
Abstract
Purpose:
We aimed to evaluate the influence of the bony morphology of the bicipital groove on the stability of the long head of the biceps tendon (LHBT).
Methods:
Among the patients who underwent magnetic resonance imaging of the shoulder at our outpatient clinic in 2012, those aged >40 years were included. After excluding cases with complete tear or unclear positioning of the biceps tendon, 464 shoulders were analyzed according to the position of the LHBT with respect to the bicipital groove. Shoulders with subluxation or dislocation of the LHBT were labeled as having unstable LHBT, while those with the LHBT located in the bicipital groove were labeled as having stable LHBT. The bony morphology of the bicipital groove was measured in terms of opening angle, medial wall angle, and depth. A shallow bicipital groove was defined as having an opening angle >94°, concurrent with earlier studies. We compared shoulders with stable and unstable LHBT regarding bicipital bony morphology. We also compared shoulders with normal and shallow grooves regarding tendon stability.
Results:
Shoulders with stable and unstable LHBT differed significantly regarding bony morphology. Shoulders with unstable LHBT showed a shallower mean depth (by 0.3 mm; p = 0.008), a smaller mean medial angle (by 2.2°; p = 0.014), and a larger mean opening angle (by 3.7°; p = 0.016). Bony morphology characterized by a shallow groove was significantly associated with increased prevalence of instability defined as LHBT subluxation or dislocation (p = 0.011).
Conclusion:
A shallow bicipital groove, identified by the larger opening angle, smaller medial angle, and shallower depth, may represent a predisposing factor for biceps tendon instability.
Introduction
The long head of the biceps tendon (LHBT) originates from the superior labrum with an intra-articular course, then courses through the groove of the biceps before joining with the short head tendon. There is a consensus that the long head tendon can be a source of pain and significant dysfunction. 1 The LHBT can be affected by pathologies such as tendinitis, rupture, and instability, and the latter of which can manifest as subluxation or dislocation and is typically suspected as the source of pain and dysfunction. 2 While stabilization during tendon excursion is mostly ensured by soft tissue restraints such as the superior glenohumeral ligament, coracohumeral ligament, and tendons of the subscapularis and supraspinatus, which are considered to be the main stabilizers, it has been shown that the contours of the bicipital tuberosities help to contain the LHBT within the groove. 3 However, the relationship between the morphology of the bicipital groove and LHBT instability is not yet fully understood. 1
The significance of the morphology of the bicipital groove was debated in previous reports, but no consensus has been reached to date. 4 –7 During suture anchor tenodesis in the bicipital groove, 8 diverse morphology of the groove could be noted, with some grooves appearing relatively shallow. These shallower grooves often exhibited biceps tendon subluxation, raising the question of whether the depth of the bicipital groove has any relationship with the stability of the biceps tendon.
In the context described above, the purpose of the present study was to determine whether the morphology of the bicipital groove affects LHBT stability. Our hypothesis was that a shallow bicipital groove would contribute to tendon instability.
Materials and methods
Data were collected between January 2012 and December 2012 in the form of magnetic resonance images (MRIs) of the shoulder. The study considered patients who presented at the outpatient department of our institute with shoulder discomfort. The inclusion criteria were shoulder pain as the predominant complaint, age over 40 years, and MRI taken at our institute at the time of the visit and using a predefined protocol. The exclusion criteria were MRI from another institute or performed under a different sequential protocol; diagnosis of inflammatory arthritis; history of significant trauma or surgery; cysts in the region of the lesser tuberosity, inconspicuous groove with margins difficult to distinguish because of imaging errors or deformities; complete tendon tear; and equivocal position of the biceps tendon in the MRI. Institutional review board approval was waived for this retrospective analysis of MRIs, as no patient identification data were collected.
