
Abstract
Purpose:
The Pirani score is widely used in the treatment of idiopathic clubfoot. Some authors recommended to base decision for Achilles tenotomy in Ponseti method on this score (hindfoot score [HFS] > 1, once reducibility of lateral head of talus (LHT) is zero) instead of originally described indications (dorsiflexion < −10–15° once complete abduction is achieved). Yet correspondence of these indications has not been evaluated. Aim of this study was to verify whether in a cohort, where decision is based on dorsiflexion, the Pirani score corresponds to the limits suggested. Secondarily, to describe temporal variation in Pirani score along treatment, which has not been previously investigated.
Methods:
In a prospective study, 79 idiopathic clubfeet in 47 cases consecutively treated with Ponseti method by a single orthopaedic surgeon were evaluated at each casting session with Pirani system; score progression and scores at time of decision to perform tenotomy were determined.
Results:
HFS and its subcomponents showed minimal improvement during subsequent sessions of casting and then rapid correction with tenotomy. Medial crease resolved rapidly. Midfoot score and its remaining subcomponents corrected gradually. Total Pirani score showed initially a progressive correction and then a more abrupt improvement with tenotomy. At the time of decision to perform tenotomy, in 8 (10.1%) of 79 cases, the decision whether or not to perform tenotomy based on dorsiflexion would have been different based on the cut-offs for Pirani score suggested.
Conclusion:
Using Pirani score in guiding indication for tenotomy may imply different decisions in a portion of cases, which should be considered when comparing series.
Introduction
Numerous scoring systems have been proposed to rate idiopathic clubfoot at presentation. 1 The ideal features of any classification scoring system include reliability, feasibility in a clinical setting and ability to monitor correction, predict appropriate treatment, recurrence rate and long-term outcome. 1,2
The system proposed by Pirani et al., 3 now routinely used in most centres, is easily and quickly feasible in clinical setting without the need for technical equipment 4,5 and has been proven reliable. 2 –4,6 –8
The utility of this scoring system at the initial evaluation has been largely accepted. 5,9 Its ability in predicting the number of casts required for clubfoot correction and the need for tenotomy in the Ponseti method has been investigated with variable results. 1,5,10 –14 Initial Pirani score has been suggested to correlate with the risk of relapse, whereas its influence on the long-term outcome is still unclear. 15
In addition, it has been advocated that the Pirani score can assist throughout the treatment process, particularly in tracking treatment progress and in guiding the indication for Achilles tenotomy. 5,6,11,16 –20 Yet, these features have been poorly investigated.
The aim of this study was to describe the progression of correction along the Ponseti treatment using the Pirani scoring system and to analyse the Pirani score at the moment when the indication for Achilles tenotomy is evaluated.
Methods
We performed a retrospective analysis of prospectively collected data, investigating idiopathic congenital clubfeet consecutively treated from October 2013 to October 2015 with the Ponseti method by a single-trained orthopaedic surgeon, as a part of a prospective longitudinal study. 21 Postural deformities, age greater than 6 months at presentation and patients treated with an accelerated protocol, 22 were excluded from the study. Clubfeet categorized as non-idiopathic at presentation or at successive evaluations were not included.
All feet were treated by the same paediatric orthopaedic surgeon according to the method described by Ponseti. 23 Progressive correction of the deformity was achieved by means of weekly sessions of manipulations and casting (plaster of Paris long-leg cast) and finally the equinus was addressed. A percutaneous Achilles tenotomy was performed under general anaesthesia if the foot could not be dorsiflexed to 15° once complete abduction was achieved and a final cast was applied for 20 days. After removal of last cast, a foot abduction brace (Mitchell–Ponseti brace) was applied 23 h/day for 3 months and gradually reduced to naptime and night-time wear until 4–5 years of age. 21
