
Abstract
Purpose:
The purpose of this study is to review the updated evidence comparing outcomes between minimally invasive surgery (MIS) and conventional open surgery (COS) for lumbar spinal stenosis (LSS).
Methods:
All randomized controlled trials (RCTs) published from January 2005 to August 2016 were identified through PubMed and MEDLINE databases. Only RCTs including patients with LSS and with direct comparison between COS and MIS were selected for analysis. The intra- and post-operative effects of different MIS and COS on patients with LSS were evaluated for any differences.
Results:
We reviewed 10 RCTs comparing the effect of MIS and COS for LSS. Most trials showed that MIS rendered a shorter duration of hospital stay, lower reoperation rate, visual analogue scale (VAS), 36-Item Form Health Survey (SF-36) score, creatinine phosphokinase-skeletal muscle (CPK-MM) levels and a higher Japanese Orthopaedic Association (JOA) score. However, the intergroup differences were not statistically significant for all comparisons and were only present for selected mild cases of spinal stenosis.
Conclusions:
This systematic review suggests that MIS reduces operating time, duration of hospital stay and CPK-MM levels. However, the evidence for these parameters is weak. Moreover, there is no conclusive evidence that MIS reduces reoperation or has better improvement in pain and outcome scores like VAS, SF-36 and JOA scores. The evidence is limited due to poor standardization of MIS definition, methodology and details of surgeon experience. MIS techniques should not be studied as a group, as each procedure is vastly different from each other.
Keywords
Introduction
Lumbar spinal stenosis (LSS) was first described by Verbiest 1 in 1954 as a clinical condition with symptoms of nerve root compression on standing or walking but not at rest. LSS was further classified into either developmental or degenerative 2 with the later accounting for a greater proportion of patients. 3 Regardless of the type of LSS, treatment entails a period of conservative treatment including back mobilization, core strengthening, pharmacotherapy and bracing 3 and epidural steroid injections 4 . Surgical intervention is considered if symptoms do not improve with conservative means.
Conventional laminectomy is the surgical gold standard for managing LSS and can achieve satisfactory results in 56–85% of patients. 5 However, proponents of minimally invasive surgery (MIS) have targeted the limitations of this approach including its incision size, traumatic muscle retraction, extensive removal of the posterior spinal structures and possible larger volume of intraoperative blood loss. 6 Damaging the paraspinal muscles and liberal removal of posterior bone may cause iatrogenic spinal instability. In view of these perceived disadvantages, MIS has grown in popularity among spine surgeons treating LSS. It is believed that MIS may limit surgery-related morbidity and mortality by reducing the degree of surgical trauma while maintaining similar surgical outcomes. 7 MIS has been used to describe a wide range of techniques ranging from full-endoscopic interlaminar decompression and microscopic unilateral laminectomy for bilateral decompression to lumbar spinous process-splitting laminectomy.
At this stage, it is important to establish whether MIS techniques are superior to conventional open surgery (COS) in terms of better clinical outcomes, reduced operative trauma and duration and reduced complications. Hence, the aim of this study is to perform a systematic review of the available literature to compare the outcomes of MIS with COS for treatment of LSS.
Methods
Search strategies and selection criteria
Identification of relevant studies was performed by searching PubMed and MEDLINE databases with the keywords: ‘lumbar’, ‘spinal stenosis’ and ‘decompression’. The inclusion criteria were as follows: (1) randomized controlled trials (RCTs) that directly compared MIS with COS; (2) targeted population in the studies were patients with LSS; (3) interventions being compared in the studies were used to treat LSS cases and (4) studies published in English. Studies fulfilling the above criteria but failed to report clinical outcomes were excluded. Two independent reviewers evaluated the titles and abstracts of these remaining papers.
A total of 1844 studies published from January 2005 to August 2016 were found. After narrowing the search results to RCTs published in English only, 120 studies remained. After screening titles and abstracts, another 100 studies were found to fail our inclusion criteria and were excluded. Out of the remaining 20 studies with full-text to be reviewed, 10 were excluded due to duplications. As a result, 10 RCTs were included for analysis in this systematic review. The flow diagram for studies included into the systematic review is summarized in Figure 1.

Flow diagram of studies included into the systematic review. RCT: randomized controlled trial.
