
Abstract
Aims:
Magnetic resonance guided focused ultrasound (MRgFUS) is a new modality in the management of primary and secondary bone tumors. We aimed to investigate the safety, efficacy, and feasibility of using MRgFUS for the treatment of (1) benign bone tumors with the intent of complete tumor ablation, (2) primary malignant bone tumors with the intent to assess its effectiveness in causing tumor necrosis, and (3) metastatic bone disease with the intent of pain relief.
Method:
Twenty-four patients with benign bone tumors, primary malignant bone tumors, and metastatic bone disease were treated with one session of MRgFUS. Contrast-enhanced (CE) magnetic resonance imaging (MRI) was carried out post-procedure to assess and quantify the area of ablation. Those with malignant primary tumors had the tumors resected 2 weeks after the treatment and the ablated areas were examined histopathologically (HPE). The other patients were followed up for 3 months to assess for the side effects and pain scores.
Results:
Significant volume of ablation was noted on CE MRI after the treatment. Benign bone tumors were ablated with minimal adverse effects. Metastatic bone disease was successfully treated with significant decrease in pain scores. Ablated primary malignant tumors showed significant coagulative necrosis on MRI and the HPE showed 100% necrosis. Pain scores significantly decreased 3 months after the procedure. Only two patients had superficial skin blistering and three patients had increase in pain scores immediately after treatment.
Conclusion:
MRgFUS is effective, safe, and noninvasive procedure that can be an adjunct in the management of primary and metastatic bone tumors.
Introduction
Amputation used to be the standard method of treatment for bone sarcomas until 1980s. The development of limb-sparing surgery for malignant bone tumors has changed the face of cancer treatment. New advances in imaging and chemotherapy have contributed to better survival rates. 1 Survival rates improved from 15% to 20% before the 1970s with surgery alone to 55–80% in the 1980s with the addition of chemotherapy. Multiple-drug regimens are now considered essential part of bone sarcoma treatment. 1
Latest addition to the current treatment for bone tumor is ultrasound. Two most commonly employed ultrasound treatments are high-intensity focused ultrasound (HIFU) and magnetic resonance guided focused ultrasound (MRgFUS).
HIFU is a precise procedure by which pathogenic tissue is heated, ablated, and destroyed. In medical research, HIFU has been a subject of researchers for over 20 years now. HIFU causes selective tissue necrosis in a well-defined volume, at a variable distance from the transducer, by heating. For therapeutic purpose, ultrasound therapy uses lower frequencies with significantly higher intensities. Focused ultrasound generates heat, ablating tissue only at the focal point. The ablation of each focal volume of a tissue is called a sonication. In HIFU therapy, ultrasound beams are focused on diseased tissue, due to the significant energy deposition at the focus, temperature within the tissue can rise as high as 65°C and above, this destroys diseased tissue by coagulation necrosis. Higher temperature levels are avoided to prevent boiling of liquids inside the tissue. In theory, sonication of the beam treats a defined portion of the targeted tissue. Treatments consist of multiple exposures of focused energy or sonication. Extracorporeal HIFU ablation in the treatment of patients with large hepatocellular carcinoma. 2 –4
MRgFUS[Since both “magnetic resonance imaging guided focused ultrasound” and “magnetic resonance guided focused ultrasound” are given as expansions for “MRgFUS,” we have followed “magnetic resonance guided focused ultrasound” as the expansion throughout article for consistency. Please check and approve.] is a noninvasive method for ablating tumors, which combines two different technologies: magnetic resonance (MR) imaging (MRI) is used for guidance and monitoring purposes and HIFU. It is an attractive modality for the noninvasive thermal ablation of soft tissue tumor. 5 –9 MR thermometry allows the physician to control and adjust the treatment in real time to ensure that the targeted tumor is fully treated and the surrounding tissue is spared. MR images that are acquired during the process will confirm the area of the sonication and also will give the quantitative analysis of the area of coagulative necrosis. It offers efficient and safe focused ultrasonic waves treatment.
