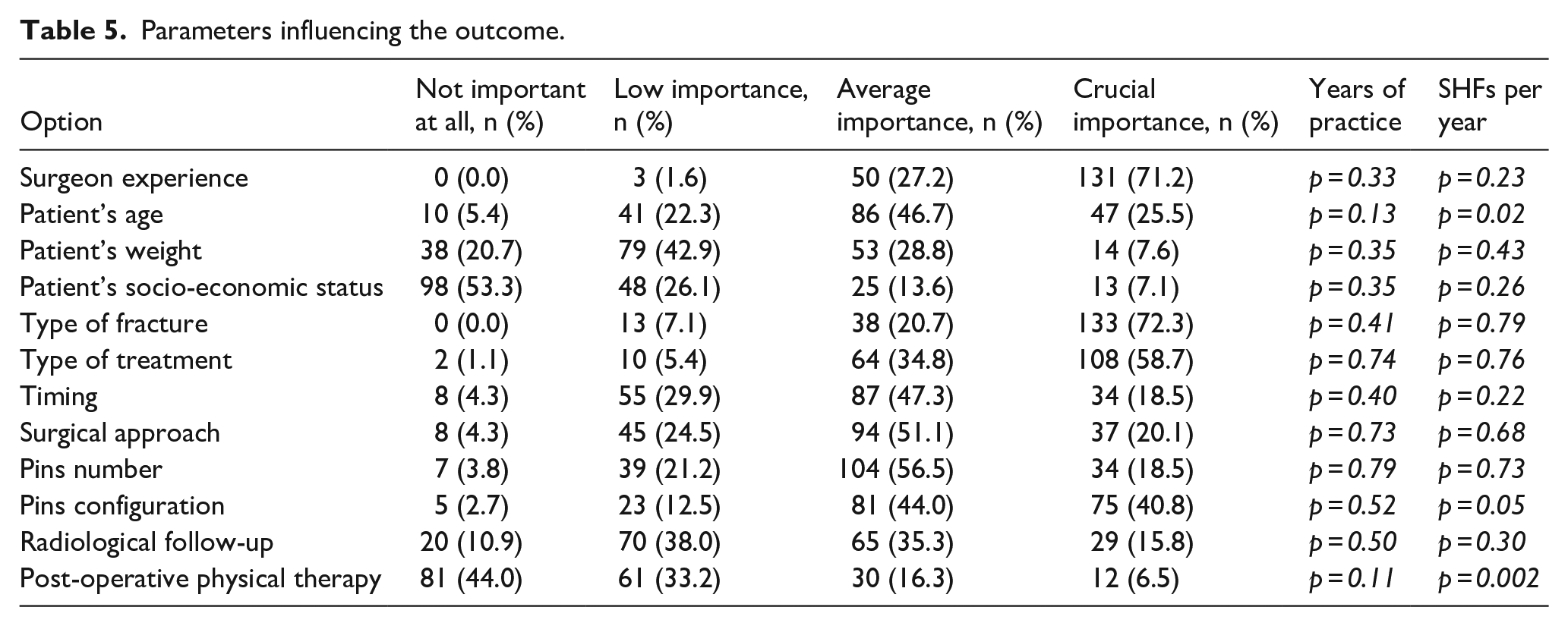
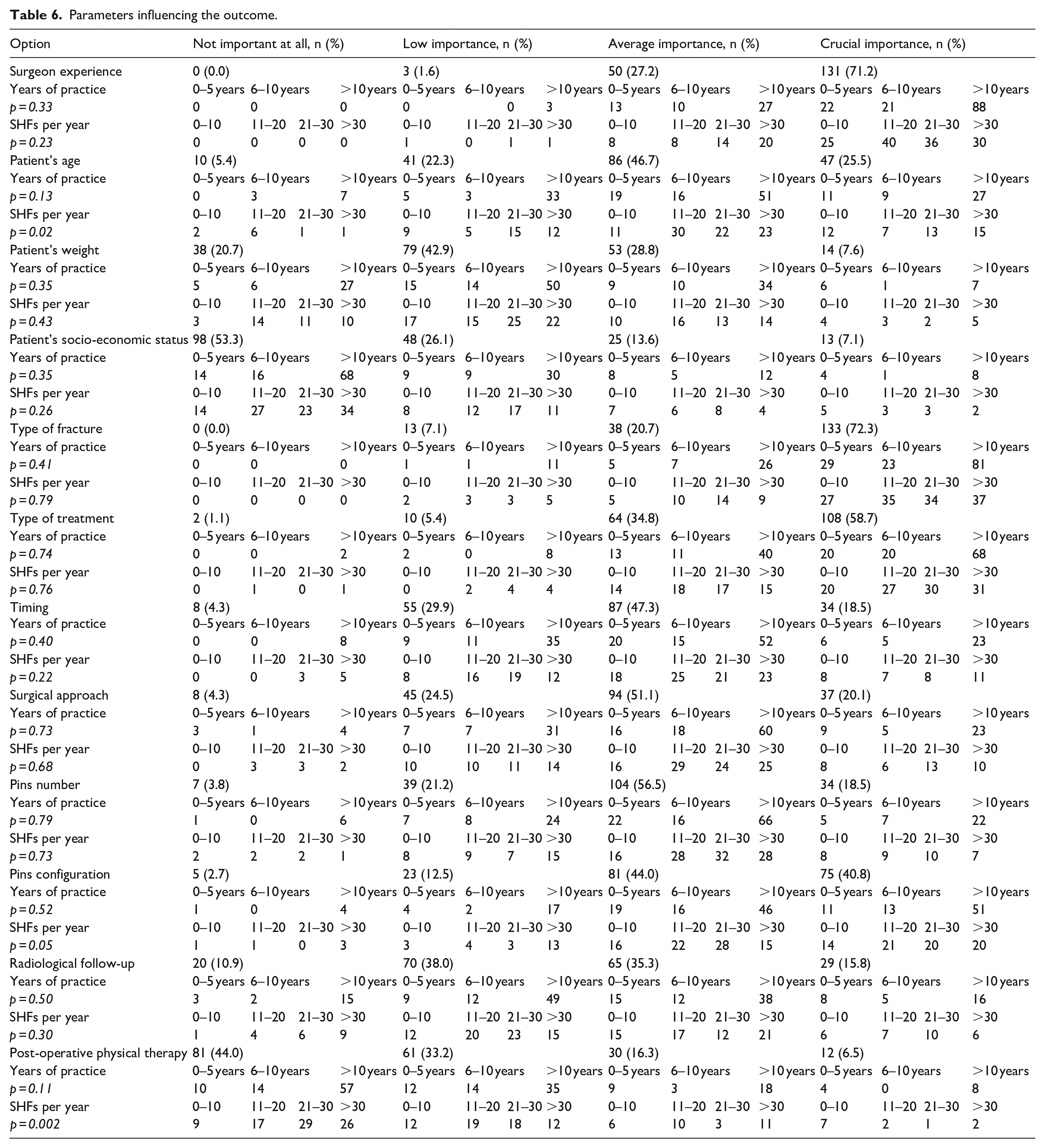
Among respondents, 72.3% (n = 133) (YiP: p = 0.41; SHFpY: p = 0.79) rated fracture type as of “crucial importance” for expected outcome of SHFs treatment, followed by surgeon experience (71.2%; n = 131) (YiP: p = 0.33; SHFpY: p = 0.23), type of treatment (58.7%; n = 198) (YiP: p = 0.74; SHFpY: p = 0.79), pin configuration (40.8%; n = 75) (YiP: p = 0.52; SHFpY: p = 0.05), patients’ age (25.5%, n = 47) (YiP: p = 0.13; SHFpY: p 0.02), surgical approach (20.1%; n = 37) (YiP: p = 0.73; SHFpY: p = 0.68), number of pins (YiP: p = 0.79; SHFpY: p = 0.73) and timing of surgery (YiP: p = 0.4; SHFpY: p = 0.22) (18.5%; n = 34), radiographic follow-up (15.8%; n = 29) (YiP: p = 0.5; SHFpY: p = 0.3), patients’ weight (7.6%; n = 14) (YiP: p = 0.35; SHFpY: p = 0.43), socio-economic status of the patient (7.1%; n = 13) (YiP: p = 0.35; SHFpY: p = 0.26), and post-operative physical therapy (6.5%; n = 12) (YiP: p = 0.11; SHFpY: p = 0.002) (Tables 5 and 6).
Parameters influencing the outcome.
Discussion
The 2020 EPOS SHFs questionnaire received the highest response rate (46.3%) among EPOS surveys; in fact, most of the previous questionnaires received a variable response rate, between 23% and 43%.13–17 Concerning the previously published SHFs surveys from other scientific societies, they reported limited evidence, focused on specific fracture patterns only, did not detail the post-operative protocol, and in some cases were limited to a restricted cohort of a nation cohort.2,7,18,19 The 2020 EPOS SHFs survey provided data on the management and follow-up of SHFs from more than 20 countries. Surgeon experience, type of fracture, and pins configuration were the main factors influencing the outcome of SHFs in children.