Data extraction
Data were grouped into (1) background information of studies (Table 1), (2) intraoperative parameters (Table 2) and (3) post-operative clinical outcomes for comparison and analysis (Table 3). Background information of studies included the number of patients enrolled, the study population, mean age of patients, inclusion and exclusion criteria and interventions involved. Operating time, estimated blood loss and complication rates were the three intraoperative parameters used to compare the effects of different interventions. Due to many variations in post-operative assessment tools used by the included RCTs, only assessment methods used by at least three RCTs were used for analysis. This included duration of hospital stay, reoperation rate, visual analogue scale (VAS) score for leg pain and back pain, 36-Item Form Health Survey (SF-36) score, creatinine phosphokinase-skeletal muscle (CPK-MM) levels and the Japanese Orthopaedic Association (JOA) score. Results of other less common assessment methods were only discussed but not included in the analysis.
Comparison of baseline subjects, recruitment and interventions.

VAS: visual analogue scale; MR: magnetic resonance.
Comparison of intraoperative parameters.

a p < 0.05 compared with bilateral laminotomy.
b p < 0.01 compared with bilateral laminotomy.
Comparison of post-operative parameters.a
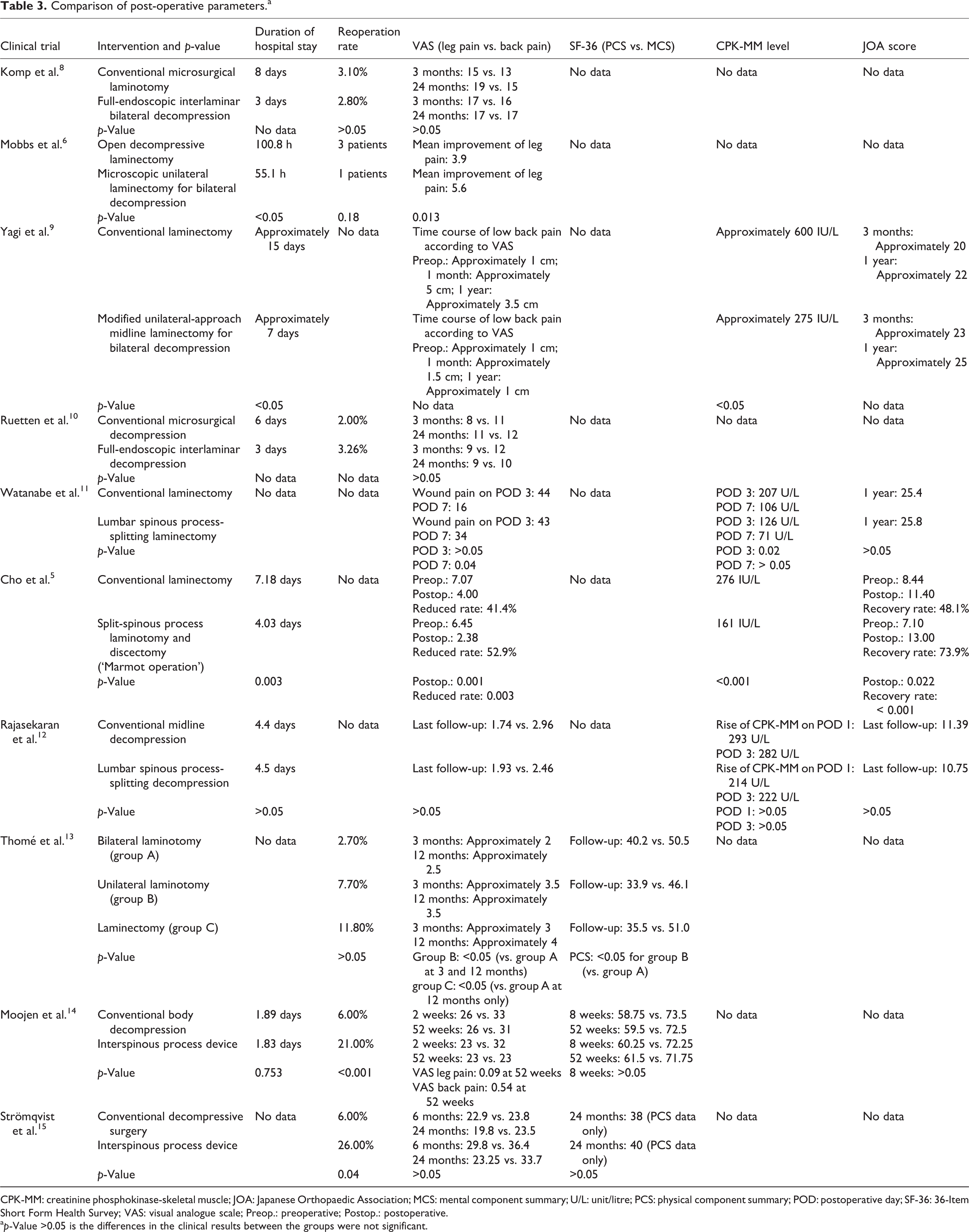
CPK-MM: creatinine phosphokinase-skeletal muscle; JOA: Japanese Orthopaedic Association; MCS: mental component summary; U/L: unit/litre; PCS: physical component summary; POD: postoperative day; SF-36: 36-Item Short Form Health Survey; VAS: visual analogue scale; Preop.: preoperative; Postop.: postoperative.