MRIs and measurements
The MRIs were obtained at our institute using a closed scanner with a standardized protocol for image sequencing and slice thickness to minimize imaging variability. Fat-suppressed T1-weighted fast spin-echo sequences were performed to acquire images in the axial plane (repetition time/echo time (TR/TE), 434–565/18–24 ms; section thickness, 3 mm; field of view, 15 cm; matrix size, 224 × 224), the coronal oblique plane parallel to the long axis of the supraspinatus tendon (TR/TE, 434–565/20–24 ms; section thickness, 3 mm; field of view, 15 cm; matrix size, 224 × 224), the sagittal oblique plane (TR/TE, 434–565/20–24 ms; section thickness, 3 mm; field of view, 15 cm; matrix size, 224 × 224), and a plane perpendicular to the long axis of the supraspinatus tendon (TR/TE, 434–561/18–24 ms; section thickness, 4 mm; field of view, 15 cm; matrix size, 224 × 224). T2-weighted turbo spin-echo sequences were performed to acquire images in the axial plane (TR/TE, 2868–3184/80 ms; section thickness, 3 mm; field of view, 15 cm; matrix size, 224 × 224; echo train length (ETL), 16), the coronal oblique plane (TR/TE, 2661–2906/80 ms; section thickness, 3 mm; field of view, 15 cm; matrix size, 256 × 256; ETL, 16), and the sagittal oblique plane (TR/TE, 2791–2906/80 ms; section thickness, 4 mm; field of view, 15 cm; matrix size, 264 × 262; ETL, 16). The images were