MRgFUS is currently used for treatment of uterine fibroids, 10 breast cancer, 11 prostate cancer, 12 liver, 13 and renal tumors. 14 Each treatment performed using different protocols and principles.
In our study, we used MRgFUS to determine the effectiveness of treatment in primary bone tumors (malignant and benign) and metastatic bone disease. For this study, we created a standardized protocol to deliver safe and efficient treatment.
The aim of this study is to investigate the safety, efficacy, and feasibility of using MRgFUS for the treatment of: benign bone tumors with the intent of cure, primary malignant bone tumors with the intent to assess its effectiveness in causing tumor necrosis, and metastatic bone disease with the intent to control pain.
Materials and methods
This interventional clinical study was carried out at the University of Malaya Medical Centre, Kuala Lumpur. It is a non-randomized uncontrolled single-group treatment clinical study carried out from September 1, 2009 till April 30, 2012. This study was approved by the Hospital Ethical Committee (MEC: 738.3) prior to the interventional clinical study. Strict inclusion and exclusion criteria were followed as listed below: Inclusion criteria Both male/female patients more than 11 years old. Patients who have consented and able to attend all study visits. Patients with histologically confirmed primary malignant bone tumor. Patients with known tumors who present with painful metastasis. Patients with symptomatic radiological confirmed benign bone tumors. Patients with primary malignant bone tumor planned for wide resection. Targeted tumors are MRgFUS device accessible, for example tibia, fibula, or femur. Tumor not involving the neurovascular bundles. Patients whose lesion are ≥5 mm away from the skin. Tumors clearly visible by non-contrast MRI. Exclusion criteria Diffuse skeletal tumor spread as evaluated by imaging. Patients who need surgical stabilization of the affected bone in metastatic bone disease. Impending fracture of the metastatic bone. Targeted tumor located in the vertebral column.
Patients with unstable cardiac status including unstable angina pectoris on medication documented myocardial infarction within 6 months of protocol entry, congestive heart failure requiring medication (other than diuretic), and patients on anti-arrhythmic drugs. Severe uncontrolled hypertension (diastolic BP > 100 on medication). Patients with standard contraindications for MRI such as non-MRI compatible implanted metallic devices including cardiac pacemakers and so on. Known intolerance or allergies to the MRI contrast agent (e.g. gadolinium or Magnevist). The presence of scarring in the path of the passage of the energy-planned to the treatment area such as keloid, previous scars or traumatic scars. Tumor involving the neurovascular bundles or <1 cm from tumor margin. Severe cerebrovascular disease (multiple Cerebrovascular accident (CVA) or CVA within 6 months). Patients on anticoagulation therapy or those with an underlying bleeding disorder. Individuals who are not able or willing to tolerate the required prolonged stationary position during treatment (approximately 3 h). Patients whose lesion are <5 mm from the skin. Patients with previous radiation therapy. Patients with life expectancy <3 months (inadequate time for the follow-up of the patient to check the safety parameters of this study). Patients with surgical stabilization of tumor site with metallic hardware.
We recruited the patients from the orthopedic oncology clinic. Informed consent was taken from the patient or family members. They were given information regarding the research study, MRgFUS procedure, risks, and benefits of the treatment. Written informed consent was obtained.
Preoperative MRI and CT scans were performed to determine the extent of tumor, marrow involvement, and location of vital structures. All patients were treated with one session of MRgFUS using the “Bone 2 apparatus” with enhanced/elongated/nominal sonication. Analgesia and sedation administered during the procedure and complications encountered were recorded. For cases of primary malignant bone tumors such as osteosarcoma, only a portion of the tumor was ablated to determine its effectiveness in order to determine percentage of necrosis post chemotherapy of the specimen. The area ablated was noted to the pathologist reading the specimen.
Area of ablation was monitored during the MRgFUS procedure and the number of “sonication” was decided according to the needs and condition of the patients. Analysis was done pre and during the procedure so that the desired area of ablation and necrosis can be estimated and achieved in one cycle of MRgFUS.
