
Abstract
Background:
Proximal humeral fractures are common in the elderly and can present with multiple fracture configurations. Our case series describes a three-part valgus-impacted fracture pattern of the proximal humerus that underwent spontaneous reduction by nonsurgical management with good functional outcomes.
Methods:
Seven patients who sustained low-energy three-part valgus-impacted fractures of the proximal humerus were studied. We retrospectively reviewed serial anteroposterior radiographs of each patient taken as part of routine follow-up. For clinical outcomes, patients were assessed by a physical examination of both shoulders. A Disability of Arm, Shoulder, and Hand (DASH) questionnaire assessed the functional outcomes.
Results:
In all seven patients, fractures reduced spontaneously without any complications. Radiologically, the neck–shaft angle decreased from an average of 169° to 141
Conclusion:
Low-energy three-part valgus-impacted fracture pattern of the proximal humerus has the ability to spontaneously reduce by nonsurgical management with good functional outcomes.
Keywords
Introduction
Fractures of the proximal humerus are the third most common fractures in the elderly, 1 usually occurring after falls from standing height. 2
Court-Brown et al.’s 3 landmark study in 2002 first reported positive functional outcomes in patients with displaced valgus-impacted fractures of the proximal humerus treated nonsurgically. Recently, there has been further emphasis on the outcomes of nonsurgical management 4,5,6 of proximal humerus fractures, with trials such as the Proximal Fracture of the Humerus: Evaluation by Randomisation (PROFHER) 6 randomized clinical trial reporting no significant differences in functional outcomes in patients with displaced fractures treated surgically versus nonsurgically.
Our study aims to highlight the ability of a displaced three-part valgus-impacted fracture pattern to spontaneously reduce with nonsurgical management despite an anatomical and mechanical disadvantage while showing good functional outcomes.
Materials and methods
All the recruited patients were those who presented over a span of 3 years between 2012 and 2014. All seven patients initially presented to the accident and emergency department and were subsequently seen in the specialist orthopedic clinic within 5 days of presentation.
Patients were included only if they adhered to the following inclusion criteria. All included must have sustained the aforementioned three-part valgus-impacted fracture pattern of the proximal humerus secondary to low-energy trauma. All must have had the same treatment protocol, which included only nonsurgical management with analgesia as well as immobilization in an arm sling followed by physiotherapy. While in the arm sling, no specific position of immobilization was utilized for these patients. Physiotherapy was started after approximately 4 weeks of immobilization in the arm sling for each patient and included flexibility exercises such as pendular exercises, joint and soft tissue mobilization, and strengthening exercises of the shoulder. All patients were followed up regularly in our physiotherapy center and were also taught how to do their own therapy independently at home.
We evaluated each patient radiographically and clinically. Radiographically, X-rays of the shoulder at time of injury as well as at subsequent follow-ups were taken. The neck–shaft angle for each radiograph was measured twice on two separate occasions and averaged to increase accuracy. The neck–shaft angle was determined by the intersection of a line drawn on the central axis of the humeral shaft and another line drawn perpendicular to the anatomical neck of the humerus.
Clinically, a routine shoulder examination was done to assess any residual bony deformity as well as the power and range of motion of the bilateral shoulders. Each patient was also requested to complete the Disability of Arm, Shoulder, and Hand (DASH) questionnaire. DASH consists of a 30-item self-reported questionnaire designed by the American Academy of Orthopaedic Surgeons (AAOS) used to measure physical function and symptoms in people with musculoskeletal disorders of the upper limb.
Results
All seven patients included in our study with three-part valgus-impacted fracture patterns of the proximal humerus sustained closed fractures secondary to low-energy trauma. The interval between the latest clinical assessment and the date of the injury varied between 3 and 19 months for each patient. One patient declined to complete the DASH questionnaire and two refused a physical examination.
Of the seven patients in our study, three were male and four were female. The mean age of the study population was 62 years, ranging from 39 to 79 years. All seven patients except one patient who had a history of mixed dementia were premorbidly independent in their activities of daily living and active in the community.
Significantly, all seven fractures in our study underwent spontaneous reduction at the time of latest follow-up. The medial cortices of each fracture, which were originally displaced, all managed to spontaneously reduce and unite in all seven fractures. We also noted a significant decrease in the humeral neck–shaft angle. An average of 105 days ranging from 26 days to 330 days elapsed between the day of injury and the final radiograph taken as part of the follow-up. In our series, the humeral neck–shaft angle decreased from an average of 169° prereduction (156–179°) to 141° (128–150°). Overall, this represented an average decrease of 28° (Figures 1–3).

