
Abstract
In the past decades, an increasing number of surgeons started using posterior vertebral column resection (PVCR) to treat severe, rigid and angular spinal deformities. Little high-level evidence is available to guide surgical treatment. The aims of our study were to identify important surgical strategies and key technical points of Chinese experts who have extensive experience in the management of severe, rigid and angular spinal deformities using PVCR, and to standardize and unify the current core concepts. Workgroups of consensus were formed by selecting nationwide representing experts and comprehensive consultations. Eight task forces for major issues were established, then retrieval of literature, collection of expert opinions and writing of review articles were carried out. A modified Delphi process was chosen in round-table forum with three face-to-face meetings. Consensus was reached with items graded more than seven points including: indications and contraindications of PVCR; review PVCR in the evolution of spinal osteotomies; The corrective mechanism and safety of spinal cord; monitoring and responses of spinal cord crisis; characteristics and therapeutic outcome of pulmonary function; management of bleeding during PVCR; relationship of pedicle screw insertion and spinal cord safety; and analysis of non-neurologic complications and prevention strategies. In conclusion, The essential properties regarding PVCR procedure are tightly linked with various factors such as medical and surgical indication, range and level of vertebral column resection, strategies of correction, corrective efficiency and control of neurological risk. PVCR is used mainly for severe, rigid spinal deformity that is not manageable by other osteotomy techniques.
Introduction
In the last century, severe, rigid and angular kyphoscoliosis (Figure 1) and severe kyphosis (Figure 2) were considered to be insurmountable problems for spinal correction surgery. Despite the great efforts made by spine surgeons in exploring effective solutions, the frustrating corrective outcomes, high incidence of neurological complications and massive bleeding were major threats to various spinal correction procedures and technologies. Since posterior vertebral column resection (PVCR) was reported by Suk et al. to be effective in the management of severe, rigid spinal deformity in 2002, 1 PVCR has been carried out successively at many spinal deformity centres in China. Until now, owing to social and historical developments and its large population, China has been one of the countries that has the largest number of patients suffering from such severe spinal deformities, that are treated by PVCR procedures. Moreover, with satisfactory clinical outcomes and lower incidences of neurological complications, systemic research on PVCR has been carried out by Chinese experts with extensive clinical experience. In addition, over the last decade, the remarkable achievements of Chinese surgeons have been presented via many international conferences and journals, and spinal surgeons around the world have been attracted to the Chinese experts’ depth and range in the treatment of severe, rigid and angular spinal deformities.

Severe kyphoscoliosis.

Severe angular kyphosis.
However, the application and popularization of PVCR were obstructed by many challenges and risks. These included complicated surgical procedures, the need for higher surgical skills, various spinal deformities and patients’ condition and different levels of understanding and proficiency of this technique among surgeons. At present, interpersonal learning and communication among novice practitioners are restricted by confusing concepts and lack of unifying identities for core concepts and key technologies of PVCR. The common problems include, for example: How to define ‘severe’ and ‘rigid’ spinal deformities? What is the indication for PVCR? With regard to the range of resection and principle of deformity correction, what is the essential difference between PVCR and other spinal osteotomy techniques? From where does the risk of spinal cord injury arise and how can it be prevented from happening? What should we do if it occurs? How can bleeding during the operation be controlled?
The aims of the Kunming round-table forum are to summarize the salient points of the treatment experiences of national experts who have extensive experience in the management of severe, rigid and angular spinal deformities using PVCR; to standardize and unify the current core concepts; and to reach a consensus for important surgical strategies and key technical points. The achievements of this forum will be presented as an expert consensus to greatly improve the ability of spinal surgeons in the management of severe and rigid spinal deformities.
The preparations of the conference were made as follows: (1) selecting the participating experts who have the right to vote and speak: those domestic experts who have reported their experience in the treatment of severe, rigid and angular spinal deformities using PVCR in international and/or national journals and at professional meetings were identified through the China National Knowledge Infrastructure database, WANFANG Academic Search System and PubMed database retrievals; (2) following interactions with those experts by email, phone or face-to-face communications, workgroups of consensus were formed with positive responses and directions of the specialists; and (3) eight major issues were established in the treatment of severe, rigid and angular spinal deformities using PVCR, following communications with the experts: (a) the indications and contraindications of PVCR in the treatment of spinal deformities; (b) evaluation of PVCR in the evolution of spinal osteotomies; (c) spinal cord protection during PVCR; (d) spinal cord crisis during PVCR – monitoring and feedback; (e) characteristics and therapeutic outcome of pulmonary function in patients with severe, rigid spinal deformities and respiratory dysfunction; (f) controlling bleeding during PVCR; (g) pedicle screw implantation and spinal cord protection during PVCR; and (h) analysis of non-neurologic complications and prevention strategies during PVCR.
Three months before the round-table forum, scholars in the workgroup were divided into eight task forces, each composed of two to three panellists. Each task force was responsible for one major issue. Retrieval of international and domestic literature, collection of expert opinions and writing of review articles were carried out by the task forces. Academic and clinical values and consistency with other issues were censored by the experts. A weekly working group meeting was held to discuss the opinions and suggestions of each task force and solve specific problems. The draft of consensus was composed based on substantial literature support and full communication with the experts.
Method for consensus
Currently, three methods are considered to reach consensus in the medical field: the Delphi process, the Nominal Group Technique (NGT) and Consensus Development Conference. In recent years, the RAND-UCLA (RAND Corporation-University of California Los Angeles) method obtained from the Delphi process and NGT was considered more seriously. According to the clinical and consensus guideline of the World Health Organization, the modified RAND-UCLA was chosen for this conference 2 (Figure 3).