Dynamic contrast-enhanced (CE) MRI was performed immediately after the treatment and the extent of non-perfusion was used to assess the completeness of treatment, the extent of the tumor necrosis. This was measured as the cubic centimeter area of necrosis.
Area of necrosis and ablation was measured immediately after the MRgFUS procedure using CE MRI scan. The hypointense areas on the MRI scan showing area of necrosis were compared with the pre-procedure scans and actual area of ablation by MRgFUS. Area of ablation was calculated and recorded in cubic centimeter.
The temperature at the area of ablation was recorded during the MRgFUS procedure and compared with the pre-procedure MRI and CT scans. It was noted that the areas that show increased temperature were corresponding with the hypointense areas on post-procedure MRI scan, thus necrosis and ablation by MRgFUS was confirmed in these particular parts of the tumor. After the area of ablation was calculated on each slice of MRI scan, multiplication with the number of slices for that particular region was done, thus giving us the actual area of ablation in cubic centimeter.
Volume of the ablated tissue was measured in cubic centimeter area, so that the actual ablation power of the focused ultrasound can be measured under the MR guidance.
Histopathological examination
For the cases of primary bone tumor, surgical excision was performed within 2 weeks after the MRgFUS therapy. The resected specimen was sectioned to determine evidence of gross tumor destruction and any re-growth of tissue in the treated region. This is compared to the post-MRgFUS CE MRI to determine the percentage of tumor viability in treated areas and graded as follows: 0%, <10%, 10–25%, >25%, >50%.
Post-procedure patient assessment
Patients were assessed on day 1 for the complications such as skin burns, pain, fractures, and neurovascular injury. A second assessment was carried out 3 months after the procedure.
Data collection
Visual analogue score (VAS) pain scores were assessed and recorded for all the patients. First recording was done before procedure when patients were recruited in the study. Second recording was done 1 day after the procedure. Third was done 3 months after treatment. The use of analgesic drugs before and after the procedure was also recorded.
For the safety analysis, the side effects such as blisters and superficial skin burns, fractures associated with the treatment, neurovascular damage, and other local and systemic side effects were assessed after the treatment. The assessment was done before MRgFUS, on day 1 and 3 months after the procedure.
The assessment for the tumor necrosis or area of ablation after the treatment was done using the CE MRI. The hypointense areas showing the ablated regions were compared with the pre-procedure MRI scans, and then calculations were made accordingly. These measurements were recorded as area in cubic centimeter units.
Data analysis
Data analysis was performed by a statistician using the SPSS version 20.
Results
Total number of recruited patients for the study during the study period was 26. Only 24 patients managed to complete the procedure. Two patients were excluded from the study as their body size could not fit into the MRgFUS system table.
The age of patients ranged from 12 years to 60 years old (mean age: 28 years old) as shown in Figure 1. Majority of the patients were male (male:female ratio; 3:1). Majority of the tumors (71%) were located on the lower limb: seven each in femur and tibia; three each in pubic rami, fibula, and humerus; and one in radius. Most of the patients were cases of osteosarcoma (45%), followed by osteoid osteoma (18%) and others such as Ewing’s sarcoma (9%), metastatic bone disease (14%), chondrosarcoma (9%), and Synovial Sarcoma (5%).