For each clubfoot, evaluation of the Pirani score3 was performed by the same clinician before the first cast application and after cast removal at each successive visit. The Pirani scoring system takes into consideration six different components of clubfoot deformity: posterior crease (PC), emptiness of the heel (EH), rigidity of equinus (RE), medial crease (MC), curvature of the lateral border (CLB) of the foot and reducibility of the lateral part of the head of the talus (LHT). Each component is scored on a three-point scale (0 = No abnormality, 0.5 = Moderate abnormality and 1 = Severe abnormality): the sum constitutes a total on a six-point scale (total score, TS), where higher scores indicate a more severe deformity. TS is divided into two subtotal scores, representing midfoot (midfoot score [MFS]: summing up MC, CLB and LHT) and hindfoot contracture (hindfoot score [HFS]: summing up PC, EH and RE), each ranging from 0 to 3.
The clinician familiarized himself with the scoring system before the study was commenced. A score sheet with pictures and explanations was used to report the scores. Evaluations were not blinded with regard to previous sessions since details of previous examinations were usually available at the time of following evaluation.
Approval of the institutional review board was obtained. Families were informed that data would be submitted for publication and gave their consent.
The SPSS for Windows version 22 (IBM SPSS Inc., Chicago, Illinois, USA) was used for statistical analysis. Feet undergoing (tenotomy group) and not undergoing Achilles tenotomy (non-tenotomy group) were compared with regard to MFS, LHT and HFS at the time when the decision was made whether to perform tenotomy or not (thus before tenotomy for tenotomy group and before application of the foot abduction brace for non-tenotomy group). After evaluating normality of the data distribution and using Levene’s test for equality of variances, the student’s t test was used to analyse the differences in the scores between the two groups. A p-value < 0.05 was considered to be significant.
For each case, we calculated the number of casts required for correction and divided cases in groups according to the number of casts. For each group, mean scores of each component, subtotal score and TS at each visit were calculated and plotted on a graph.
Results
A total of 79 idiopathic clubfeet in 47 patients (37 male, 10 female, 15 unilateral, 32 bilateral) met the criteria and were analysed. Mean age at first cast was 30.6 days (range: 5–168 days). Mean Pirani score was 4.8 (range: 2–6). Mean number of casts was 4.4 (range: 2–7). Achilles tenotomy was performed in 84.8% of clubfeet treated (67 of 79 feet) at a mean age of 62 days (range: 47–191). Initial correction was achieved in all feet (mean Pirani score at last cast removal: 0.41 ± 0.47, range 0–1.5). Only minor complications (skin irritations) were experienced during the correction phase.
At the time of decision to perform tenotomy or not, MFS was lower than 1 in all feet, with a statistically significant difference (p = 0.004) between non-tenotomy group (mean MFS is 0.00) and tenotomy group (0.06 ± 0.16, range 0–0.5). LHT was 0 in 95% of feet (75 of 79), with a non-significant difference (p = 0.0.391) between non-tenotomy group (mean LHT is 0.00) and tenotomy group (0.03 ± 0.12, range 0–0.5).
HFS was significantly (p = 0.000) lower in non-tenotomy group (0.83 ± 0.39, range 0.5–1.5) than in tenotomy group (2.25 ± 0.69, range 0.5–3). Two (16.7%) of 12 feet in non-tenotomy group had HFS > 1 (at subsequent follow-up feet showed complete correction and TS 0). Six (9.0%) of 67 feet in tenotomy group had HFS ≤ 1.
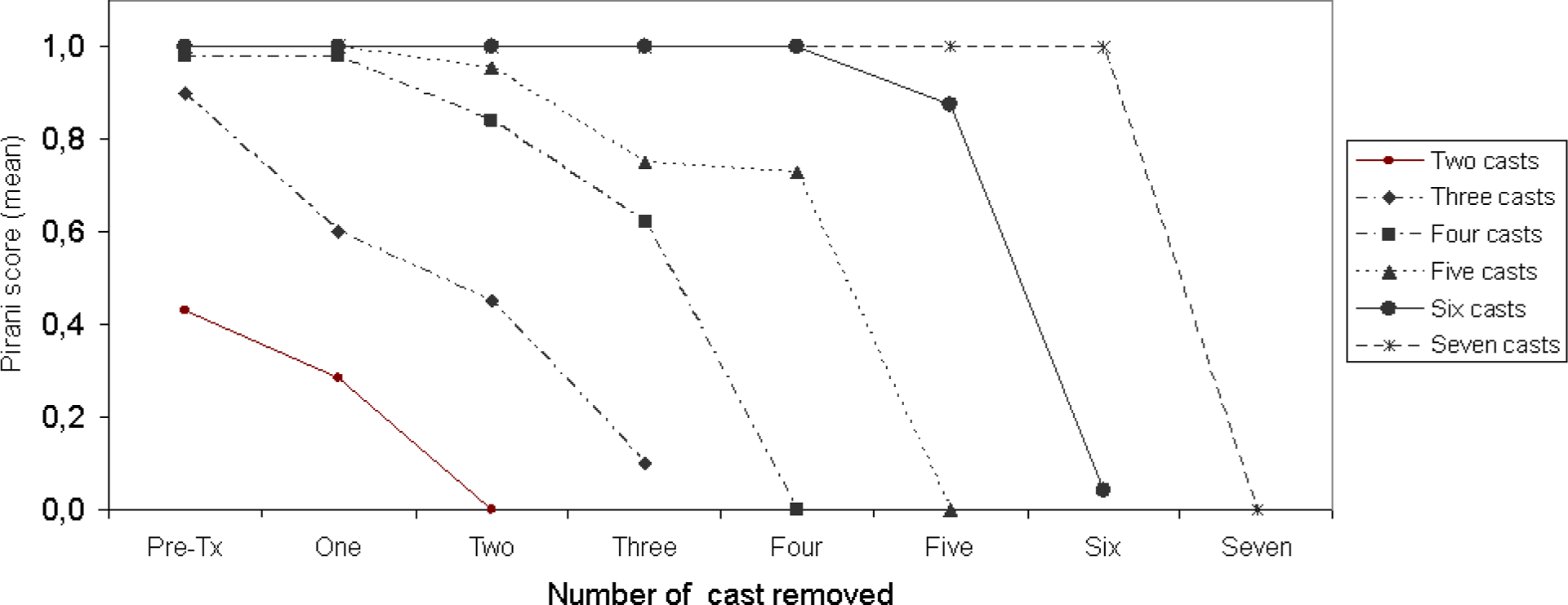
The number of casts required for correction was calculated, and cases were divided into groups: two-cast group included 7 feet, three-cast 10 feet, four-cast 25 feet, five-cast 22 feet, six-cast 12 feet and seven-cast 3 feet. Different patterns of correction were recorded by plotting respective scores on graphs.
PC usually disappeared after Achilles tenotomy or just a minor improvement was recorded earlier (Figure 1). EH showed no (or minimum) improvement throughout the casting sessions (Figure 2). A considerable improvement was recorded after Achilles tenotomy, but in 39 feet (of 79), final EH was > 0.