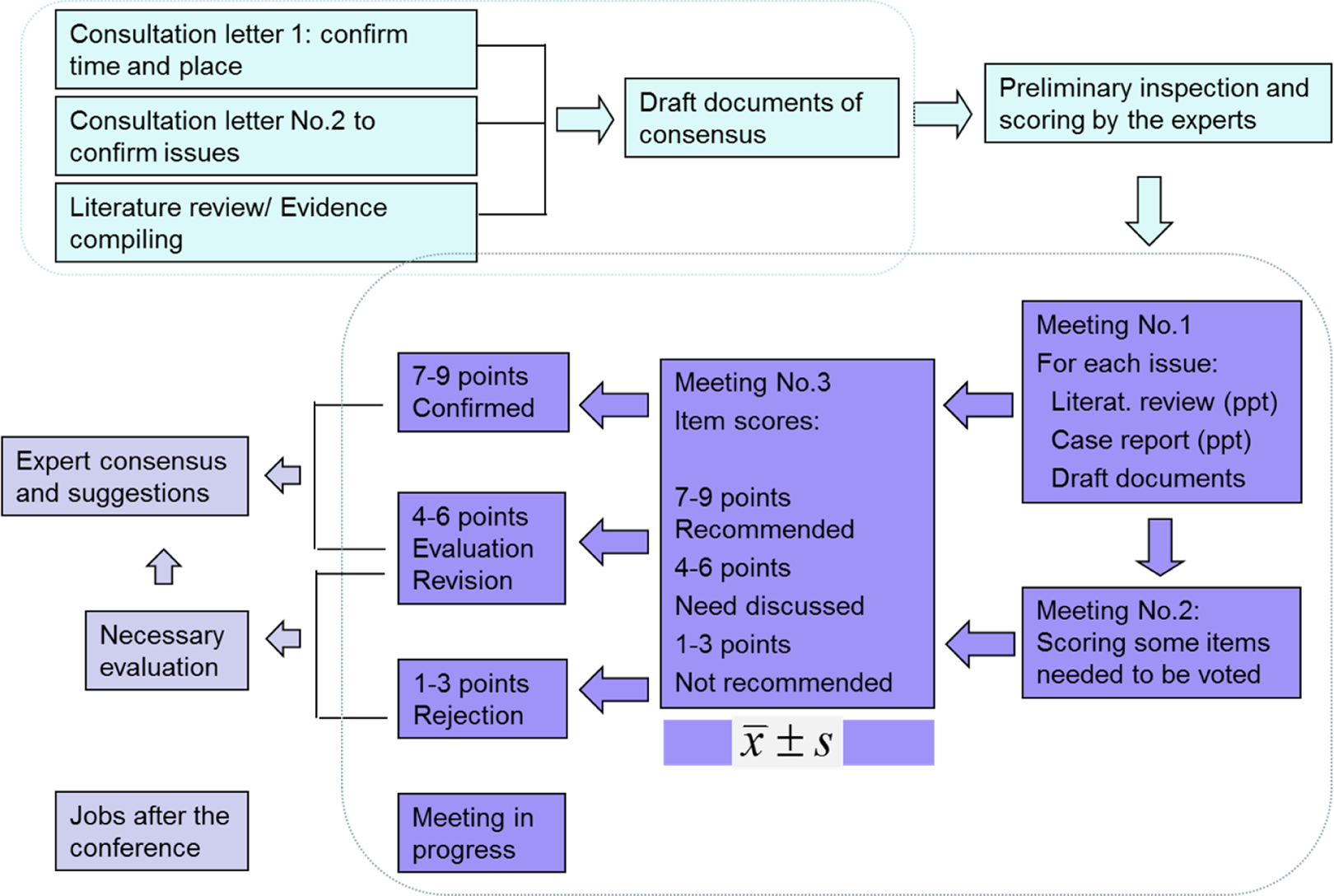
Processes of the experts’ consensuses.
To reach consensus on the treatment of severe, rigid and angular spinal deformity using PVCR, the round-table forum was held on 11 June 2016, in Kunming. Each issue of the conference was discussed as follows: (1) the related literature review and background of each item were given by the scholar of the task force; (2) lecture on interpretation of this issue was made by one or two panellists nominated beforehand by the expert group; (3) support for and objections to the items were elaborated in the form of case reports by the panellists nominated beforehand by the expert group; (4) the items were stated and discussed one by one and then the adopted items were revised; (5) degree of approval by the expert: electronic voting machines were used to ensure the confidentiality. The final consensus was reached according to the items and their descriptions discussed and revised by all the participating experts.
After the meeting, a first draft of the consensus was compiled and printed by the workgroup, which was then posted to each expert for re-examination and revision. The review was based on degree of approval, strength of recommendations and level of evidences. The comments of the review with the strength of recommendations of each item were collected by the workgroup, and the consensus with its descriptions was finalized by the workgroup, adding the latest literature evidence. A score of 1–9 points was used in the judgement of the recommendation, with higher scoring indicating higher strength. The strength of recommendation for each item was expressed as mean ± standard deviation. For the purpose of further guidance, items graded less than seven points after discussion were not recommended and were deleted from the final consensus.
Limitation
There were some limitations of methodology in the programme. First, as with any Delphi-based method, the consensus was based on experts’ opinion and on the assumption that several people with diverse backgrounds agree on an issue. Even though we employed panellists and experts through literature screening and full exchange of information, we may not have represented all caregivers. Second, although all participating experts or group members had extensive experiences in clinical practice, the programme was geared toward all participation in evidence analysis, and consensus has been achieved by online documental files and pre-meeting lectures. For the limitation of education background, the lack of an interactive evidence-based medicine training course may lead to a bias of systematic evaluation of literature and judgement of the items.
Part 1: The indication and contraindication of PVCR
Background
In the past decades, an increasing number of spinal deformity surgeons started using PVCR to treat severe, rigid and angular spinal deformities. 3 PVCR has replaced the traditional circumferential VCR and can correct spinal deformity more effectively than other correction techniques such as Smith–Petersen osteotomy (SPO) and pedicle subtraction osteotomy (PSO). However, it is a complex and risky technique and can pose a great challenge to the surgeons and patients. The surgeons involved in correcting spinal deformity using PVCR need strict and appropriate indication and contraindication to make an optimal surgical choice. For this reason, the definition of the ‘severe, rigid and angular spinal deformity’ is significant in the decision-making of PVCR.
Consensus
1. PVCR is often the first choice for treating the severe, rigid kyphoscoliosis, angular kyphosis and other deformities that can’t be corrected by other osteotomies (strength of recommendation 7.65 ± 1.57).
SPO and PSO are mainly used to correct sagittal plane deformities and can achieve limited correction in the coronal plane. However, they cannot be used to correct severe, rigid kyphoscoliosis and angular kyphosis. With PVCR, we can correct the spinal deformity more effectively, which the other osteotomy techniques can’t achieve; however, with PVCR the surgical risk is much higher than that of other techniques. For this reason, PVCR is used mainly for spinal deformities that cannot be corrected by other methods.
2. By ‘severe’ spinal deformity, we mean that the Cobb angle of the main curve is more than 90° in the coronal plane and/or more than 90° in sagittal plane (strength of recommendation 7.80 ± 1.32).
3. By ‘rigid’ spinal deformity, we mean that the flexibility of the main curve is less than 20% (strength of recommendation 7.22 ± 2.35).
In ‘severe rigid’ spinal deformity, the spinal deformity involves a very large Cobb angle and poor flexibility. The use of the terms ‘severe’ and ‘rigid’ in the literature are notoriously obscure. Their definitions are constantly updated with the development of the corrective technique and the surgical devices. Nowadays, according to the literature, in severe spinal deformity the Cobb angle of the main curve is more than 80–100°, and in rigid spinal deformity the flexibility of the main curve is less than 10–30%. 4,5 A consensus about the definition of severe and rigid spinal deformity offers a clinical and research baseline to the spine surgeons all over the world.
4. The ‘angular’ spinal deformity means:
a sharp angle with remarkable structural abnormalities of vertebral column in the apex of the curve; a small number of vertebrae involved in the curve; and magnetic resonance imaging scan shows that the spinal cord is angular in the apex area (strength of recommendation 7.50 ± 1.37).
For over a century, the term ‘angular’ has been used to describe a spinal deformity, 6 and it is used to describe spinal deformity with a sharp angle involving a small number of vertebrae in the curve. Angular spinal deformities are mainly used to describe the curve with kyphosis and sometimes scoliosis. Remarkable structural abnormalities of vertebral column in the apical area of those spinal deformities are observed. However, spinal surgeons seemed to be more concerned about the angular deformity of the osseous structure rather than the deformity of the spinal cord, which has a real impact on the surgical strategy and the risk.
5. Excision of hemivertebra associated with a mild spinal deformity cannot be considered equal to PVCR (strength of recommendation 7.45 ± 1.97).
In the mild spinal deformity caused by the hemivertebra, the spine does not totally lose stability after the excision of the hemivertebra, which can be corrected by closing the gap obtained from the hemivertebra excision. Based on the concept of correction, correction skill, risk to the spinal cord, surgical trauma and complexity of operation, excision of hemivertebra is definitely not equal to PVCR. 4
6. The following are the contraindications of PVCR.
Absolute contraindication
Poor basic medical condition of the patient: heart failure and type II respiratory failure.
Patient and the families can’t accept the potential risk and complications accompanying PVCR.