Gartland’s type II SHFs represent a relatively broad spectrum of lesions ranging from mildly extended fractures to fractures with coronal and/or rotatory malalignment, and controversy regarding their management exists. Most type II SHFs are treated surgically by the large majority of respondents although 15% agree that closed reduction and casting is a valuable option in this sub-group of patients.20,21 Moraleda et al. 22 reported type II SHFs treated conservatively tend to develop mild cubitus varus and mild increase in elbow extension. O’Hara et al. 23 recommended conservative treatment in type IIA and Kirschner wire fixation in type IIIB fractures. Similarly, Ariyawatkul et al. 24 suggest surgical treatment for type IIB fractures and found that if the lateral capitellar-humeral angle difference or the shaft condylar angle difference from the uninjured side is less than 18°, type IIA fractures are stable enough to be treated by cast immobilization. In contrast, Pham et al. 25 reported excellent results in type IIB SHFs treated with Blount’s technique.
Gartland’s type III SHFs are managed by closed reduction and percutaneous pinning in most cases. Present evidence suggests that delaying surgery by up to 3 days from injury in closed supracondylar humeral fractures without neurovascular injury is safe and does not significantly increase the risk of peri- and post-operative complications, or the need for open reduction. 26 However, clear guidelines regarding timing of surgery are not available due to the lack of high-quality trials.
Despite the fact that timing of surgery was considered to be of “average” or “crucial importance” by almost two-third of the respondents, our data are not conclusive, and the only clear information concerns the preference of treating SHFs within 24 h from injury. About 60% of respondents postpone surgery to the next day if patients are admitted after midnight; this percentage rises to 80% if surgeons postponing to the next days all fractures admitted during the night shift are added. This approach is supported by the literature; in fact, pinning errors have been found to be more frequent in surgeries performed at night, 27 probably due to inadequate facilities or staff. 27 When surgery is postponed, the use of skin or trans-skeletal traction is avoided by 98.3% of the EPOS members, who prefer to splint the fracture with (26.6%) or without (71.7%) a preliminary closed reduction.
Another highly debated issue is the positioning of the patient. Presently, the evidence supporting prone versus supine positioning is scarce, and of limited evidence.28,29 The choice of position is based on surgeon experience, and prone position been shown to facilitate reduction, to use the C-arm more easily, and to reduce the rate of iatrogenic nerve injury.30,31 However, it could make upper airways management, as well as treatment of polytrauma patients, more difficult; in addition, when the exposure of the antecubital fossa is needed for reduction or neurovascular exploration, the patient should be repositioned. 32 However, only 11 out of 184 (6%) respondents declared to position the patient prone, while 17 (9.2%) declared to perform the operation with the patient in this position only in selected cases. With 84.8% of the preference, the supine position was the preferred one because is quicker, it allows for standard anesthesia management and it gives the possibility to perform an anterior, anteromedial, or anterolateral approach, if conversion to open reduction is required. 28 Following fracture reduction, in patients supine, the elbow is locked in hyperflexion and external rotation, and this could result in loss of reduction, increase of forearm compartment pressure, and anterior displacement of the ulnar nerve. 32
Pins configuration and pin number were considered “average” or “crucial” factors in the management of SHFs by 84.8% and 75% of the respondents, respectively. Nevertheless, no clear preference was revealed by the survey about pin configuration as crossed pins (33.7%) and two divergent lateral (23.9%) pins were mostly done. This result reflects the uncertainty of the literature with several biomechanical33–36 and clinical37–39 studies reporting the superiority of a pin configuration over the others. Crossed pinning has been found to be the most stable configuration in different fracture patterns,33–36 especially when three k-wire (two lateral and one medial) are used; 33 however, a recent metanalysis 39 reported 4.9% of iatrogenic ulnar nerve injury in crossed pinning, but the performance of safe procedure for the medial pin 40 can significantly reduce the risk of injuring the nerve.37,38 To avoid ulnar nerve injury, lateral pinning is the preferred fixation technique by 50% of respondents; in particular, most surgeons use two lateral pins (38.6%) and the remaining three (11.4%).
Open reduction is indicated when closed reduction is not possible due to issue entrapment (i.e. muscle, median nerve, brachial artery), compartment syndrome, and neurologic and/or vascular injury.27,41 When conversion to open reduction is required, most respondents (40.8%) select the lateral approach although it does not show any advantage over the anterior approach, and it does increase both the risk of injuring the radial nerve and the risk of elbow stiffness. 27 It was described that posterior and lateral approaches had higher rates of cubitus varus, while medial and lateral approaches restrict joint motion less than posterior approaches. 42 In an interesting instructional course, Kzlay et al. suggested to use a surgical approach according to the location of the metaphyseal spike and the displacement of the distal fragment; this approach allows direct visualization of anatomic structures trapped or displaced by the metaphyseal spike. 42
Almost the entire sample declared to remove pins between 3 (40.2%) or 4 (58.2%) weeks after the initial surgery. As for the follow-up, the survey did not provide any clear indication, and it is highly likely that every surgeon or every institution adopts a specific protocol.