a p-Value >0.05 is the differences in the clinical results between the groups were not significant.
Statistical analysis
Results of clinical outcomes brought about by MIS were compared to those by COS. Parameters were listed in mean ± standard deviation. p-Value of <0.05 for the intergroup differences were considered statistically significant.
Results
Description of included trials
Ten RCTs comparing the effect of MIS and COS for LSS were included in this systematic review. The number of patients was involved in each RCT ranged from 41 to 192 patients with a mean of 101 ± 54 patients. The average age of patients among all RCTs was 64 ± 6 years old. MIS techniques under comparison in the 10 selected RCTs included full-endoscopic interlaminar (bilateral) decompression, microscopic unilateral laminectomy for bilateral decompression, modified unilateral-approach midline laminectomy for bilateral decompression, lumbar spinous process-splitting laminectomy/decompression, split-spinous process laminotomy and discectomy (‘Marmot operation’), bilateral laminotomy, unilateral laminotomy and interspinous process devices. The COS techniques compared included conventional laminectomy, conventional laminotomy and conventional midline decompression.
Intraoperative parameters
Operating time
Seven RCTs 5,8 –10,12 –14 compared operating time between COS and MIS. Among all measured MIS studies, only full-endoscopic interlaminar decompression and interspinous process devices shortened the operating time when compared to COS. In the RCT conducted by Komp et al., 8 the mean operating time for full-endoscopic interlaminar bilateral decompression was 42 min while conventional microsurgical laminotomy was 64 min In another study by Ruetten et al., 10 the mean operating time for full-endoscopic interlaminar decompression was 34 min as compared to 48 min for conventional decompression. The differences between procedures for these two RCTs were statistically significant. For interspinous process devices, surgery lasted for 23 min while conventional decompression lasted for 43 min and this difference was also statistically significant. 14
Blood loss
Intraoperative blood loss was measured in eight RCTs. 6,8 –11,13 –15 Besides the spinous process-splitting procedures, other MIS procedures rendered less blood loss. Although the differences were insignificant, both split-spinous process laminotomy and discectomy 5 and lumbar spinous process-splitting decompression 12 caused 20 ml more blood loss than conventional laminectomy and conventional midline decompression, respectively. However, no comparison could be made for full-endoscopic interlaminar decompression, as blood loss was not reported due to the authors’ claim of imprecise measurement with continuous irrigation. 8,10
Complication rate
Only five RCTs 6,8,10,13,14 measured the complication rate and only three included the p-value for comparison. Both full-endoscopic interlaminar decompression 8,10 and bilateral laminotomy 13 reduced the complication rate by more than 50% as compared to COS and the differences were statistically significant. Full-endoscopic interlaminar decompression was found to reduce the number of transient post-operative dysaesthesia and urinary retention, epidural hematoma, soft tissue infections and delay in wound healing. 10 In contrast, bilateral laminotomy caused less incidental durotomy, no increased risk of neurological deficit and reduced reoperation rates. 13
Post-operative parameters
Duration of hospital stay
Seven RCTs 5,6,8 –10,12,14 measured the duration of hospital stay after surgery. For all RCTs, MIS reduced the duration of hospital stay as compared to COS. Among the seven RCTs, only three 5,6,9 reported that the differences between the comparison groups were statistically significant. In the study conducted by Cho et al., 5 the duration of hospital stay after split-spinous process laminotomy and discectomy was 4.03 days as compared to 7.18 days for conventional laminectomy. Mobbs et al. 6 reported that the duration of hospital stay after microscopic unilateral laminectomy for bilateral decompression to be 55.1 h and that for open decompressive laminectomy was 100.8 h. In addition, Yagi et al. 9 found the duration of hospital stay after modified unilateral-approach midline laminectomy for bilateral decompression was 7 days, which was approximately 50% less than conventional laminectomy (15 days).