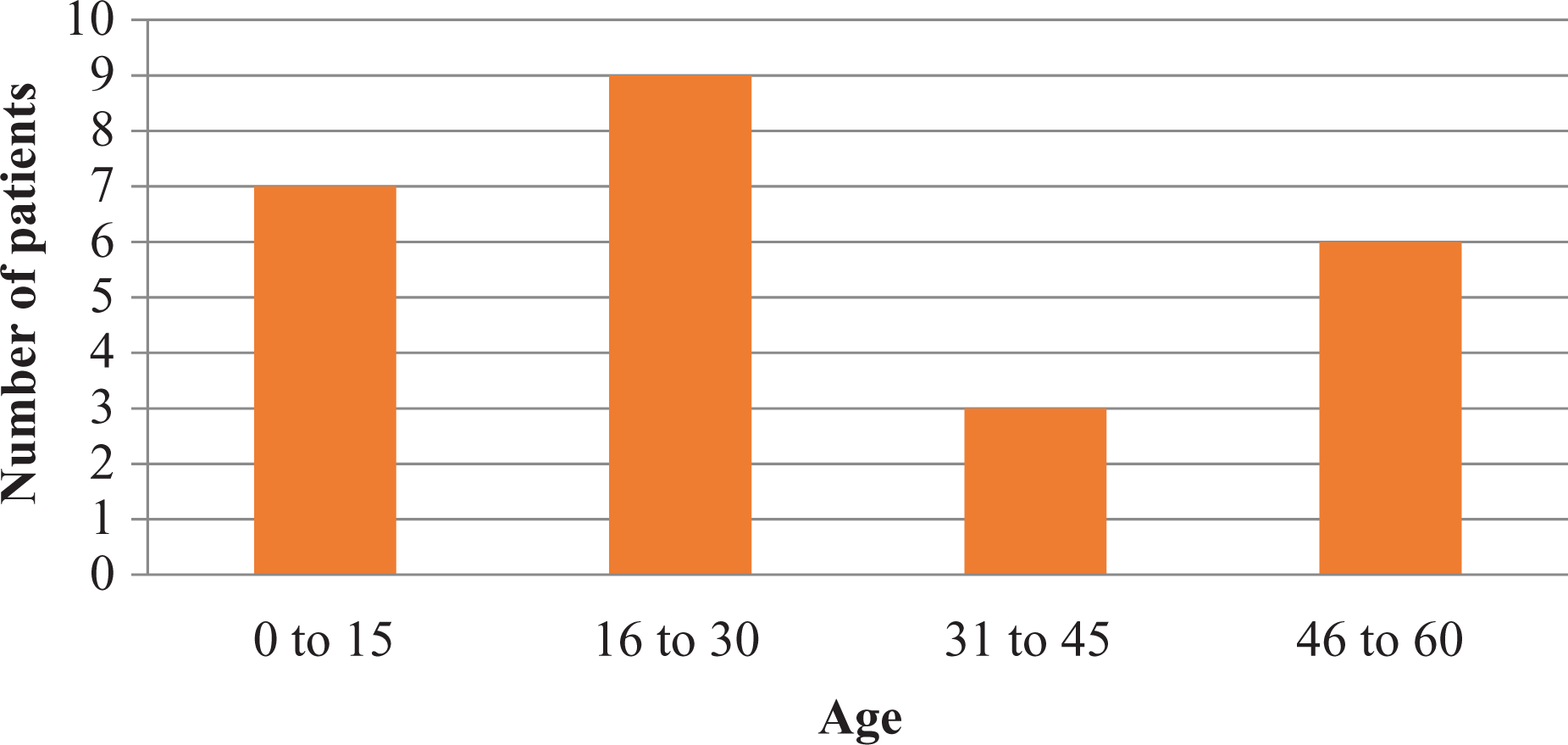
Age distribution.