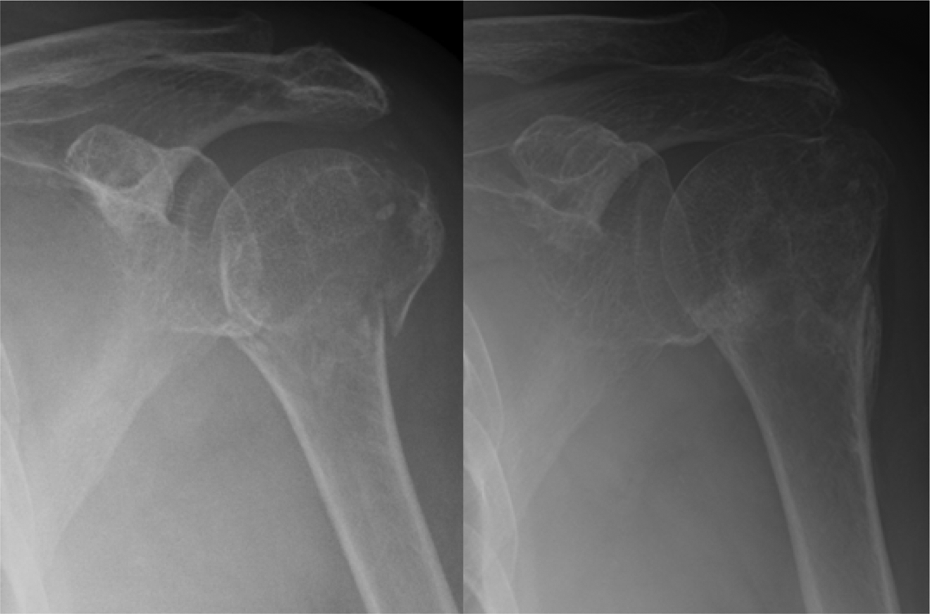
Radiographs belonging to a 69-year-old gentleman taken on the day of the injury and 28 days after the injury. The neck–shaft angle decreased from 165° to 128°. At the point of last review, he reported no limitation in his daily activities.
Radiographs of a 73-year-old lady on the day of the injury and 93 days post injury. The neck–shaft angle decreased from 156° to 143°. At the latest review, she had returned to doing all her regular activities including marketing and housework.

Radiographs of a 79-year-old lady. The neck–shaft angle decreased from 174° to 150°, 330 days after the injury. She had almost no limitation in motion relative to the contralateral shoulder and had no limitations in her daily activities at the time of the latest review.
On physical examination, none of the patients exhibited any gross deformity of the affected arm on inspection or palpation. No pain was reported on palpation or active and passive movement of the affected arm. Average ranges of motion for flexion, abduction, and external rotation were measured and compared to the contralateral side. In the affected arm, the range of motion obtained included an average flexion of 134° (110–160°), external rotation of 36° (20–45°), and abduction of 122° (100–140°). This is compared to the nonaffected contralateral arm, which exhibited an average flexion of 163° (140–180°), external rotation of 55° (45–75°), and abduction of 163° (130–180°). Power was grade 4 of 5 for abduction, flexion, internal rotation, and external rotation relative to the contralateral side for three patients, and 5 of 5 for all three motions in two patients.
For six patients interviewed, the mean DASH score was 18.17 points, which was at an average of 13.6 months after the initial injury.
At the time of the latest follow-up, all seven patients managed to obtain their premorbid functional levels. None of our patients experienced any significant complications such as avascular necrosis of the humeral head, rotator cuff injury, adhesive capsulitis, or persistent pain.
Discussion
Achieving anatomical reduction is one of the key challenges in the treatment of proximal humerus fractures especially in displaced, comminuted fracture patterns.
A study by Tepass et al. in 2013 7 surveying the experiences of a total of 348 hospitals in the treatment of proximal humeral fractures revealed nonanatomic reduction as the top and secondary displacement of the fracture as the third most common complications among implant perforation, avascular necrosis, and implant-related impingement in the top five most commonly seen complications.
In the three-part valgus-impacted fracture pattern, self-reduction is unique and unexpected as it occurs against a mechanical disadvantage. In this fracture configuration, the greater tuberosity is abducted by the pull of the supraspinatus, and both gravity and the pull of the deltoid muscle act in opposite directions on the humeral head and shaft respectively to impact the humeral head into the shaft of the humerus. Despite this, all three fracture fragments were able to spontaneously disimpact and reunite against the pull of the attached musculature and force of gravity without any active reduction in all seven patients in our series. Of note, the humeral head was also noted to drift superiorly out of valgus as reduction occurred. We are unable to definitively explain how this unique observation occurs but postulate that transient deltoid weakness could be a factor in facilitating self-reduction. Due to the retrospective nature of our study, a clear time course for reduction was not possible as follow-ups and intervals between radiographs were not uniform.
Although not the primary aim of our study, we also assessed the clinical outcomes in our patients against patients treated both nonsurgically and surgically. Court-Brown et al.’s 3 study found that patients with displaced three-part fractures of the proximal humerus treated nonsurgically saw a perceived 10% drop in strength and reach as well as approximately 20% drop in abduction and flexion on the affected side. In our series, the two youngest patients aged 39 and 41 years managed to achieve Medical Research Council (MRC) grade 5 power, whereas all the remaining patients above the age of 60 years obtained MRC grade 4 power globally. Both patients obtaining MRC grade 5 power reported a subjective weakness in the affected arm despite having no demonstrable weakness in the contralateral arm. Range of motion was limited by approximately 18% in flexion and 25% in abduction, but none of our patients reported any significant limitation in activity.
In 2002, a large-scale study done by AAOS consisting of approximately 450,000 households estimated the mean DASH score of the population to be 10.1. 8 Of the six patients we reviewed in our series, the mean DASH score was 18.17, which is just above the population mean as reported by AAOS.
Limitations of study
Some limitations of our study include a relatively small sample size and its retrospective nature. Further studies are needed to evaluate the topic further such as a study of a control group. Further imaging such as computed tomography scans could also aid in better visualizing the fracture pattern and the process of reduction.
Conclusion
Our case series serves to emphasize a displaced three-part valgus-impacted fracture pattern of the proximal humerus that unexpectedly underwent spontaneous reduction by nonsurgical management.
Footnotes
Author’s note
National Healthcare Group Institution DSRB, Study number 2014/00234.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.