Relative contraindication
The pedicles of the vertebras adjacent to the osteotomy are poor, and sufficient screws cannot be inserted into the pedicle of the cranial and caudal vertebras adjacent to the resection level to maintain the stability of the spine.
Type I respiratory failure.
Poor nutritional status of the patient who can’t bear the surgical trauma of PVCR.
The surgeon is not familiar with PVCR or the surgeon can’t perform the PVCR with expertise (strength of recommendation 7.32 ± 1.39).
The PVCR is a powerful correction technique for severe, rigid and angular spinal deformity, but the risk of the operation is high. It is the last-resort procedure for patients with severe, rigid spinal deformity. The surgeon should seriously consider this procedure and whether he can ensure the safety of the spinal cord and the life of the patient. Poor basic medical conditions, such as heart failure, severe restrictive ventilation disorder, respiratory failure and poor nutrition, can increase the rate of the complications and mortality. Furthermore, insufficient screws inserted into the pedicles of the cranial and caudal vertebras adjacent to the resection level are dangerous to the spinal cord. One must be clearly aware that the PVCR should not be performed if there is a lack of a harmonious team including surgeon and anaesthesiologist or if the surgeon is unfamiliar with the procedures of PVCR or can’t perform it expertly. The PVCR should not be performed if the patient and family members cannot accept the potential risks and complications.
Part 2: To review PVCR from the evolutionary history of applying spinal osteotomy to correct spinal deformity
Background
For severe, rigid spinal deformity, not only the huge curvature but also the lack of flexibility makes it difficult to correct the curve safely and directly by usual methods. Therefore, while correcting these deformities, it is important to make the rigid spine more ‘flexible’ through posterior or/and anterior approaches, which enable spinal osteotomy to move forward. In 1945, Smith-Petersen et al. 7 first reported the use of SPO technique to correct kyphosis in ankylosing spondylitis (AS) patients. Thereafter, different techniques of spinal osteotomy, such as PSO, PVCR and so on, were introduced, which made great breakthroughs in the treatment of severe, rigid spinal deformities. 1,8 –10
In the past 70 years, the field of spinal osteotomy has experienced a complex evolutionary process. The SPO technique, the basic form of spinal osteotomy, is responsible for the breakthrough in the treatment of ‘round’ kyphosis such as AS. At that time when there was no modern spinal instrumentations, the use of the SPO technique to correct these spinal deformities was regarded as a ‘magnificent feat’. However, SPO was only suitable for patients presented with smooth round deformities in the sagittal plane, but it could not safely and effectively correct more severe and complex spinal deformities. In 1985, Thomasen reported the use of PSO in more severe and complex sagittal deformity, again enabling a forward movement in the field of spinal osteotomy. Meanwhile, the limitations of the PSO techniques in treating much more severe and complex spinal deformities also demand a further improvement in spinal osteotomy. From the developmental history of spinal osteotomy, each new osteotomy technique was an attempt to further explore new techniques that could not be solved by the previous techniques. Nowadays, with comprehensive application of different osteotomies, spinal surgeons can treat the most challenging patients with severe, rigid and angular kyphoscoliosis.
In the past 10 years, spine surgeons not only tried their best to increase the correction rate in one dimension but also pursued balance in three dimensions, a more satisfactory outcome and a decrease in the neurological risk during correction. Therefore, different kinds of spinal osteotomies were reported successively, such as closing–opening wedge osteotomy (COWO), 11 asymmetrical PSO, 12 vertebral column decancellation, 13 posterior multilevel vertebral osteotomies, 14 PVCR and so on.
COWO abandoned the PSO technique ‘bone-on-bone contact’ in order to decrease the potential neurological risk during correction, to achieve solid reconstruction of anterior and middle columns and to promote the corrective and fusion rates. Unfortunately, still there are several disadvantages in correcting severe, rigid kyphoscoliosis by COWO, which would be surmounted by the introduction of PVCR technique as reported by Suk et al. 1 The introduction of PVCR made possible the correction of severe, rigid spinal deformity, becoming the last resort for these patients. The PVCR was introduced based on the result from the demands of the patients and the efforts of the spinal surgeon to challenge the difficult and complex spinal deformities.
Consensus
7. Being different from PSO, PVCR has unique corrective features and mechanisms with different optimal indications (strength of recommendation 7.96 ± 1.19).
PSO is often used to correct the spinal deformity predominantly on the sagittal plane, which is achieved through closing the osteotomy gap with limited coronal correction. Because of its risks caused to the spinal cord, PSO is often performed in the thoracic–lumbar or lumbar vertebrae in order to improve the sagittal imbalance or directly to correct part of angular kyphosis. PVCR is especially suitable for severe, rigid kyphoscoliosis or severe angular deformities.
8. One or more vertebrae are fully resected using PVCR, including adjacent intervertebral disks, in order to create space for correction; the separated spine is connected only by the spinal cord and its stability is maintained by internal fixation completely; with regard to spinal cord safety during correction, the extent of vertebral resection using PVCR is mainly related to the severity of spinal deformity (strength of recommendation 8.25 ± 0.85).
Using PVCR, one or more vertebrae with adjacent disks are resected completely in order to achieve 360° circumferential decompression of the cord. Any residual disk or bony structures would cause compression of the spinal cord or nerve root. During PVCR, the artificial space created by complete resection of vertebrae enables observation, evaluation and control of the tension of spinal cord. To meet the requirements of correction and to maintain neurological safety, the number of resected vertebrae should be as low as possible. The excessive residual space after correction would have a negative effect on reconstruction, subsequent fusion and long-term outcomes.
9. During the PVCR procedure, spinal shortening performed each time reduces the tension of the spinal cord, and the aim is not only to focus on correction directly but most importantly to perform a further correction under a moderate lower tension of the spinal cord (strength of recommendation 8.09 ± 1.35).
Being different from PSO, the correction using PVCR starts with spinal shortening, which is directly aimed not only at correction but to achieve a safe corrective procedure under a moderately lower tension of the spinal cord, thus keeping it away from any higher tension. In the corrective process, this can be performed repeatedly so that the spinal cord is not exposed to increased tension. At the end of correction, a reserved gap will be kept without closing.
At the end of correction, it is important to retain a residual circumferential space in the cord to (1) avoid direct compression of spinal cord/dural sac from osteotomy ends, (2) decrease excessive stacking of spinal cord/dural sac, (3) reserve space for the compliance change in the cord following the subluxation of the spinal ends after osteotomy and (4) benefit for effective and reliable support and for reconstruction of anterior and middle column by utilizing this space.
10. The resection of vertebrae and discs in PVCR should be careful and cautious enough, especially in the case of severe, rigid kyphoscoliosis; and the exposure and resection of the pedicle on the concave side would be one of the most difficult steps (strength of recommendation 7.32 ± 1.58).
While using PVCR to correct severe, rigid kyphoscoliosis, it is difficult to expose and resect the pedicle on the concave side because of the higher grade rotation of the apical vertebrae and the sclerotic articular process with malformation of pedicles. Hence, this process should be done in a cautious manner.
11. The residual space after PVCR correction needs structural reconstruction, which will be important to prevent internal fixation failure and loss of correction (strength of recommendation 7.32 ± 1.58).
At the end of correction using PVCR, the residual corrective space should be reconstructed: if the distance interval between the two osteotomy ends is more than 10 mm, it is recommended to use structural bone grafting with titanium mesh; if the distance is less than 10 mm, it is recommended to use structural bone grafting with autograft. The residual space after structural bone grafting was filled with cancellous bone graft to increase the area and density of grafting. 4
12. Of all kinds of spinal osteotomies, the use of PVCR is considered to have greater challenges and risks with higher technical demands and difficulties. And the choice of PVCR should be made cautiously (strength of recommendation 8.75 ± 0.44).