Ninety-five percent of the respondents require post-operative elbow radiographs, and half of them performs a radiographic check 1 week after surgery. In order to limit exposure to radiation, expenses and time away from work for caregivers, Mansor et al. 43 recommend to carry out a single radiographic check 1 week after the surgery, in case the risk of loss of reduction is high (engagement of fragments, bi-cortical engagement, and pins crossing at the fracture site); when adequate fixation is obtained intraoperatively, the radiographic check is recommended after 3–4 weeks, at the time of hardware removal. All respondents unanimously require AP and lateral elbow radiographs at the time of pins removal; in particular, one-third request additional radiographs 1 month or more after hardware removal.
Only the 22.8% of the respondents believe PT can influence the outcome of SHFs. Several authors did not report any benefit from a short course of PT on elbow function or motion.44–46 Recently, two pilot trials47,48 analyzed the benefits of video gaming in restoring normal elbow function and in reducing pain after conservative or surgical treatment. In particular, tennis, boxing, and bowling gaming could shorten recovery time, 48 and should be considered in the holistic management of elbow injuries. 47
This study carries some limitations. First, the surveys gathered answers from EPOS members only. Second, surgeons of different age and different level of expertise responded to the survey; moreover, the comparison between European and not-European members were not performed as the differences between national health systems could induce a selection bias. In addition, the survey may include answers from surgeons not treating SHFs on a regular basis. Finally, the survey can report the surgeons’ answers in a hypothetical case, but not what they effectively perform in their everyday practice. Despite such limitations, the survey had an excellent response rate of 46.3% higher than most other surveys.13–17
In conclusion, surgeon experience, type of fracture, treatment modality, and pins configuration were indicated as the main factors influencing the outcome of SHFs. EPOS members agreed on the treatment modality of Gartland’s type II and III SHFs, patient positioning, and timing of hardware removal. Other important issues such as timing of surgery, pins configuration, surgical approach, and post-operative protocol are still debated. Post-operative PT is not considered necessary by a large majority of respondents.
Footnotes
Appendix 1
Parameters influencing the outcome.
| Option | Not important at all, n (%) | Low importance, n (%) | Average importance, n (%) | Crucial importance, n (%) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Surgeon experience | 0 (0.0) | 3 (1.6) | 50 (27.2) | 131 (71.2) | ||||||||||||
| Years of practice | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | ||||
| p = 0.33 | 0 | 0 | 0 | 0 | 0 | 3 | 13 | 10 | 27 | 22 | 21 | 88 | ||||
| SHFs per year | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 |
| p = 0.23 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 8 | 8 | 14 | 20 | 25 | 40 | 36 | 30 |
| Patient’s age | 10 (5.4) | 41 (22.3) | 86 (46.7) | 47 (25.5) | ||||||||||||
| Years of practice | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | ||||
| p = 0.13 | 0 | 3 | 7 | 5 | 3 | 33 | 19 | 16 | 51 | 11 | 9 | 27 | ||||
| SHFs per year | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 |
| p = 0.02 | 2 | 6 | 1 | 1 | 9 | 5 | 15 | 12 | 11 | 30 | 22 | 23 | 12 | 7 | 13 | 15 |
| Patient’s weight | 38 (20.7) | 79 (42.9) | 53 (28.8) | 14 (7.6) | ||||||||||||
| Years of practice | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | ||||
| p = 0.35 | 5 | 6 | 27 | 15 | 14 | 50 | 9 | 10 | 34 | 6 | 1 | 7 | ||||
| SHFs per year | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 |