analyzed using the Centricity web PACS viewer (GE Medical Systems, Chalfont, UK). The condition of the biceps tendon was determined by following the biceps tendon in all the sequential axial images. The position of the LHBT relative to the entire course of the intertubercular groove was assessed on transverse T1-weighted images.
Subluxation of the LHBT was defined as displacement of the LHBT over the inner rim of the intertubercular groove but with partial contact between the LHBT and the groove. 9 In the MRI, LHBT subluxation was clearly distinguishable from appropriate LHBT positioning within the bicipital groove (Figure 1) and diagnosed upon noting the biceps tendon perched on the lesser tuberosity of the humerus (Figure 2). 10 Dislocation of the LHBT was defined as a complete loss of contact between the LHBT and the intertubercular groove (Figure 3). 9 When the biceps tendon could not be visualized in or around the groove, the diagnosis of complete tear with retraction was established. After analysis, the shoulders with LHBT subluxation or dislocation were labeled as having unstable LHBT, while those with LHBT positioned within the groove were labeled as having stable LHBT.

MRI showing the LHBT positioned within the bicipital groove. MRI: magnetic resonance image; LHBT: long head of the biceps tendon.
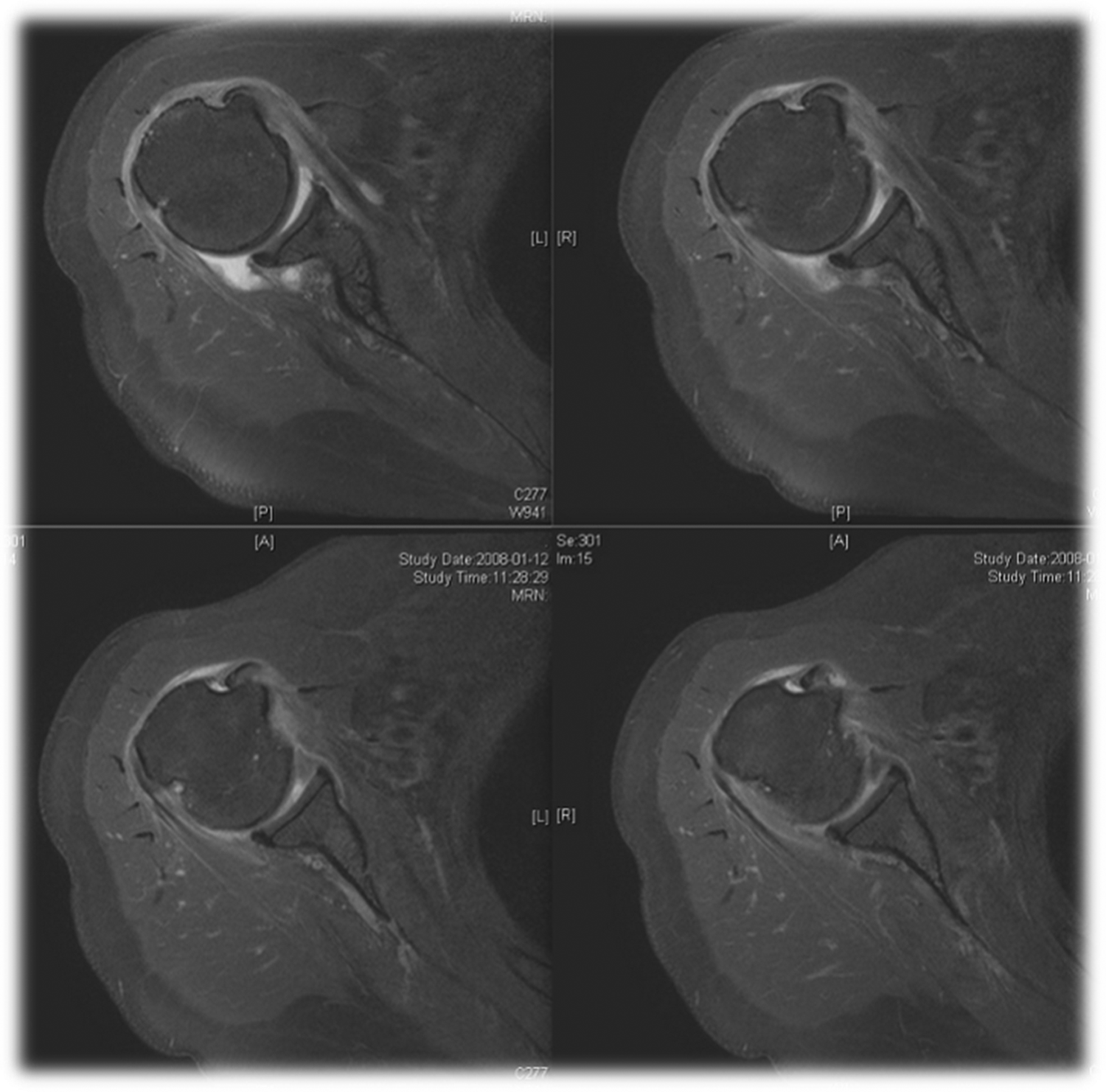