Area of ablation and number of sonication
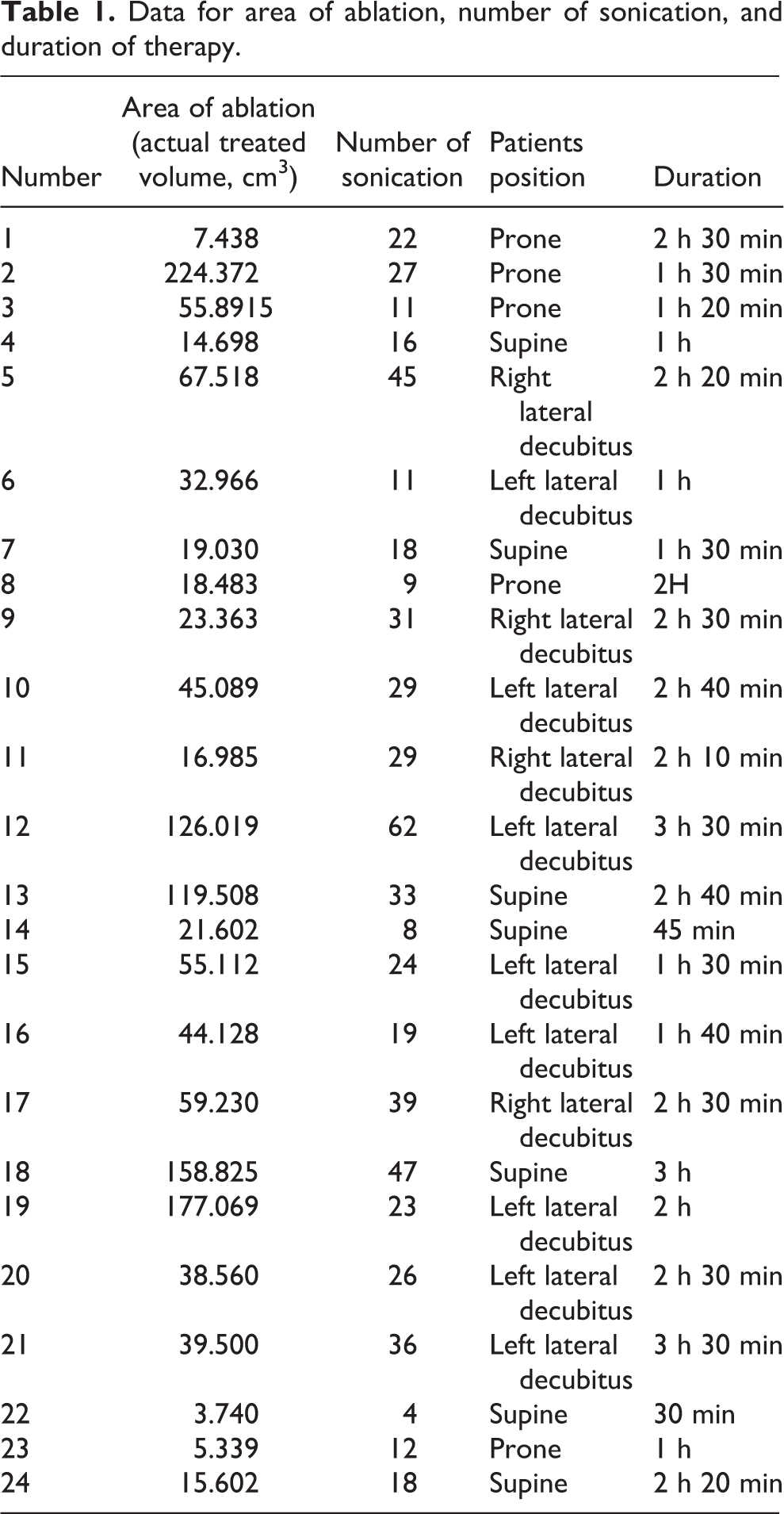
Position of the patient on the treatment table was dictated by the location of the tumor, depth from the skin, size of tumor, and area plan for ablation by MRgFUS. Twelve patients were in decubitus position, seven in supine positions, and five in prone position.
The longest duration for treatment was 3 h and 30 min, and shortest duration for the treatment was 30 min. The average time for treatment was 1 h 50 min (Table 1). The duration for treatment was determined by the number of sonication required per patient, that is, higher number of sonication will require more time for ablation.
Data for area of ablation, number of sonication, and duration of therapy.
From our study, the lowest value for area of ablation was 3.740 cm3 and highest value was 224.372 cm3 (mean = 57.89 cm3). The highest numbers of sonication given to patient were 62 and the lowest numbers of sonication given were 4 (mean = 25). The patient who had 62 sonication had actual area of ablation of 126.01 cm3, while the patient getting four sonication had an actual area of ablation of 3.74 cm3 (Table 2). Larger area of ablation naturally required a higher number of sonication.
MRgFUS ablation values.