Reoperation rate
Six RCTs 6,8,10,13 –15 reported the results of reoperation rate. Among these, only the intergroup differences in studies conducted by Moojen et al. 14 and Strömqvist et al. 15 were statistically significant. In both RCTs, interspinous process devices led to a reoperation rate of more than 20% as compared to 6% for conventional decompression. Also for all MIS techniques compared, only interspinous process devices led to a higher reoperation rate.
VAS score
All selected RCTs used the VAS score to assess the clinical outcomes of MIS and COS. Four of 10 RCTs reported no significant intergroup differences. 8,10,12,15 Mobbs et al. 6 reported that patients who underwent microscopic unilateral laminectomy for bilateral decompression had a better mean improvement in leg pain with a significant intergroup difference as compared to conventional open laminectomy. Watanabe et al. 11 focussed on wound pain using VAS scores and found that significant intergroup differences in wound pain were only observed on post-operative day 7.
36-Item form health survey
Only three RCTs used SF-36 as an objective clinical outcome measure. 13 –15 Moojen et al. 14 and Strömqvist et al. 15 reported no statistically significant intergroup differences for both physical and mental component summaries. However, Thomé et al. 13 found that unilateral laminotomy rendered a statistically better result than bilateral laminotomy in the physical component summary.
CPK-MM levels
Four RCTs measured post-operative CPK-MM levels. 5,9,11,12 Yagi et al. 9 reported that patients who underwent modified unilateral-approach midline laminectomy for bilateral decompression had a post-operative CPK-MM level of 275 IU/L as compared to 600 IU/L for conventional laminectomy. Cho et al. 5 found that the post-operative CPK-MM level for split-spinous process laminotomy and discectomy was just 161 IU/L, compared to conventional laminectomy, which was 276 IU/L. These differences found in both studies were statistically significant. Watanabe et al. 11 also reported similar findings but the statistically significant intergroup differences were only observed on post-operative day 3 with a post-operative CPK-MM level of 126 IU/L in lumbar spinous process-splitting laminectomy and 207 IU/L in conventional laminectomy. In contrast, Rajasekaran et al. 12 measured the rise of CPK-MM levels only on post-operative day 1 and day 3 for lumbar spinous process-splitting decompression and conventional midline decompression and found no statistically significant intergroup differences on both days.
JOA score
JOA score was used by four RCTs as their clinical objective assessment tool. 5,9,10,12 Cho et al. 5 reported a post-operative JOA score of 13 for split-spinous process laminotomy and discectomy as compared to 11 for conventional laminectomy. This RCT also compared the post-operative score with the pre-operative score and found out that the recovery rate was 73.9% for split-spinous process laminotomy and discectomy as compared to 48.1% for conventional laminectomy. Both differences were statistically significant. Yagi et al. 9 who studied microendoscopic decompression did not provide the p-value for their results and thus the advantages seen with their MIS technique could not draw any substantial significance. Other studies such as Watanabe et al. 11 reported a 1.4 times greater post-operative JOA score for lumbar spinous process-splitting laminectomy than conventional laminectomy while Rajasekaran et al. 12 reported that lumbar spinous process-splitting decompression had a post-operative JOA score of 10.7, which was 0.6 lower than conventional midline decompression. These findings were not statistically significant. Outcome scores were hence variable without any clear advantage identified between MIS and COS.
Other outcome measurements
Apart from the six post-operative parameters mentioned, there were also other parameters included in the selected RCTs but were not included for analysis since they were used by less than three RCTs. Mobbs et al. 6 reported that microscopic unilateral laminectomy for bilateral decompression had a greater mean improvement in Oswestry disability index (ODI) than open decompressive laminectomy (28.6 vs. 17.8) but the intergroup differences were not statistically significant. This study also could not find significant differences in the 12-Item Short Form Health Survey (SF-12) between MIS and COS. The mean improvement in SF-12 score for the physical component summary was 40.1 for MIS but was 40.2 for COS while the mental component summary for MIS and COS was 50.2 and 47.1, respectively. However, the intergroup differences for the mean improvement of both physical component summary and mental component summary were not statistically significant.