MRI showing subluxation of the LHBT, defined as a positioning of the tendon within the bicipital groove but perched on the lesser tuberosity. MRI: magnetic resonance image; LHBT: long head of the biceps tendon.
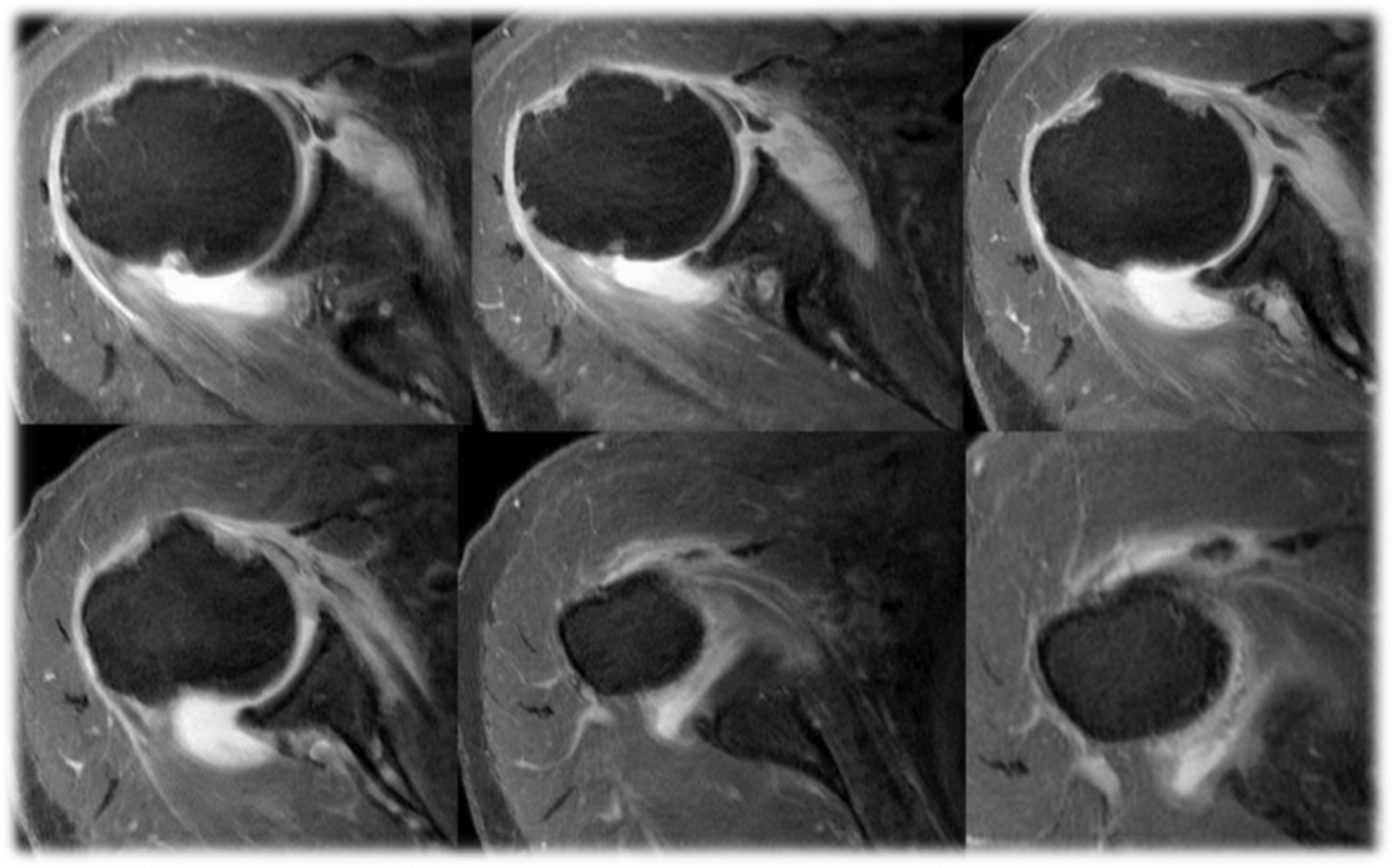
MRI showing dislocation of the LHBT, defined as a complete loss of contact between the tendon and the bicipital groove. MRI: magnetic resonance image; LHBT: long head of the biceps tendon.
The morphology of the bicipital groove was described in terms of distances and angles measured on the MRIs, as previously proposed. 4 The necessary lines and angles were drawn on the MRIs using the specialized functionality provided by the Centricity web PACS viewer. The values of the distances (in millimeter) and angles (in degrees) of interest were read from the screen. The opening angle, medial wall angle, and depth of the bicipital groove (Figure 4) were measured starting from the deepest point of the groove, which was previously described to lie at the midsection of the bicipital groove. The definition of shallow groove was based on the value of the opening angle (≥94°), as proposed and applied in earlier studies. 4 All measurements were performed by the same observer, who is a trained orthopedic shoulder fellow, with more than 1 year of experience evaluating shoulder MRIs. The measurements were performed twice on different dates, and the mean values were retained.