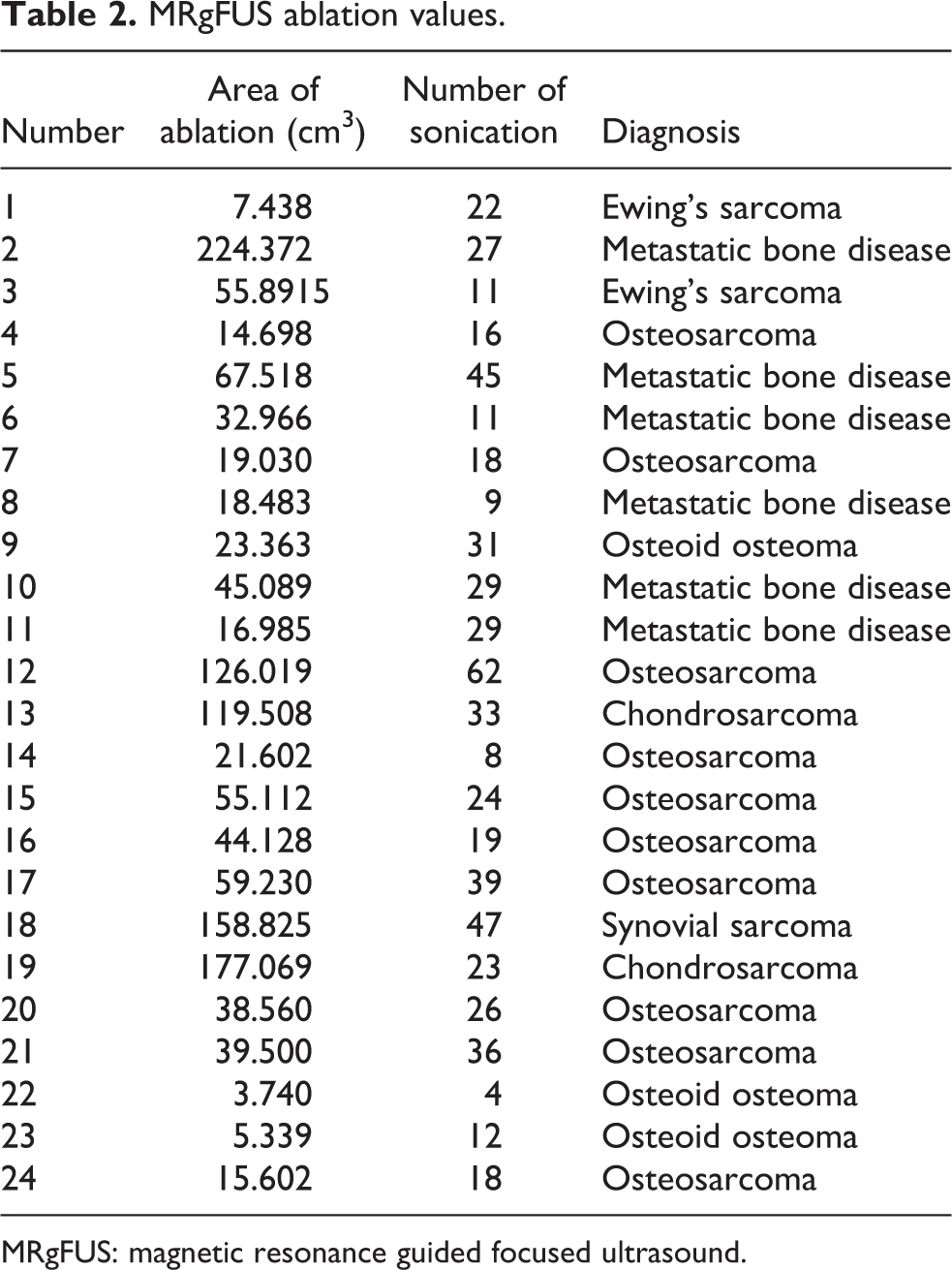
MRgFUS: magnetic resonance guided focused ultrasound.
Volume of ablation measured in cubic centimeters was analyzed to calculate the efficacy of MRgFUS procedure. This was done via the Functool software (version 10.2) as shown in Figure 2.

Area of ablation.