Patient satisfaction index (PSI) score was used by Thomé et al. 13 for comparing bilateral laminotomy, unilateral laminotomy and laminectomy. PSI was a modified sub-item of the North American Spine Society outcome questionnaire, which included items asking whether patients were satisfied with post-operative pain reduction and the improvement in ability to perform daily activities. Bilateral laminotomy had the highest PSI score in the post-operative 3-month, 6-month and 1-year follow-up assessments. After 3 months of surgery, the PSI score for bilateral laminotomy was 94.6, which was significantly better as compared to unilateral laminotomy. At post-operative 1 year, the PSI score for bilateral laminotomy increased to 97.3 which was significantly better than unilateral laminotomy (74.4) and laminectomy (73.5).
Watanabe et al. 11 and Rajasekaran et al. 12 measured the level of C-reactive protein (CRP). In the former RCT, a significant difference was only recognized between lumbar spinous process-splitting laminectomy (1.1 mg/dl) and conventional laminectomy (1.9 mg/dl) on post-operative day 7. In the latter RCT, no statistical differences in mean CRP level were observed between lumbar spinous process-splitting decompression and conventional midline decompression on both post-operative day 1 and day 3.
Atrophy rate of paravertebral muscles measured by T2-weighted axial magnetic resonance images was recorded by Yagi et al. 9 and Watanabe et al. 11 Both found that the atrophy rate was lower in the group of patients who underwent MIS and the intergroup differences were statistically significant. It was believed that the lower atrophy rate contributed by MIS was due to reduced damage to paravertebral muscles which could preserve spinal stability.
Discussion
Based on only a small sample of RCTs, there is a clear advantage of MIS techniques over COS with regard to intraoperative parameters including operating time, blood loss and complication rate. Although this advantage is statistically significant, the actual reduction of operating time and blood loss is only by approximately 10–15 min and 20 ml, respectively. Thus, the differences may not be clinically significant. Furthermore, it is unclear whether this operating time included preparation time and instrument setup, such as endoscope and monitor connection, which may be longer in MIS techniques. Comparisons are also difficult due to the various procedures discussed. Each procedure is fundamentally different and with variable operation duration. Similarly, the actual blood loss may be underestimated since it is difficult to measure blood loss due to continuous irrigation. Moreover, for endoscopic surgery, blood loss cannot be accurately measured and is usually estimated by the operating surgeon.
For post-operative outcomes, the main advantages of MIS as described were duration of hospital stay and lower CPK-MM levels. MIS techniques generally reduced the duration of hospital stay by approximately 2–3 days. This value may be subjected to variations in institutional practices, patient’s general health condition and the post-operative analgesics protocol, which were not discussed in the studies. Hence, it cannot be generalizable to all practices. Nonetheless, this is a relevant and important finding that may have significant impact on cost comparisons between techniques. This cost concern should be addressed in future work. Most studies concur with reduced CPK-MM levels in MIS procedures. Although the difference is significant between the two techniques, its clinical impact is unknown. Correlation between severity of back pain, mobility and core strength should be addressed to highlight the significance of this finding.
The most important outcome measure in spinal stenosis treatment is symptom resolution. Our review suggests that there is no clear advantage of MIS with regard to VAS, SF-36 or JOA scores. Hence, both MIS and COS can achieve adequate decompression and symptom relief. This statement, however, may not be applicable to all cases of LSS. One of the major limitations of the included RCTs is the unknown nature of severity of stenosis. In more narrowed spinal canals, the ability of some techniques to achieve adequate decompression may be limited.
Despite the growing popularity of MIS in management of LSS, conclusive evidence for its superiority over COS is lacking which is highlighted in this systematic review. The reasons for lack of conclusive evidence include the definition of MIS, no standardized methodology to assess outcomes, variations in patient selection and surgeon experience.