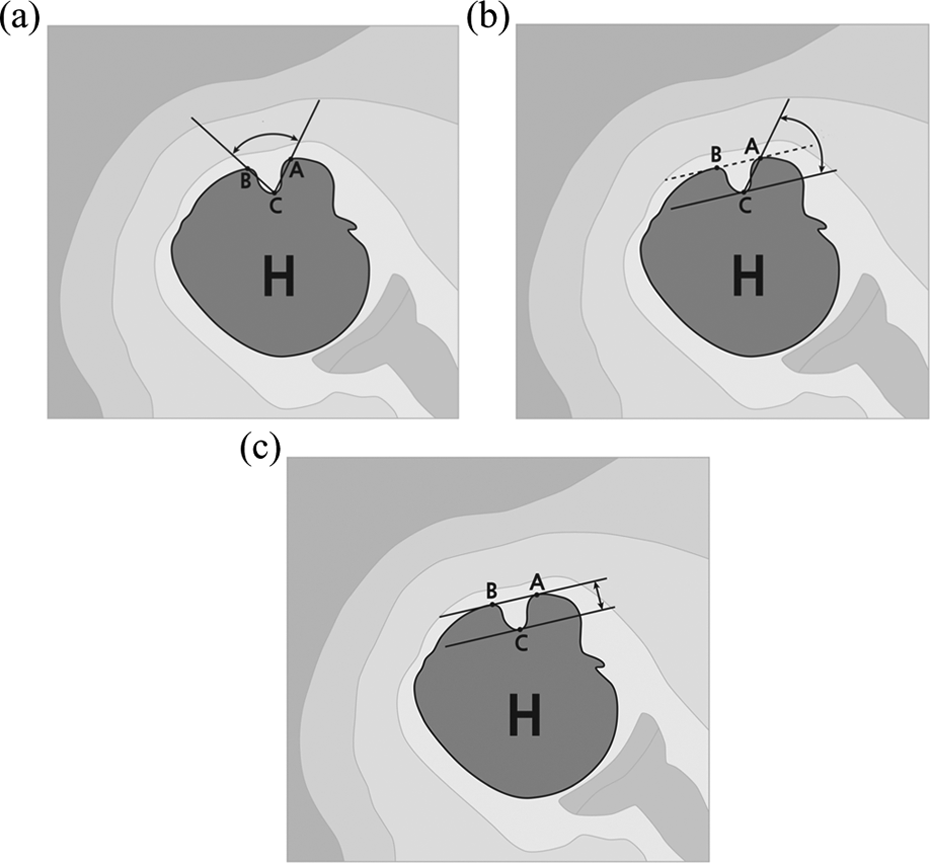
Measurement of the morphologic characteristics of the bicipital groove on a magnetic resonance image. (a) The opening angle represents the angle between the line connecting the deepest point of the groove and the highest point of the greater tuberosity (CB) and the line connecting the deepest point of the groove and the highest point of the lesser tuberosity (CA). (b) The medial wall angle represents the angle between the line connecting the deepest point of the groove to the highest point of the lesser tuberosity (CA) and the line passing through the deepest point of the groove (C) and parallel to the line connecting the highest points of the greater and lesser tuberosities (BA). (c) The depth of the bicipital groove represents the vertical distance from the deepest point of the groove (C) to the line connecting the highest points of the greater and lesser tuberosities (BA).
Analysis
A power calculation was performed according to the formula derived from the Gaussian distribution: n = (z·s/e)2, where n is the minimum sample size, z = 1.96 for the 5% level of significance, s is the standard deviation of the sample, and e is the accepted error. 11
We evaluated the differences between the groups of shoulders with stable and unstable LHBT in terms of bony morphology of the bicipital groove (depth, medial wall angle, and opening angle). We also compared shoulders with normal grooves against those with shallow grooves in terms of the incidence of tendon instability.
Results
In total, 464 patients (223 male) were included in the study. The average age of the subjects was 56.0 years (ranging from 40 to 86 years). The study sample consisted of 464 shoulders, diagnosed based on the MRIs with rotator pathologies (n = 341 shoulders; cuff tears in 234, tendinosis in 83, and calcifications in 24), adhesive capsulitis (n = 62), superior labrum anterior–posterior lesions (n = 26), or no specific pathology (n = 35). According to the power calculation, the sample size was sufficiently large to draw conclusions about the general population, accepting an error of 0.1 mm for the groove depth and 10° for the measured angles.