Both PSO and PVCR are three-column osteotomies. But as reported by the history review of spinal osteotomy, PVCR is much more aggressive owing to its more complicated mechanism, higher technical difficulties and increased technical demands compared to PSO and other trans-vertebral osteotomies. According to the 2011 Mortality and Morbidity report of the Scoliosis Research Society, the total rates of complications in SPO, PSO and PVCR were 28.1%, 39.1% and 61.1%, respectively. 15 Therefore, the choice of PVCR should be the last resort in the treatment of severe, rigid kyphoscoliosis, owing to its greater risks and challenges.
Part 3: The corrective mechanism and the safety of spinal cord
Background
Spinal osteotomy is a kind of surgical procedure involving a high-risk neurological impairment. The core problem in using spinal osteotomy to correct spinal deformities is the safety of neurological structures. Throughout the 70-year history of spinal osteotomy, the treatment extent of deformity has been widened from the simple round kyphosis in the past to the severe, rigid and angular kyphoscoliosis at present; the extent of resection has been enlarged from the posterior column only at the earlier stage to partial or total resection of the whole vertebrae 16,17 ; the resected location has been extended from the lumbar vertebrae initially to thoracic or even cervical vertebrae; the corrective effects have also been pursued from increasing the corrective rates initially to improve the three-dimensional (3D) corrective effects at present. However, following the enlargement of vertebral resection and the increasing severity of deformity, there are much higher risks to spinal neurological structures. In the three-column spinal osteotomies, the neurological complications related to PSO were up to 7.0–14.3%, 15,18 whereas it was 5.7–27% in PVCR. 19,20 Hence the problem of neurological protection existed in each stage of spinal osteotomy, and every leap in spinal osteotomy with regard to the neurological safety will certainly be a significant breakthrough.
SPO correction is based on the posterior column resection followed by closing the posterior gap by opening the anterior intervertebral disks. Thus, PSO is achieved through wedge osteotomy by extending posterior column to part of middle and anterior columns in order to achieve correction, thereby closing the wedge gap. Therefore, irrespective of SPO or PSO, the corrections are achieved through closing the posterior gap after osteotomy. For these two osteotomies, achieving an increased angle of correction means to essentially enlarge the extent of vertebral resection. Following this, when the enlarged gap from extended osteotomy is closed, the stacking of spinal cord will threaten neurological safety. Corrections done using SPO and PSO involves closing osteotomy gap, shortening posterior column and stacking the spinal cord . The more the corrective rate, the higher the risk to the spinal cord. So if simply closing gap and shortening posterior column are being used in surgical management of severe kyphoscoliosis, the risks for the spinal cord would not be avoided. With further understanding of PSO, spinal surgeons began to recognize that pursuing ‘bone-on-bone contact’ in the wedge gap after osteotomy would cause excessive stacking of the cord and is a risky factor for neurological damage. Through complete resection of a vertebral segment and supporting middle column with a titanium mesh, COWO technique reduces the risk of spinal cord stacking from excessive spinal shortening and also achieves a better corrective effect on the sagittal plane. 21 And COWO could be considered as a transitional stage from PSO to PVCR. Considering the safety of spinal cord, the history of spinal osteotomy is also an evolutionary story of the spinal surgeons’ deep thinking about the neurological risks and protection related to corrective method.
In spinal osteotomies, the risks to the spinal cord could be related to several aspects 22 : from specific aetiology to morphological characters, from internal instrumentation insertion to vertebral resection and from corrective procedure to reconstruction, each step or procedure would face potential neurological risks. According to the resources, these neurological risks could be divided into two categories: primary and iatrogenic factors. The primary factors include aetiology, morphological characters (curve degrees, apical sites, with or without intraspinal malformation, etc.). The iatrogenic factors involve several aspects of surgical process. Effective control of the risks related to the procedure will help spinal surgeons to mitigate disastrous neurological complications.
Consensus
13. The source of neurological risks during spinal osteotomy mainly includes:
Pedicle screw insertion, both higher and excessive lower tension of the spinal cord related to corrective procedure, preoperative neurological deficits, morphological character of curves, degree of main curve, intraspinal malformation, corrective manoeuvres, spinal cord ischemia, segmental arteries damage, site and number of vertebral resection, selection of surgical procedures and so on.
14. PVCR enables correction of severe, rigid kyphoscoliosis through a space created by complete resection of vertebral segments, and the spinal cord tension is often increased following corrective procedures, which can be reduced effectively by repeated spinal shortening so as to maintain the cord in a moderately lower tension status. Using PVCR helps in protecting the spinal cord by performing correction and maintaining the cord in a moderately lower tension (strength of recommendation 8.14 ± 0.65).
In the process of surgical correction by spinal osteotomy, the key of spinal neurological protection is to control the translation of resected spinal ends and to maintain the cord in a moderate lower tension status. During PVCR, the deformity was decreased following the correction, especially for severe, rigid kyphoscoliosis cases, translation and/or compression of the resected ends would happen and threaten the safety of spinal cord by increasing its tension. In PVCR, through resecting vertebral segment totally, an artificial space for correction is created and the tension of the cord can be controlled initiatively; never try to close the space and always maintain it in order to reserve enough buffer space for spinal cord displacement following correction, which increases the reliance and safety of the spinal cord. The ‘high’ tension of spinal cord is a relative concept, and it is difficult to measure it by a tool or some objective index. Thus, the tension of spinal cord/dural sac can be evaluated by real-time and repeated palpation and inspection during PVCR procedure.
15. The spinal cord serves as the suppositional pivot during PVCR, which can much better control the abnormal translation between resection ends and decreases the risks to spinal cord (strength of recommendation 7.15 ± 2.77).
The aim of pivot in spinal osteotomy is to emphasize that the corrective force exerting process should always centralize that point. In PSO correction, the anterior cortical substance of vertebrae serves as the pivot. But in PVCR, the spinal cord acts as a suppositional pivot, and the procedure is to the detriment of the spinal cord displacement, involving angulation, rotation and so on. Based on that, the main advantage is that the change of spinal cord tension can be regulated timely and effectively. The differences of corrective pivot determine the differences of corrective manoeuvres and even determined the difficulties of surgical procedure and the risks to spinal cord.
16. The translation of resection ends is a main problem during PVCR correction. For kyphoscoliosis, this translation will occur easily in any 3D direction. In the process of correction, accurate pre-judgement and effective control of spinal translation will help to prevent spinal neurological injury (strength of recommendation 8.47 ± 0.84).
The translation of resection ends in PVCR could result not only from complete loss of spinal stability but also from improper application of corrective force, which would cause pivot displacement. Using one-dimensional corrective forces to correct a 3D deformity, the problem to be faced is translation of resection ends, which is an important risk factor in PVCR correction. It is recommended that a temporary rod should be used before complete loss of spinal stability following vertebral resection. In the corrective process, the direction of spinal translation should be pre-determined and controlled effectively for neurological protection. The spinal translation could not always be avoided, but on the basis of maintaining corrective space and keeping low tension of spinal cord, the acceptable angulation of spinal cord on coronal/sagittal plane is less than 20° and no more than 30° in rotation.
17. In order to protect the spinal cord, the temporary rod should be considered and utilized actively; and the main corrective process should be based on the in situ rod bending and rod exchange techniques so as to increase the safety of correction following vertebral resection (strength of recommendation 8.32 ± 1.38).