Progression of PC correction. PC: posterior crease.

Progression of empty heel parameter.
RE did not improve until discontinuation of the final cast in feet requiring more than five casts; in feet requiring less than six casts, a progressive improvement was recorded, but most of the correction was achieved after last cast removal (Figure 3).
Rigid equinus correction.
MC resolved rapidly and was completely corrected after the first one/two casts (Figure 4).

MC correction. MC: medial crease.
LHT and CLB corrected gradually throughout the course of treatment (Figures 5 and 6).

Correction of reducibility of LHT. LHT: lateral part of the head of the talus.

Correction of CLB of the foot. CLB: curvature of the lateral border.
As regards subtotal scores, HFS showed minimal improvement during subsequent sessions of casting, remaining ≥2.5 until last cast in most feet requiring tenotomy, and then showed rapid correction (Figure 7); MFS showed gradual improvement along the casting sessions (Figure 8).

HFS correction. HFS: hindfoot score.

MFS correction. MFS: midfoot score.
TS showed initially a progressive correction and then a more abrupt improvement of 2–3 points with the tenotomy (Figure 9).

TS progression. TS: total score.
As regards progression of TS in every single foot, the score improved in comparison with previous casting in 81.6% (283) of 347 sessions, was unchanged in 18.4% (64/347) and never increased; among these, in seven circumstances, the score remained unchanged for two consecutive sessions and in one circumstance for three sessions.
Discussion
The Ponseti method (including serial casting, percutaneous Achilles tenotomy and bracing) 23 currently represents the gold standard for clubfoot treatment and provides initial complete correction in most cases (reported correction rates of 89–98%). 9,24 –26
The two scoring systems that are most commonly used to track progression of correction with the Ponseti method are the Dimeglio score 27 and the Pirani score. 3 The utility of the former in tracking progression has been previously analysed. 21,28 With regard to Pirani score, its use is described by most authors not only for initial evaluation but also in the subsequent steps of correction. 6,12,16 –20 Yet its temporal progression and the one of its constitutive parameters has been poorly investigated. 16,18,19 Visual representation of the scores on a graph may represent a paradigm roadmap of treatment, thus supporting inexperienced practitioners for expected results following each cast. 28
We recorded typical patterns for each parameter. As regards hindfoot parameters, they tended to show only minor improvement with subsequent casts. Particularly, EH and PC improved for the most part at discontinuation of the final cast. RE showed a slight progressive improvement in feet requiring less than six casts, but generally most of the correction was achieved after Achilles tenotomy. This is intuitive, since equinus is supposed to be the last deformity to be corrected. 28 Yet it has been demonstrated in MRI studies 29 (and it is commonly experienced in applying casts) that correction of equinus occurs more gradually throughout the casting sessions as automatic result of correction of the midfoot variables. 28 This feature has been confirmed using the Dimeglio score, 21,28 which therefore seems to be more sensitive in monitoring equinus than the Pirani score.
As a result, HFS showed only slight improvement during subsequent sessions of casting and abrupt correction after Achilles tenotomy.
MC was completely corrected after the first one/two casts. Persistence or appearance of MC over a certain number of casts should raise suspicion on the right progression of correction.
The only parameters showing gradual improvement that followed the clinical correction provided by the Ponseti method were LHT, CLB and consequently MFS, with the latter reaching zero in almost all cases.
TS documented an improvement in 81.6% of the sessions, and progression was gradual throughout the treatment (mostly due to MFS) with a more abrupt improvement of 2–3 points with the tenotomy (due to HFS).