Pain score and side effects associated with MRgFUS treatment
The VAS scores are shown in Table 3. The mean VAS pain score pre-procedure was 3.04, on post-procedure day 1 was 3.17, and post-procedure 3 months was 0.7 (n = 10, patients who did not undergo resection). There was no significant difference before and after the MRgFUS treatment after one day of therapy (p-value = 0.327). However, the VAS score was significantly lower after 3 months of procedure (p-value = 0.000).
VAS score assessment before and after treatment.

Side effects
Only two patients (7.7%) were noted to have superficial burns such as blisters at the site of treatment, and three patients (11.5%) had significant pain immediately post-procedure with pain score (VAS) more than 6.
Histopathological examination
Histopathological analysis of the tumors was only done for the primary malignant bone tumors (n = 14) because these tumors were removed after the MRgFUS procedure. Benign tumors and metastatic bone diseases were not included, as no surgical indications for total resection of these tumors.
Although the histopathological examination (HPE) analysis showed 100% necrosis, in area of tumor tissue ablated by MRgFUS. The HPE results were difficult to interpret in measuring the effectiveness of MRgFUS procedure because it was difficult to differentiate on HPE, whether the necrosis was caused by chemotherapy in these cases or by the MRgFUS ablation as most of these patients were on neoadjuvant chemotherapy.
Treatment outcome
Four patients in this study had benign lesions such as osteoid osteoma. The patients with benign lesions showed significant ablation volume on the post-procedure MRI, as showed in the actual ablation values data. They also remained symptom free in the period of follow-up for this study (3 months). The VAS scores showed significant decreased values on follow-up at 3 months.
Patients with primary malignant tumors (i.e. 10 patients with osteosarcoma, 2 patients with chondrosarcoma, 2 patients with Ewing’s sarcoma, and 1 with synovial sarcoma) were assessed by post-procedure MRI, which showed significant area of necrosis as showed in the actual ablation values data, and also the HPE analysis of these tumors showed 100% necrosis of tumor tissue in the areas ablated by MRgFUS.
Patients treated for the metastatic bone disease (n = 6) were also assessed by post-procedure MRI, which showed significant area of ablation as showed in the actual ablation values data. Follow-up on these patients was done for 3 months and they stayed symptom free with significant decrease in pain scores.
Discussion
For the past 20 years, HIFU in combination with diagnostic ultrasound and more recently MRI (MRgFUS) have opened new avenues of therapeutic treatment for bone and soft tissue sarcoma. The therapeutic potential of HIFU has enabled a more focused and localized application of high-energy therapy without harming the surrounding tissue.
The addition of MRI guidance with HIFU allows for better pretreatment planning, control, and direct monitoring of the treatment process during the process of ablation of the targeted pathology. 15 HIFU is used for the thermal treatment of benign and malignant lesions, targeted drug delivery, and also for the treatment of thrombi (sonothrombolysis). Therapy of prostate cancer under ultrasound guidance and the ablation of benign uterine fibroids under MRI monitoring are now available to patients. 15 This treatment is US Food and Drug Administration (FDA) approved. The HIFU ablation therapy of prostate cancer under ultrasound guidance is clinically available in Europe, Asia, and the Americas except for the United States. For other target organs (breast, brain, liver, and bone), HIFU is still in clinical or preclinical test phase.