In the process of using PVCR to correct kyphoscoliosis, it is difficult to control the resected ends translation by the cantilever or transverse translation techniques and so on. But the in situ rod bending and rod exchange techniques are always performed around the spinal cord – ‘a suppositional pivot’, which effectively prevents the translation of resected ends from pivot displacement. Therefore, in PVCR correction, it is recommended to use the in situ rod bending and rod exchange techniques as the main corrective manoeuvre.
Because the processes of repeated in situ rod bending and/or rods exchange will decrease the mechanical strength of the rod, the terminal fixation should be changed into unused rods.
18. For some cases with most severe, rigid spinal deformity, preoperative traction would not only decrease degree of curvature and related difficulties of operation, but also could be helpful to evaluate the status of the spinal cord, which is significant for the pre-judgement of the potential tolerance of spinal cord to tensional changes in corrective process (strength of recommendation 7.05 ± 2.84).
Modern imaging techniques only reflect preoperative structural abnormality of the spinal canal and spinal cord. They do not cover the prediction and assessment of compliance of the spinal cord to tension during surgical correction. When severe, rigid spinal deformity with or without intraspinal malformations, the spinal cord is exposed to high tension and is close to decompensation. Surgical correction would push the spine and threaten the cord. On the contrary, preoperative traction increases spinal cord tension slowly and steadily so surgeons can assess the cord function and potential compliance to tension in a safe and effective way.
19. The ligation of increased number of segmental vessels will raise the risk to spinal cord (strength of recommendation 8.37 ± 1.12).
The segmental vessel is an important blood supply of the spinal cord. Ligation of the segmental vessel is also an important and effective measure, but could decrease the blood supply of the spinal cord and cause a neurological deficit. In PVCR, following the ligation of an increasing number of segmental vessels, the risks to the spinal cord will increase. Thus the segmental vessels should be ligated carefully.
Part 4: Spinal cord crisis (crucial status of neurological injury) related to PVCR procedures for severe, rigid spinal deformity correction – Monitoring and responses
Background
Although the gradual technical advances on spinal deformity surgery lead to improved correction rate and widely indicated cases, literature review based on a large number of case studies showed there has been a similar occurrence rate of neurological deficits related to spinal deformity correction procedures between the present and several decades ago. 23 In addition to the wake-up test, intraoperative neuromonitoring (IONM) has been advocated and widely adopted in patients undergoing spinal deformity surgery, for assessment of the spinal cord integrity with real-time feedback to allow for interventions if necessary, all with the goal of minimizing neurologic injury. Recently, multimodality monitoring, such as combined somatosensory evoked potential (SSEP), motor evoked potential (MEP) and electromyography, has been reported with high sensitivity and specificity (92.9% and 99.4%) on early detection of neurological deterioration. 24,25 Despite the success reported in the literature, there have been multiple anecdotal accounts of apparent false positive alerts, 26 which may compel surgeons to take unreasonable risks or unnecessarily change the operative plan, with increased surgical time. Moreover, several reports mentioned the false negative alerts of IONM during surgery of severe spinal deformity.
According to the guidelines for assessment and management of neurologic injury in the surgical treatment of idiopathic scoliosis, 27 corresponding strategies triggered by IONM alerts include: (1) reassessment of neuromonitoring signal strength, (2) increase spinal cord perfusion, (3) considering the Stagnara wake-up test, (4) critically examine pedicle screw position and remove malposition implant, (5) correction relaxed and releasing the tension on the spine, (6) assess canal for fragments of bone, gel foam or bone wax, which may cause cord compression, (7) decompression of epidural hematoma and (8) steroid protocol. Although relatively uncommon, delayed postoperative spinal cord injury may be attributed to progressive spinal cord ischemia secondary to traction or to the development of an epidural hematoma. The patient must be observed closely after operation.
There was a high incidence of IONM alert during PVCR procedure for the treatment of severe, rigid spinal deformity, due to the ‘sick or at high risk’ spinal cord accompanying severe deformity, the great amount of blood loss during operation, aggressive manoeuvres such as vertebral resection (destroyed stability of spinal column) and deformity correction (spinal cord tension change, and excessive displacement of spinal column or spinal subluxation). It is necessary to set up a series of strategies for the proper response to spinal cord crisis related to PVCR procedures for severe, rigid spinal deformity correction.
Consensus
20. Electrophysiological neuromonitoring has contributed to warn surgeons about potential neurological deficit during PVCR procedure for severe spinal deformity correction. However, considering the diagnostic test characteristics, IONM is not the only indicator for identification of spinal cord crisis. In case of an absent or abnormal signal, the wake-up test is recommended (strength of recommendations 8.81 ± 0.40).
Multimodality monitoring, including combined SSEP, MEP, and the wake-up test, is highly recommended for severe spinal deformity patients undergoing correction procedures. Surgeons always have to be aware of the possibility of false positive or false negative rate in IONM. Besides, conventional surgical manoeuvres during the PVCR procedure may give rise to a temporary disturbance of the spinal cord but in a functional tolerable range, and transient IONM signal changes should be detected. Wake-up tests are recommended in cases of absent or abnormal IONM signal. Frequent wake-up tests need the collaboration between the surgeon and the anaesthesiologist, and they are recommended to be performed after instrumentation is placed and finish of correction. Although relatively uncommon, delayed postoperative spinal cord injury can’t be ignored. It is important to have a monitoring protocol where clinical constant observations are made of motor and sensory functions at least for the first 24-h postoperative.
21. There is a significant high risk of spinal cord crisis during PVCR procedure for severe, rigid deformity correction (strength of recommendations 8.81 ± 0.40).
Once IONM data met the warning criteria and lasted for some period of time, a spinal cord crisis was indicated. For patients with severe, rigid deformity undergoing PVCR procedure, spinal cord crisis or injury would occur during the process of exposure and pedicle screw insertion, the process of vertebral column resection and the process of correction. The IONM signals must be continuously monitored throughout the PVCR procedure, especially during deformity correction, which is associated with most frequently causative factors such as spinal column instability, excessive displacement or spinal subluxation, mechanical impingement, change in spinal cord tension or hypoperfusion of the cord.
22. For patients with severe, rigid deformity and undergoing PVCR procedure, proper responding strategies to IONM alerts can reduce the rate of postoperative neurologic deficits, especially permanent spinal cord injury (strength of recommendations 8.31 ± 0.63).
The key elements for intraoperative responding to spinal cord crisis are prompt identification and appropriate treatment. Prompt indicates that early identification may increase the possibility of neurologic improvement. It is necessary to evaluate IONM technical and anaesthetic variables and to correct hemodynamic and oxygenation status. Reassessing IONM signals helps to exclude the temporary tolerable disturbance of the spinal cord, which was caused by previous corrective manoeuvres. Besides, the wake-up test should be performed when a false negative rate was suspected. The appropriate responding steps are beneficial to improve neurologic function, including adjustment of physical status, increase spinal cord perfusion, steroid drug as methylprednisolone and surgical manoeuvres.