At last cast removal, TS frequently resulted above zero, despite correction could be considered complete, as reported by other authors. 1,11,30,31 This was mostly due to persistence of EH above zero (49.4% of feet). The incidence of persistence of this feature has been poorly investigated (only Adegbehingbe et al. 30 described rate in their experience: 22% of cases) and longer follow-up will be needed to verify if this implies higher risk of recurrence. Yet it is commonly experienced and it has been shown 30 that empty heel pad has a tendency to remodel over time to a normal shape; its persistence at the end of treatment should not be considered an indication for further procedures 30 and correction is considered complete even with an empty heel above zero at the point of fitting into the abduction brace. 31
In order to analyse the utility of Pirani scoring system in guiding the indication for Achilles tenotomy, we looked for Pirani-related indications for tenotomy in the literature. In online manuals of Ponseti method, 18,19 it is stated that tenotomy would be indicated when HFS is higher than 1, MFS is lower than 1 and LHT is zero. Yet even papers describing the use of Pirani score in the evaluation of clubfoot usually do not base the indication on this score but mainly on originally proposed limits of dorsiflexion higher than −10/−15° with complete abduction, 11 –13,15,22,32 which is our behaviour as well. We performed a posteriori an analysis to verify whether the above-mentioned Pirani-based indications corresponded to the original guidelines. We found that in most of the cases, the indications corresponded. In particular, the limits of coverage of the head of the talus and MFS < 1 were almost always respected (these are prerequisites for correction both in tenotomy and in non-tenotomy group), and the HFS was significantly higher in the tenotomy (mean HFS 2.25 ± 0.69) than in the non-tenotomy group (mean 0.83 ± 0.39) with the limits of HFS > 1 respected in 89.9% of feet. Yet the limit of HFS could not be regarded as strict, since in a few feet, the tenotomy was not performed despite an HFS > 1 and other few feet underwent tenotomy despite an HFS ≤ 1. These data do not imply superiority of one system with respect to the other one (longer-term follow-up would be required), but show that, in a portion of cases, surgeons basing their indications on Pirani score may take different decisions in comparison with surgeons using dorsiflexion. For example, a foot with full correction of abduction, MFS = 0, dorsiflexion to 5°, RE = 0.5, EH = 0, PC = 0 and HFS = 0.5 does or does not undergo tenotomy according to the criterion used; this could explain part of the variability of tenotomy rate reported in the literature in different series.
Since the assessment of PC, 4 empty heel sign 4,8 and dorsiflexion 33 is not completely reliable, the use of a dorsiflexion lateral radiograph of the foot has been proposed to rule out cases with midfoot breakage and elevated calcaneus and more objectively determine the need for tenotomy. 33 This could be of value particularly in case of doubt (e.g. persistence of EH and PC in front of satisfying dorsiflexion).
The strength of our study is that all feet have been treated by a single trained orthopaedic surgeon with the same method and represent consecutive cases of a prospective study. Main weaknesses are that assessment and treatment were performed by the same person and that evaluations were usually not blinded with regard to previous evaluation; nevertheless, since Pirani score was recorded only for descriptive purposes and did not seem to have influenced treatment in this series, we feel that this bias was not significant. In addition, long-term follow-up will be needed to ascertain whether the initial correction obtained could be maintained; yet interest of the article was in the dynamics of correction and not in subsequent rate of recurrence, and initial correction was obtained in all cases.
In conclusion, our article described the progression of clubfoot correction using Ponseti method according to the Pirani score and showed that MFS tends to correct gradually, HFS improves only at the end of treatment and TS acts as a result of these two patterns. The use of the limits of Pirani score suggested in the literature instead of dorsiflexion in guiding indication for tenotomy may imply a different decision in a small number of cases, which should be considered when evaluating different series.
Footnotes
Author’s note
This study was conducted at the Department of Pediatric Orthopedics and Traumatology, Rizzoli Orthopaedic Institute, Bologna, Italy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
One of the authors (CN Abati) received a grant from CEDISS Security Engineering, a private donor without profit interest.