Statistically significant differences were identified between the groups of shoulders with stable and unstable LHBT with respect to age (p < 0.001), sex (p = 0.031), incidence of subscapularis tear (p < 0.001), groove depth (p = 0.008), medial angle (p = 0.014), and opening angle (p = 0.016). Compared to shoulders with stable LHBT, those with unstable LHBT showed a shallower mean depth (by 0.3 mm), a smaller mean medial angle (by 2.2°), and a larger mean opening angle (by 3.7°). The demographic data and morphological characteristics of the bicipital groove for the groups of shoulders with stable and unstable LHBT are presented in Table 1.
Demographic data and morphological parameters of the bicipital groove of shoulders with stable positioning (within the bicipital groove) and unstable positioning (subluxation or dislocation) of the long head of the biceps tendon.

LHBT: long head of the biceps tendon.
On the other hand, we found that 433 shoulders had normal groove, while 31 had shallow groove (opening angle ≥94°). The bicipital groove was determined to be normal in 354 (94.9%) of 373 shoulders labeled as stable LHBT and in 79 (86.8%) of 91 shoulders labeled as unstable LHBT, and this difference was statistically significant (p = 0.011).
Discussion
We found that shallow morphology of the bicipital groove, identified by the shallower depth, larger opening angle, and smaller medial angle as measured in the MRI, may represent a predisposing factor for developing biceps tendon instability. Therefore, the morphology of the bicipital groove should be considered as a potential factor affecting the stability of the biceps tendon.
The biceps tendon has been identified as a common source of shoulder pain and related disability, but the exact incidence of LHBT instability remains unknown. 1 A study based on computed tomography arthrography reported that medial displacement of the LHBT may occur in up to 16% of rotator cuff tears. 9 A more recent arthroscopic study identified LHBT instability in 45% of patients with a rotator cuff tear, with isolated anterior instability in 16%, isolated posterior instability in 19%, and combined anteroposterior instability in 10% of tears. 2 Isolated lesions of the biceps tendon, not accompanied by rotator cuff pathologies, have also been reported. 6,12 A recent study by Urita et al. showed that the presence of a spur on the bicipital groove or a subscapularis tear was useful for identifying LHBT disorders. 13 The LHBT can be affected by a wide range of pathologies such as tendinitis, partial or complete tear, and instability in the form of subluxation or dislocation. Of these pathologies, the present study focused on LHBT instability. Soft tissue restraints and the bony contours of the bicipital groove are known to confer stability to the LHBT during its excursion. 1 The bicipital groove is an hourglass-shaped corridor between the greater and lesser tuberosities of the humeral head. The soft tissue restraints, including the superior glenohumeral ligament and the coracohumeral ligament, form the biceps pulley, along with the tendons of the subscapularis and supraspinatus. 1 Biceps tendon instability has also been noted in patients with intact rotator cuffs and has been postulated to be due to injury to other restraints. 14
The bony contours of the bicipital groove might restrain the biceps tendon in the groove, although they are thought to play a lesser role than that of the soft tissue restraints. 9 Research into the relationship between the characteristics of the bony morphology of the bicipital groove and the incidence of tendon instability has been ongoing for several decades. Meyer identified a supratubercular ridge in 17.5% of 200 humeri evaluated and suggested that the presence of this ridge increases the probability of dislocation of the biceps tendon from the bicipital groove. 6 Hitchcock and Bechtol studied 100 humeri and suggested an association between the presence of a supratubercular ridge and the presence of spurs in the bicipital groove. 5 They further distinguished a moderately or markedly developed supratubercular ridge in 59% and 8% of the evaluated humeri, respectively. Hitchcock and Bechtol also suggested the importance of the angle formed by the line joining the greater and lesser tuberosities with the medial wall of the bicipital groove (formed by the lesser tuberosity). They noted that the anatomy of the human shoulder dictates that the biceps tendon is pulled against the lesser tuberosity when it is under tension and suggested that the angle of the medial wall is therefore very important in retaining the tendon within the bicipital groove, with a steeply sloped medial wall offering better retention. Pfahler et al. studied the morphology of the bicipital groove on radiographs tangential to the bicipital groove and correlated the radiographic findings with the pathology of the biceps tendon, as determined by ultrasonography and clinical symptoms. 