IONM triggered corresponding surgical manoeuvres: (a) eliminate or remove fragments which cause spinal cord impingement, (b) reversed in situ rod bending and segmental de-rotation based on pedicle instrumentation, to decrease the opposite displacement between two aspects of resected area, (c) adjustment of extreme spinal cord tension which may be too high or too low, by compression or distraction force via instrumentation and (d) widening laminectomy and additional adjacent vertebral resection if necessary. Enlarged correction space may reduce the abrupt turning tendency of the spinal cord, and relieve the pressure from the canal edge, to decrease the rate of new or worsening neurologic event. 28,29
Part 5: Characteristics and therapeutic outcome of pulmonary function in patients with severe, rigid spinal deformity and respiratory dysfunction
Background
Severe, rigid spinal deformity is often associated with respiratory impairment. In addition to correction of the deformity, improving lung function is also one of the important goals of therapy. Preoperative lung function is influenced by a series of factors such as age, major curve size, apex location, complexity of deformity and so on. Moreover, therapy strategy, surgical options and recovery tendency of post-op lung function are also affected by those factors. Severe, rigid spinal deformity has significant impacts on lung function. Poorer lung function is a life-threatening factor, which is a great and inevitable challenge in caring for patients with severe, rigid spinal deformity. Accurate preoperative assessment of lung function is conductive to the evaluation of tolerance to correction operation, the choice of proper treatment opportunity, the sufficient preparation before operation, as well as the development of appropriate surgical plan.
Consensus
23. Patients with severe, rigid spinal deformity have poor lung functions manifesting as severe or profound severe restrictive ventilatory impairment. Type I respiratory failure and malnutrition can often be found in these patients (strength of recommendations 8.22 ± 1.00).
Spinal deformity is often associated with restrictive ventilatory impairment, and decrease of pulmonary function parameters is significantly correlated with severity of deformity. Lung function is exacerbated with the increase of the Cobb angle. Patients with a Cobb angle ≥90° have poorer lung function in comparison to those with a Cobb angle <90°. 30 Severe spinal deformity can exacerbate pulmonary dysfunction or respiratory failure. Respiratory failure included type I (arterial oxygen pressure <8 kPa) and type II (arterial oxygen pressure <8 kPa combined with arterial carbon dioxide pressure >6.65 kPa). Exertional dyspnoea can be found in patients with a Cobb angle >100°, and chronic respiratory failure can be found in patients with a Cobb angle >120°. 31
24. Admission assessment of lung function ought to be taken as a basis for comparison when planning treatment of PVCR in patients with severe, rigid spinal deformity. Type I respiratory failure is relative contraindication of PVCR procedure, and type II respiratory failure is absolute contraindication of PVCR procedure. Permanent existing respiratory failure after respiratory functional exercises and preoperative traction should be taken as absolute operation contraindication (strength of recommendations 8.00 ± 1.33).
In patients with severe, rigid spinal deformity, a preoperative forced vital capacity (VC) value lower than 40% prediction or 25 ml/kg increases the possibility of delayed extubation. 31 Respiratory failure can be found in 75% patients with profound restrictive ventilatory impairment (VC < 20%) preoperatively. Improvement of lung function can be achieved after respiratory training in those patients, helping dispose of the traditional idea that those patients were a contradiction of corrective operation, especially for PVCR.
25. Preoperative traction has positive effect on improvement of lung function in patients with severe, rigid spinal deformity. In addition to preoperative traction, measures to improve lung function include: (a) pulmonary function exercise (blowing balloons, respiratory gym, coughing and physical activity), (b) non-invasive ventilator and (c) nutritional support (enteral and parenteral; strength of recommendations 8.00 ± 1.30).
Pulmonary respiratory rehabilitation training can strengthen respiratory muscles, increase respiration efficiency, increase the alveolar ventilation volume, alleviate the airway collapse, facilitate alveolar gas discharge and improve ventilation function and blood oxygen exchange. Non-invasive ventilator used preoperatively that can improve alveolar hypoventilation and hypoxemia, correct respiratory and metabolic acidosis and increase the exercise tolerance of patients with spinal deformity. 32 For patients with severe, rigid and angular spinal deformity, not only would the preoperative traction be able to reduce spinal cord risk, it would also help to ensure life security by increasing respiratory function and operation tolerance.
26. Following PVCR, characteristics of changes for lung function in patients with severe, rigid spinal deformity and preoperative respiratory dysfunction include: respiratory recovery in adolescents is better than that in adults; it would take about 2 years to restore lung function up to or exceeding preoperative level (strength of recommendations 7.50 ± 2.15).
Not only can PVCR effectively correct spinal deformities, it can also improve lung function in patients with severe, rigid spinal deformity and preoperative respiratory dysfunction. The best outcome of lung function can be achieved if PVCR was carried out in patient with age of 12–18. The results of 2-year follow-up suggested the significant improvement of lung function in patients with different ages, and the results of 5-year follow-up suggested a further improvement. 33 –35
Part 6: The management of bleeding during PVCR in treating severe, rigid spinal deformity
Background
The massive blood loss in spinal correction surgery is one of the main problems. 3 In PVCR, which has a prolonged operative time, large wound and extremely complex technique, the potential traumatic coagulopathy is the greatest challenge for the spinal surgeon. Massive blood loss, massive blood transfusion and the traumatic coagulopathy can increase the complication rate significantly. The surgical team, including the surgeon and the anaesthesiologist, should fully understand this feature of the PVCR and understand in depth the traumatic coagulopathy and hyperfibrinolysis, lack of coagulation factor, hypothermia and acidosis during surgery. Based on this, the surgical team should actively apply multiple methods and techniques to respond to the traumatic coagulopathy and decrease the blood loss and blood transfusion in PVCR.
Consensus
27. PVCR is associated with prolonged operative time, a huge wound and extremely complex technique, and the blood loss is significantly more than other spinal correction technique. The massive blood loss and blood transfusion have been the most important factors that threaten the life of the patient during operation (strength of recommendations 8.59 ± 0.51).
PVCR can be associated with more than 10-h operative time, long fusion levels from the upper thoracic to lower lumber and resection of the vertebral body. Blood loss of twice the amount of adult human blood volume, which mainly comes from the huge wound, epidural veins and arteries and osseous wound, can be expected, and massive blood transfusion is needed during a PVCR procedure.
1
Massive blood loss and blood transfusion can increase the complication rate and medical costs. 28. Without active measures, massive blood loss and blood transfusion will inevitably cause traumatic coagulopathy in the PVCR patient. The traumatic coagulopathy included coagulation disorders, hyperfibrinolysis, lack of coagulation factor, hypothermia and acidosis will seriously threaten the safety of the patient in PVCR (strength of recommendations 8.31 ± 0.87).
Traumatic coagulopathy is a clinical syndrome that is caused by severe trauma and major surgery; it mainly represents a coagulation disorder. The huge wound is the pathological basis of traumatic coagulopathy in PVCR. Hyperfibrinolysis stems from a huge wound and endothelium injury, a lack of coagulation factor stems from massive blood loss and resuscitation therapy, hypothermia and acidosis; 36 all of the above factors improve the formation and development of the traumatic coagulopathy and even become part of the vicious cycle. If the surgeon does not actively take measures to deal with those risk factors, the traumatic coagulopathy will be destined to occur and develop, and it will increase the complication rate and threaten the safety of the PVCR.
29. The surgeon should actively take measures to prevent and control the formation and development of the traumatic coagulopathy, and thereby avoid the vicious cycle of coagulation disorders. The thromboelastograph is a powerful monitoring method for coagulopathy in PVCR. Thus, the surgeon can increase the safety of operation and decrease the complication rate (strength of recommendations 8.56 ± 0.62).
The thromboelastograph can help the surgeon to efficiently diagnose the coagulopathy in PVCR. Active antifibrinolytic therapy, supplementing coagulation factors in the early period, maintaining temperature and acidosis correction are effective responses to traumatic coagulopathy and coagulation disorders. It is necessary for the surgeon to use many methods and techniques to deal with traumatic coagulopathy during the whole procedure, and ensure the safety of the PVCR and decrease the complication rate.