| p = 0.43 | 3 | 14 | 11 | 10 | 17 | 15 | 25 | 22 | 10 | 16 | 13 | 14 | 4 | 3 | 2 | 5 |
| Patient’s socio-economic status | 98 (53.3) | 48 (26.1) | 25 (13.6) | 13 (7.1) | ||||||||||||
| Years of practice | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | ||||
| p = 0.35 | 14 | 16 | 68 | 9 | 9 | 30 | 8 | 5 | 12 | 4 | 1 | 8 | ||||
| SHFs per year | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 |
| p = 0.26 | 14 | 27 | 23 | 34 | 8 | 12 | 17 | 11 | 7 | 6 | 8 | 4 | 5 | 3 | 3 | 2 |
| Type of fracture | 0 (0.0) | 13 (7.1) | 38 (20.7) | 133 (72.3) | ||||||||||||
| Years of practice | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | ||||
| p = 0.41 | 0 | 0 | 0 | 1 | 1 | 11 | 5 | 7 | 26 | 29 | 23 | 81 | ||||
| SHFs per year | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 |
| p = 0.79 | 0 | 0 | 0 | 0 | 2 | 3 | 3 | 5 | 5 | 10 | 14 | 9 | 27 | 35 | 34 | 37 |
| Type of treatment | 2 (1.1) | 10 (5.4) | 64 (34.8) | 108 (58.7) | ||||||||||||
| Years of practice | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | ||||
| p = 0.74 | 0 | 0 | 2 | 2 | 0 | 8 | 13 | 11 | 40 | 20 | 20 | 68 | ||||
| SHFs per year | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 |
| p = 0.76 | 0 | 1 | 0 | 1 | 0 | 2 | 4 | 4 | 14 | 18 | 17 | 15 | 20 | 27 | 30 | 31 |
| Timing | 8 (4.3) | 55 (29.9) | 87 (47.3) | 34 (18.5) | ||||||||||||
| Years of practice | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | ||||
| p = 0.40 | 0 | 0 | 8 | 9 | 11 | 35 | 20 | 15 | 52 | 6 | 5 | 23 | ||||
| SHFs per year | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 |
| p = 0.22 | 0 | 0 | 3 | 5 | 8 | 16 | 19 | 12 | 18 | 25 | 21 | 23 | 8 | 7 | 8 | 11 |
| Surgical approach | 8 (4.3) | 45 (24.5) | 94 (51.1) | 37 (20.1) | ||||||||||||
| Years of practice | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | ||||
| p = 0.73 | 3 | 1 | 4 | 7 | 7 | 31 | 16 | 18 | 60 | 9 | 5 | 23 | ||||
| SHFs per year | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 |
| p = 0.68 | 0 | 3 | 3 | 2 | 10 | 10 | 11 | 14 | 16 | 29 | 24 | 25 | 8 | 6 | 13 | 10 |
| Pins number | 7 (3.8) | 39 (21.2) | 104 (56.5) | 34 (18.5) | ||||||||||||
| Years of practice | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | ||||
| p = 0.79 | 1 | 0 | 6 | 7 | 8 | 24 | 22 | 16 | 66 | 5 | 7 | 22 | ||||
| SHFs per year | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 |
| p = 0.73 | 2 | 2 | 2 | 1 | 8 | 9 | 7 | 15 | 16 | 28 | 32 | 28 | 8 | 9 | 10 | 7 |
| Pins configuration | 5 (2.7) | 23 (12.5) | 81 (44.0) | 75 (40.8) | ||||||||||||
| Years of practice | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | ||||
| p = 0.52 | 1 | 0 | 4 | 4 | 2 | 17 | 19 | 16 | 46 | 11 | 13 | 51 | ||||
| SHFs per year | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 |
| p = 0.05 | 1 | 1 | 0 | 3 | 3 | 4 | 3 | 13 | 16 | 22 | 28 | 15 | 14 | 21 | 20 | 20 |
| Radiological follow-up | 20 (10.9) | 70 (38.0) | 65 (35.3) | 29 (15.8) | ||||||||||||
| Years of practice | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | ||||
| p = 0.50 | 3 | 2 | 15 | 9 | 12 | 49 | 15 | 12 | 38 | 8 | 5 | 16 | ||||
| SHFs per year | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 |
| p = 0.30 | 1 | 4 | 6 | 9 | 12 | 20 | 23 | 15 | 15 | 17 | 12 | 21 | 6 | 7 | 10 | 6 |
| Post-operative physical therapy | 81 (44.0) | 61 (33.2) | 30 (16.3) | 12 (6.5) | ||||||||||||
| Years of practice | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | 0–5 years | 6–10 years | >10 years | ||||
| p = 0.11 | 10 | 14 | 57 | 12 | 14 | 35 | 9 | 3 | 18 | 4 | 0 | 8 | ||||
| SHFs per year | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 | 0–10 | 11–20 | 21–30 | >30 |
| p = 0.002 | 9 | 17 | 29 | 26 | 12 | 19 | 18 | 12 | 6 | 10 | 3 | 11 | 7 | 2 | 1 | 2 |
Acknowledgements
The authors thank all EPOS members answering to the survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.