MRI has significant beneficial attributes for HIFU therapy guidance. It can provide morphological images for planning and targeting, 15 and MR thermal monitoring allows for the detection of the thermal focus and the measurement of the temperature changes. Therefore, the accumulated applied thermal dose can be calculated and the extent of the tissue damage can be predicted. To finally assess and monitor the size and the shape of the induced tissue lesion at the end of the therapy, CE T1-weighted (CE-MRI) images are employed. The induced lesions prove hypointense, indicating the lack of enhancement and perfusion. 16
The major disadvantage of MRgFUS is the requirement of an MR-compatible HIFU therapy unit and the cost for the MR scanner itself and the MR limitations include limited space for obese patients. 17
Recently, HIFU is used in treatment of bone tumors in China. They found that it is promising modalities of treatment for limb salvage in patients with malignant bone tumors. 18 Other studies used HIFU for treatment of patients with liver, breast, bladder, uterus, and renal tumors with good results. 19 –21
This study was done to look into the effectiveness of MRgFUS therapy for primary bone tumors. Previously, it was thought that the ultrasound waves have minimum ability to penetrate the bone tissue, and furthermore sound waves are attenuated when they are passing through the bone. Hence, sound waves were not suitable for ablation of bone lesion. Smith et al. 22 found that focused ultrasound has the capacity to cause coagulative necrosis in rabbit’s bone. MRgFUS treatment is also associated with enhanced host immune response, 18 and the exact mechanism to this is not yet known.
In this study, we found that MRgFUS was used safely to treat: Benign bone tumors, for which the patients remained pain free and asymptomatic during the study follow-up period. Metastatic bone disease. It gave patients significant pain relief and reduced VAS pain scores. Primary malignant bone tumor, which has significant necrosis based on the post-procedure CE MRI and HPE.
Patients with benign bone tumors, that is osteoid osteoma, were successfully treated with MRgFUS. In this study, it shows to be curative. Therefore, MRgFUS can be further assessed as an alternative to radiofrequency ablation and other forms of noninvasive treatment options.
Patients with metastatic bone disease were successfully treated and had pain relief after the treatment. The MRgFUS provides ablation of the periosteum, which is the pain sensitive area of the bone tumors. It can be an important part of the management of the patients with palliative needs.
In cases of primary malignant bone tumors treatment, MRgFUS can improve the surgical margins prior to resection. Surgical excision still remains the mainstay of treatment for these kinds of tumors. It also has a role in management of unresectable primary bone tumors, to control their growth and progression. MRgFUS can be used as one of the modalities in the multidisciplinary management of primary malignant tumors.
Histopathological analysis for the samples of tumor ablated with MRgFUS showed 100% necrosis but it is impossible to differentiate tissue necrosis due to chemotherapy and the treatment.
The side effects of MRgFUS were used as the safety parameters. The parameters that were analyzed for this study were superficial burns or blisters, fractures associated with the treatment, pain after the procedure, neurovascular dysfunction post-treatment, and any local or systemic side effects. Only two patients had superficial burns and three had significant pain immediately post-procedure with pain score (VAS) more than 6. Other patients remained free of any side effects during the study period.
Overall, the results from this study strongly suggest that MRgFUS is safe and efficacious modality for the treatment of bone tumors.
Limitations
There are few numbers of limitations from this study that can be addressed for further study in the future.
Number of patients
The number of patients recruited for this study was limited due to strict inclusion and exclusion criteria as mentioned in the section “Materials and methods.” The short time period for the study makes it difficult to recruit patients.
Period of follow-up
The duration for follow-up in this study was up to 3 months. This duration is adequate to look at the effect of MRgFUS on the pain relief. Longer follow-up is required to determine the effect of this treatment on underlying disease.
Size of the patient
Two of the patients recruited for the study were not treated with the treatment of MRgFUS due to high Body Mass Index (BMI) as they were unable to fit inside the MRI machine.
Histopathological analysis
HPE of the malignant tumors was not conclusive, as it was difficult to differentiate between the coagulative necrosis caused by focused ultrasound and the necrosis caused by the chemotherapy received by most of the patients. Recommendations Larger sample size for the outcome of safety and efficacy by the MRgFUS treatment. Longer duration for follow-up of patients to enable detection of long-term side effects from the MRgFUS treatment. Structural changes should be made in the MRgFUS delivery system to accommodate more patients regardless of the patient’s BMI.
Conclusion
This is a pilot study for the treatment of MRgFUS for bone tumors, that is, primary malignant tumors, benign tumors, and metastatic bone disease. We can conclude that MRgFUS was able to ablate the benign bone tumors, give pain relief to the patients with metastatic bone disease, and ablate primary malignant bone tumors with significant finding of coagulative necrosis on post-procedure MRI.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.