30. The massive blood loss in PVCR stems from (a) huge wound, (b) epidural veins and arteries and (c) osseous wound: resection vertebra and bone graft bed (strength of recommendations 8.47 ± 0.80).
Blood oozing from the wound is the main reason for bleeding in the early period of PVCR. When starting vertebra resection, the blood loose mainly stems from the epidural veins and arteries and the resection vertebra, and massive blood loss in a short time is the feature in this period. Blood oozing from the bone graft bed is one of the bleeding sources in the later period of operation. With the PVCR going, the trauma and blood loss increase gradually and the traumatic coagulopathy will occur and develop. The blood loss increases significantly with the operation time extending; the coagulation disorders result from traumatic coagulopathy are particularly in the later period of PVCR. At this point, the blood oozing from the wound is the main bleeding reason, and the massive blood loss has been the inevitable result of the traumatic coagulopathy.
31. For now, antifibrinolytic drug such as tranexamic acid (TXA) used in PVCR can deal effectively with the traumatic coagulopathy and hyperfibrinolysis, so it can reduce the blood loss and blood transfusion safely and effectively (strength of recommendations 8.22 ± 1.06).
Traumatic coagulopathy and hyperfibrinolysis play an important role in the bleeding of PVCR, thus active antifibrinolytic therapy is the key point to reduce the blood loss and blood transfusion. Many attempts have been made using different antifibrinolytics to reduce operation bleeding since 1990, TXA has attracted more and more attention after the aprotinin was banned. TXA is a synthetic antifibrinolytic amino acid derivative that forms a reversible complex with both plasminogen and plasmin by binding at lysine binding sites. This binding completely blocks the interaction of plasminogen and plasmin with lysine residues on the surface of fibrin, thereby preventing proteolytic action of plasmin on fibrin and inhibiting fibrinolysis at the surgical wound. In spine surgery, TXA has become a widespread used and effective antifibrinolytic drug while the safety has been widely recognized. 37
32. Proper dosage of TXA is one of the key points to reduce the blood loss and blood transfusion safely and effectively in PVCR. Based on the existing studies, high-dose TXA is an alternative regimen for those surgeries that have long operating time, huge wound and great trauma (strength of recommendations 7.94 ± 1.56).
The safety and effectiveness of TXA used in spine surgery has been widely recognized. 37 Many dose regimens of TXA have been used to control bleeding in spine surgery, and the study results varied when low-dose TXA was applied into spine surgery, but studies indicated that the high-dose TXA can reduce bleeding in spine surgery significantly. 38 A recent randomized controlled trial has proved that high-dose TXA can reduce much more blood loss and blood transfusion than low-dose TXA without increasing complications. 39 In a study of PVCR, high-dose TXA has been proved that can reduce blood loss and blood transfusions significantly. 40
33. Maintaining temperature and correction of acidosis are effective methods to control bleeding in PVCR (strength of recommendations 8.35 ± 0.79).
Severe hypothermia and acidosis can affect the function of the platelet and coagulation factors and can promote fibrinolytic activity. Hypothermia, acidosis and coagulation disorders form the ‘Triangle of Death’, thus maintaining temperature and acidosis correction are one of the most important measures to prevent and control the traumatic coagulopathy and bleeding in PVCR. 41
34. Active supplement of coagulation factors in the early period of PVCR can reduce blood loss and avoid the vicious cycle of coagulation disorders (strength of recommendations 8.31 ± 1.30).
In the early period of PVCR, the active supplement of coagulation factors which is consumed, lost or diluted during surgery, such as fresh frozen plasma, cryoprecipitate, fibrinogen and so on, is a very important measure to restore the coagulation function and deal with the traumatic coagulopathy.
35. Appropriate intraoperative haemostasis skill, especially the adept intraspinal canal haemostasis skill can help surgeons control the blood oozing from the epidural veins and arteries (strength of recommendations 8.56 ± 0.62).
Blood oozing from the epidural veins and arteries is the main bleeding source in the vertebra resection period in PVCR, and massive blood loss in a short time is a feature in this period. However, epidural venous plexus pressure is independent of arterial blood pressure, and the drugs have a limited effect on it. Adept intraspinal canal haemostasis skill is the main means to control blood oozing from the epidural veins and arteries and also the important part of controlling bleeding for PVCR.
36. The long period of controlled hypotension in PVCR can jeopardize perfusion to important organs, and controlled hypotension has a limited effect on the bleeding from intraspinal canal and osseous wound with increasing complications (strength of recommendations 8.11 ± 1.02).
Controlled hypotension has been used in spine surgery for decades; it can reduce blood oozing from the wound effectively. However, epidural venous plexus pressure and intraosseous pressure are independent of arterial blood pressure, and controlled hypotension cannot reduce the bleeding from intraspinal canal and osseous wound significantly. Long periods of controlled hypotension in PVCR can jeopardize perfusion to important organs such as brain and spinal cord, and controlled hypotension is a risk factor for loss of vision after spine surgery. 42 Hence, we do not recommend using long-time controlled hypotension in PVCR.
Part 7: The relationship of pedicle screw insertion and spinal cord safety during PVCR in the treatment of severe and rigid spinal deformity
Background
Correction of severe, rigid spinal deformity creates further potential risk to the spinal cord and nerve root. Pedicle screw malposition was the most commonly identified iatrogenic problem, responsible for 30.3% of all IONM true-positive events. In investigating the reason, abnormal pedicle was an important factor. Most studies focused on the morphology of the pedicles. In the patients with adolescent idiopathic scoliosis, a total of 22.5% of pedicles were abnormal morphologically, 94.7% of which were located in the region of T2-T10. A total of 31.9% of the thoracic pedicles and 2.4% of the lumbar pedicles were abnormal pedicles. As to the distribution, about 10.0 and 2.9% of the abnormal pedicles were located on the concavity and convexity, within the periapical region. A Cobb angle of >70° was associated with increased abnormal pedicle. In recent years, some researches revealed that the cortical width of thoracic pedicles was the sole factor crucial for predicting the accuracy of thoracic pedicle screw placement. Three times as many pedicle screws were misplaced in abnormal pedicles compared with normal pedicles. Whether more screws can be inserted into morphologically abnormal pedicles safely is crucial during PVCR to maintain the stability of the spine, implement the corrective methods, obtain good correction and obtain solid fusion. Thus, the preoperative reliable observation and analysis of each pedicle will be very important.
Consensus
37. There is high incidence of abnormal pedicle in severe, rigid spinal deformity. Screw malposition is one of the reasons leading to iatrogenic spinal cord injury during PVCR (strength of recommendations 8.65 ± 0.49).
Over the last decades, most studies focused on the morphology of the pedicles, which gives little help to surgeons for predicting the accuracy and guiding the procedure of pedicle screw placement. The main factor of screw malposition during PVCR in the treatment of severe, rigid spinal deformity was the pedicles with small extremities or in the absence of a medullary cavity. However, even among skilled spinal deformity surgeons, new neurologic deficits are inherent potential complications of spine surgery. Screw malposition makes up a high proportion of the new neurologic deficits. 43
38. When PVCR is performed to correct the severe, rigid spinal deformity, the most crucial step is to insert sufficient screws in the pedicles, particularly pedicles in the region near the column to be resected (strength of recommendations 8.50 ± 0.73).