7 Even in the absence of an MRI-based assessment of tendon instability, a positive correlation was found between LHBT tendinitis (both clinically and on ultrasonography) and acute opening angles, flat groove, and small medial opening angles. Slatis and Aalto also noted that an inadequately developed, shallow medial wall of the bicipital groove is associated with LHBT dislocation. 15 Abboud et al. recently evaluated the biceps tendon and intertubercular groove morphology on T1 axial MRIs in 75 patients and found no correlation between biceps groove morphology and intraoperative arthroscopic findings indicating LHBT pathology. 4 The pathology of the biceps has been reported to have a bimodal distribution with regard to the bicipital groove morphology. Specifically, a shallow groove may predispose to biceps tendon instability and lesions caused by impingement against the transverse ligament, whereas a deep groove may predispose to lesions caused by impingement against the wall of the bicipital groove. 11 Therefore, studies that aim to detect an association between the morphology of the bicipital grove and LHBT lesions suffer from inherent bias, as instability and impingement are not studied separately.
Spritzer et al. analyzed the relationship between the bicipital groove morphology and biceps tendon instability. 10 They reported a strong correlation between the shape of the intertubercular sulcus and the presence of LHBT instability. However, the findings of that study were not quantitated and were limited by the small sample size and lack of statistical analysis. Studies based on the shape of the bony profile also suffer from the lack of a standardized definition of deep and shallow grooves, rendering such investigations impractical at this time. To the best of our knowledge, no systematic study has been performed to examine the correlation between biceps tendon instability and the morphology of the bicipital groove. The results of such a study will shed light on the influence of groove morphology on the incidence of tendon instability. The present study is a step in this direction, as we analyzed the morphology of the bicipital groove with specific reference to the incidence of biceps tendon instability. Another unique feature of our study is that we included all symptomatic patients over the age of 40 years, not only those requiring surgery. Since both shallow and deep bicipital grooves can cause pathologic changes, we studied only the tendon instability, thereby avoiding the confounding effect of impingement. The results of our study indicated that a shallow bicipital groove causes predisposition to biceps tendon instability. A shallow biceps groove can be identified in an MRI based on the small medial angle or large opening angle, along with reduced depth of the bicipital groove. This straightforward evaluation will allow the surgeon to make an informed decision while choosing surgical options for the management of LHBT lesions.
Our study has several limitations. First, all measurements were made on MRIs, and therefore we could only assess static instability. Not including data on dynamic instability may represent a limiting factor. Another limitation of the use of MRIs is that bony anatomy is less evident than in images generated from computed tomography experiments. However, magnetic resonance evaluations are widely performed on the target population, and therefore MRIs are readily available. Obtaining computed tomography data would entail exposure to radiation, which can be avoided by the use of the readily available MRIs. Third, since this was a retrospective study, it was not possible to assess the rotation of the arm during MRI acquisition, which may affect the findings related to LHBT stability. Although Buck et al. reported that rotation of the humerus does not critically affect the position of the LHBT in relation to the bicipital groove, 16 no consensus exists on the matter; therefore, it would be better to standardize arm rotation when performing the assessment. Fourth, the 464 patients included in this study had shoulder pain, suggesting the potential coexistence of various conditions. Finally, all measurements were performed by the same observer. Although the observer is a trained shoulder orthopedic fellow with ample experience, it is not possible to assess the bias associated with these observations. Nevertheless, the measurements were performed twice on different dates to reduce the bias. The fact that the same surgeon performed all of the measurements ensured that the evaluation was consistent.
Conclusion
A shallow bicipital groove, identified by the shallower depth, larger opening angle, and smaller medial angle, may represent a risk factor for the development of biceps tendon instability. This aspect should be considered when making treatment decisions for the management of biceps tendon lesions during arthroscopic surgery of the shoulder.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.