A lack of consensus with regard to the definition for MIS leads to a difficulty in systematically comparing MIS techniques with COS. The nature of surgical techniques varies in the 10 RCTs selected. Komp et al. 8 and Ruetten et al. 10 studied a full-endoscopic approach. Mobbs et al. 6 and Yagi et al. 9 studied unilateral laminectomy for bilateral decompression and this MIS technique only involved bony and soft tissue disruption on one side. This is in comparison to Watanabe et al., 11 Cho et al. 5 and Rajasekaran et al. 12 who performed spinous process-splitting approaches. Moreover, Cho et al. 5 performed laminotomy with discectomy while the other two RCTs adopted laminectomies. Both Moojen et al. 14 and Strömqvist et al. 15 used interspinous process devices which may be considered as an MIS technique but provides only indirect decompression. Grouping interspinous process devices with other techniques may underestimate the benefit of MIS due to their higher reoperation rates. There is also variation between the two studies. Strömqvist et al. 15 inserted the spacer under local anaesthesia while Moojen et al. 14 inserted it under general anaesthesia. This may lead to differences in pain scale and duration of hospitalization. The study by Thomé et al. 13 was the only study comparing COS with two MIS techniques, unilateral laminotomy and bilateral laminotomy. Differences in the nature of these surgeries rendered different intraoperative and post-operative outcomes. Therefore, better clarity is required when describing these ‘less-invasive’ techniques as procedures can be vastly different with variable effects on outcome measures. In addition, not all studies published with the term ‘MIS’ included a technique that adopted a smaller incision with less muscle dissection and soft tissue trauma.
Lack of standard methodology for assessing outcomes in these studies has reduced the significance of their findings. The only consistent parameters studied were the duration of hospital stay; reoperation rate; VAS, SF-36, and JOA scores and CPK-MM levels. Many other parameters including commonly used objective scoring questionnaires such as the ODI and SF-12 cannot be used for analysis. It is expected that reporting bias may be present in the selected RCTs without a consistent list of outcome measures studied.
Variations in patient selection have also limited the ability to make a fair comparison between MIS and COS. Firstly, most of the sample populations were small and at times not reported. Mobbs et al. 6 included 79 patients without data regarding gender distribution while Yagi et al. 9 and Watanabe et al. 11 included 41 patients only. With LSS being such a common surgical disorder, seeing such small sample sizes questions the patient recruitment process of these RCTs. Moreover, different inclusion and exclusion criteria have been used thereby recruiting a heterogeneous population for comparison between the selected RCTs. Mobbs et al., 6 Thomé et al. 13 and Moojen et al. 14 excluded patients who required discectomy while Cho et al. 5 included them. Since discectomy is specific for managing prolapsed intervertebral disc, this procedure is not routinely performed for spinal stenosis. Its inclusion in a RCT format will yield unfair comparisons between MIS and COS since some MIS techniques cannot tackle both the disc and hypertrophied ligamentum flavum and facets.
MIS procedures utilize relatively innovative techniques and thus have a steep learning curve. The surgeon’s experience may play an important role in the patient’s surgical outcomes. However, none of the selected RCTs specified the details of the experience of the participating spine surgeons. With some of the RCTs based on well-known MIS centres, the results presented may be an unrealistic representation of the true differences between the two approaches. Those who only perform MIS may not be as capable as others who perform COS and vice versa. Hence, better indication of the surgeon experience is necessary.
One of the major concerns with this systematic review is the inclusion of interspinous spacers. Although this is still considered as an ‘MIS’ technique, the indication of surgery may be different from other RCTs. As spacers are only able to provide indirect decompression, patients must only have mild stenosis to have adequate symptom relief with this procedure. Patients with moderate-to-severe spinal stenosis, spondylolisthesis, more significant disc degeneration or facet hypertrophy will not experience much symptomatic relief with these spacers. The procedure may even aggravate the degenerative process with further disruption of the posterior ligamentous complex. Hence, the range of clinical pathologies treatable with interspinous spacers is very narrow. The procedure also requires only a small exposure to insert the device and will undoubtedly result in shorter operative time and less blood loss. Hence, it may not be fair to compare this group of patients with other decompression methods. Nevertheless, the variability in the results shown was not exclusive to interspinous spacers and whether there is a clear advantage of MIS over COS in terms of outcome measures is unclear.
Conclusions
The current available evidence favours MIS for less operating time, intraoperative blood loss and shortened hospital stay. However, this supporting evidence is weak and highly flawed. Furthermore, no conclusion can be drawn regarding the post-operative outcomes. Results may be technique specific and MIS cannot be generalized as a whole. MIS procedures should not be studied as a group as each individual technique is vastly different in indications, learning curve, perioperative risks and postoperative outcomes. Future studies should utilize standardized definitions, methodologies and assessment parameters.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.