In these patients, sufficient screw insertion in the levels adjacent to the resection area, junctional area and terminal fixation segments is the precondition to obtain efficient deformity correction. For patients with severe, rigid spinal deformity, PVCR will be the best alternative. More safe screw insertion, particularly around the region of vertebral column resection, is crucial to control the subluxation of the spinal limb, implement the corrective methods, restoration of anterior column, get solid fusion and reduce the loss of correction and instrument breakage. 4
39. Insufficient screws inserted into the pedicle of the cranial and caudal vertebras adjacent to the resected column is a relative contraindication to the administration of PVCR to treat severe, rigid spinal deformity (strength of recommendations 8.56 ± 0.51).
During the PVCR, all the processes including (a) placement of the temporary stabilizing rod to avoid the sudden displacement of the spinal cord before losing the stability of the spine, (b) exchanging rods to correct the deformity, (c) proper and timely shortening of the spinal cord and (d) control the subluxation of the spinal limb are based on sufficient pedicle screws adjacent to the resection area.
40. It is necessary to evaluate the diameter, morphology and rotation of the pedicle by computer tomography preoperatively. The inner cortical width of thoracic pedicles is the sole factor crucial for accurate placement of thoracic pedicle screws. The outer cortical width of thoracic pedicles is a factor for the diameter of screw. An extremely small pedicle is the risk of complications related to pedicle screws (strength of recommendations 8.75 ± 0.45).
For surgeons, especially in the procedures of applying PVCR, the preoperative reliable observation and analysis of each pedicle will be very helpful for the accurate insertion of screws and the final decision of fusion segments. Recommendation: CT evaluation is regarded as a more effective means. All thoracic pedicles to be instrumented should be scanned preoperatively using CT scan. The inner cortical width of thoracic pedicles should be measured horizontally at the narrowest point of each thoracic pedicle. When the thoracic pedicle has no channel or the inner cortical width is 0–1 mm, the accuracy of thoracic pedicle screw placement will be extremely low. The angulations of the spinal deformities in the coronal plane and the rotation of the vertebral body only indirectly affected the accuracy and safety of thoracic pedicle screw placement by increasing the difficulty of the surgeries. The only crucial factors that had a direct impact on the accuracy and safety of thoracic pedicle screw placement and safety were (a) whether the pedicle had a channel and (b) the inner cortical width of the thoracic pedicles. 44 –47
Part 8: Analysis and prevention strategy of major perioperative non-neurological complications in severe, rigid spinal deformity undergoing PVCR
Background
PVCR provides a larger amount of correction than PSO; however, the reported prevalence of complications in patients treated by PVCR ranges from 34.3% to 64.3% as well as major perioperative non-neurological complications ranges from 18.75% to 40.00%.8,19,20,48 The significant risk of potentially life-threatening non-neurological complications exists in severe, rigid spinal deformity because of weak health status, poor organ function reservation, complex surgical procedure, longer operating time and excessive bleeding. The non-neurological complications involve multiple systems, multiple organs and all perioperative issues and seriously affect the patient’s life. Therefore, we should not only focus on the safety of the spinal cord but also need to take a variety of preventive measures to decrease the non-neurological complications.
Consensus
41. Severe, rigid spinal deformity undergoing PVCR is classically associated with a high rate of non-neurological complications which are seriously affecting the patient’s life. So, we should pay more attention to non-neurological complications (strength of recommendations 8.63 ± 0.50).
The non-neurological complications undergoing PVCR include (a) respiratory system-related complications: pneumonia, pleural effusion, pulmonary embolism, pleural injury, hemopneumothorax and respiratory failure; (b) wound infection: superficial infection and deep infection; (c) excessive bleeding and combine with traumatic coagulopathy; (d) cardiovascular complications: cardiac arrest, heart failure, arrhythmia, hypotension and myocardial infarction; (e) implants failure: rod fracture, pedicle screws loosening and fracture; (f) digestive system complications: intestinal obstruction and superior mesenteric artery syndrome; (g) intraspinal hematoma; (h) deep vein thrombosis; (i) dural tear and cerebrospinal fluid leak; and (j) optic deficit, high fever, death and so on. The non-neurological complications involve all perioperative issues and seriously affect the patient’s life.
42. The major reasons for non-neurological complications undergoing PVCR consist of poor preoperative cardiopulmonary function and reserves, poor nutritional status, longer operating time, excessive bleeding and serious trauma (strength of recommendations 8.63 ± 0.50).
In the patient with severe, rigid and angular spinal deformity, preoperative cardiopulmonary function and reserves, nutrition and physical activity have been significantly weakened. Serious impairment of pulmonary function badly impacts on pulmonary ventilation and oxygen exchange, and even results in respiratory failure and significantly increases the risk that the patient may not be able to be extubated and may mean a longer length of hospital stay. Malnourished status has negative influence on tissue repaired capacity and inflammatory cell response capacity and increases the risk of infection and bone graft non-fusion. 20,35 PVCR achieves outstanding correction for severe and rigid spinal deformity; at the same time, it also results in the abrupt displacement of thorax/lung/heart/great vessels and affect their normal function. From PVCR surgical procedure aspect, the complexity and extraordinary technique is associated with extensive operative exposure, long operation time, excessive bleeding and serious trauma. It has great influence on homeostasis and cardiopulmonary function. The characteristics of patient undergoing PVCR and surgical procedure are responsible for the high risk of non-neurological complications.
43. Taking a variety of preventive measures to decrease risks of non-neurological complications of PVCR (strength of recommendations 8.63 ± 0.50).
The following practices are recommended to decrease postoperative non-neurological complications with PVCR: (a) perioperative pulmonary function exercise and nutrition support; (b) using preoperative cardiac ultrasonic, dynamic electrocardiogram to screen potential cardiovascular disease; (c) applying preoperative halo-femoral traction to improve scoliosis and kyphosis and decrease technical difficulties of surgical processes; (d) using a variety of surgical techniques and haemostatic drugs to decrease intraoperative bleeding; (e) using autogenous bone graft or titanium mesh structural bone graft to reconstruct the anterior column, increasing bone graft area and density and using thick rod and cobalt chromium rods are beneficial to reduce the risk of implants failure 49 ; (f) actively systemic supportive treatment; and (g) due to disastrous postoperative deep wound infection, it is necessary to actively use antibiotics to prevent infection.
Part 9: Summary
Based on the above descriptions and comprehension concerning PVCR, and based on the agreement with expert team, we insisted that it was very necessary to give a general overview of the procedure of PVCR.
44. The essential properties regarding PVCR procedure are tightly linked with various factors such as medical and surgical indication, range and level of vertebral column resection, strategies of correction, corrective efficiency and control of neurological risk.
During PVCR, one or more vertebrae with adjacent discs are resected completely. The spinal column is divided into two free motion segments and connected only by the spinal cord; thus the integrity and stability of the spinal column are destroyed, with the purpose for achieving enough corrective space and 360° circumferential decompressions of the spinal cord. The corrective space is available for 3D correction of severe rigid deformity through spinal column shortening and reducing the spinal cord tension. The corrective space is available for improving the compliance of the spinal cord, whereas the excessive opposite displacement or subluxation of spinal column occurred during the PVCR procedure. Furthermore, the corrective space is also available for reliable and effective reconstruction on the anterior-middle column after deformity correction. PVCR is different than other reported osteotomy techniques, and the range and shape of the corrective space achieved by PVCR are mainly related to the severity of spinal deformity. PVCR belongs to a kind of high-efficiency, powerful and high-risk procedures for spinal deformity remodelling. PVCR is used mainly for severe, rigid spinal deformity that is not manageable by other osteotomy techniques.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.