
Abstract
Purpose:
To determine the predictive value of the Pirani scoring system in the need for tenotomy using the Ponseti method for management of idiopathic clubfoot.
Method:
This is a prospective observational study involving patients less than 2 years of age with idiopathic clubfoot. The consenting parents and institution ethical board approved the study. The relationship between Pirani scores and the need for tenotomy was evaluated using the independent t-test and the binary logistic regression to predict the need for tenotomy. Pearson’s r and Cohen’s κ were used to measure correlation and agreement, respectively, between the predicted and observed values. A receiver operating characteristic curve was used to interpret sensitivity and specificity levels as well as to obtain a cutoff score for predicting the requirement for tenotomy.
Results:
Eighty-four clubfeet from 50 patients were studied. Thirty-eight feet (45%) had percutaneous tenotomy. The initial total Pirani and hindfoot scores were found to predict the need for tenotomy with the model for prediction being able to predict correctly in 72.6% and 75% of the time, respectively. A higher Pirani score was associated with higher odds of requiring tenotomy (OR = 4.402, p < 0.001) and total Pirani score above the cutoff point of 4.75 predicted the need for tenotomy.
Conclusion:
The indication for tenotomy appears to be well predicted using the Pirani scoring system with the odds of requiring a tenotomy increasing by more than fourfold for every unit increase in Pirani score.
Introduction
Various scoring systems have different abilities in predicting the clubfoot management outcome. The Ponseti treatment for clubfoot deformity was introduced in North America in the late 1940s, developed by Ignacio Ponseti. This has become a primary treatment option in many countries more recently. 1,2 The Ponseti method involves serial corrective manipulations, a specific technique of cast application and a possible percutaneous tendo-Achilles tenotomy. This method has been reported to have a success rate approaching 98%. 3
The Pirani scoring system, devised by Shafiq Pirani, consists of six parameters: three each in the hindfoot and the midfoot. The parameters areas follows: curvature of the lateral border of the foot, medial crease, uncovering of the lateral head of the talus, posterior crease, emptiness of the heel, and degree of dorsiflexion (DF). 4,5 Each category is scored as 0, 0.5, or 1. The least (best) total score for all categories combined is 0, and the maximum (worst) score is 6. The Pirani scoring system can be used to identify the severity of the clubfoot and to monitor the correction. There is sparse literature on the predictive value of Pirani scoring system for tenotomy in the management of idiopathic clubfoot, thus limiting the gains to be obtained from the scoring system.
In this study, we sought the correlation between the Pirani score at the time of diagnosis and the need for tenotomy in the Ponseti method of treating idiopathic clubfoot.
Methods
A prospective observational study was done, involving patients less than 2 years of age with idiopathic clubfoot at our hospital. The consenting parents and institution Ethical board approved the study protocol according to the University of Iowa Ponseti protocol. 6 Corrective serial casts were applied after carrying out proper manipulations according to the Ponseti method. 7 If dorsiflexion was not obtained up to 15° after achieving the abduction up to 70° and correction of the varus deformity, a simple percutaneus tenotomy of the Achilles tendon was performed. A long leg cast was applied in 70° of abduction and 15° of dorsiflexion immediately after tenotomy under the effect of local anesthesia for further 3 weeks to allow for healing of the tendon. Finally, the patient was given an abduction foot orthosis brace to be worn 23 h a day for 3 months. Thereafter, the brace is to be worn every night for 3 years. Patients were monitored for temperature, pulse, and respiratory rate till 1 h of postoperative period. The relationship between Pirani scores and the need for tenotomy was evaluated using the independent t-test with p ≤ 0.05 considered to be significant, and the binary logistic regression (BLR) used to predict the need for tenotomy. The age of the patients was categorized into three groups (≤26weeks, 27–52weeks, and >52weeks), for a more analytical assessment of this variable. Pearson’s r and Cohen’s κ were used to measure correlation and agreement, respectively, between the predicted and observed values. A receiver operating characteristic (ROC) curve was used to interpret sensitivity and specificity levels as well as to obtain a cutoff score for predicting the requirement for tenotomy.
Results
Eighty-four clubfeet from 50 patients were studied. Thirty-eight feet (45%) had percutaneous tenotomy. The patients were grouped into those with and without tenotomy, and the mean score of those who had tenotomy was higher than those who did not (t = 5.679, p < 0.001).
A higher Pirani score is associated with higher odds of requiring tenotomy as shown in Table 1 (OR = 4.402, p < 0.001). Also, compared to those who were older than 52 weeks, those who were 26 weeks and below were less likely to need tenotomy (OR = 0.244, p = 0.073); however, this relationship is not statistically significant. Sex and the side of foot affected are not significant predictors of the need for tenotomy. Mean number of cast applied was 5.1.
BLR to predicting need for tenotomy from TPS.
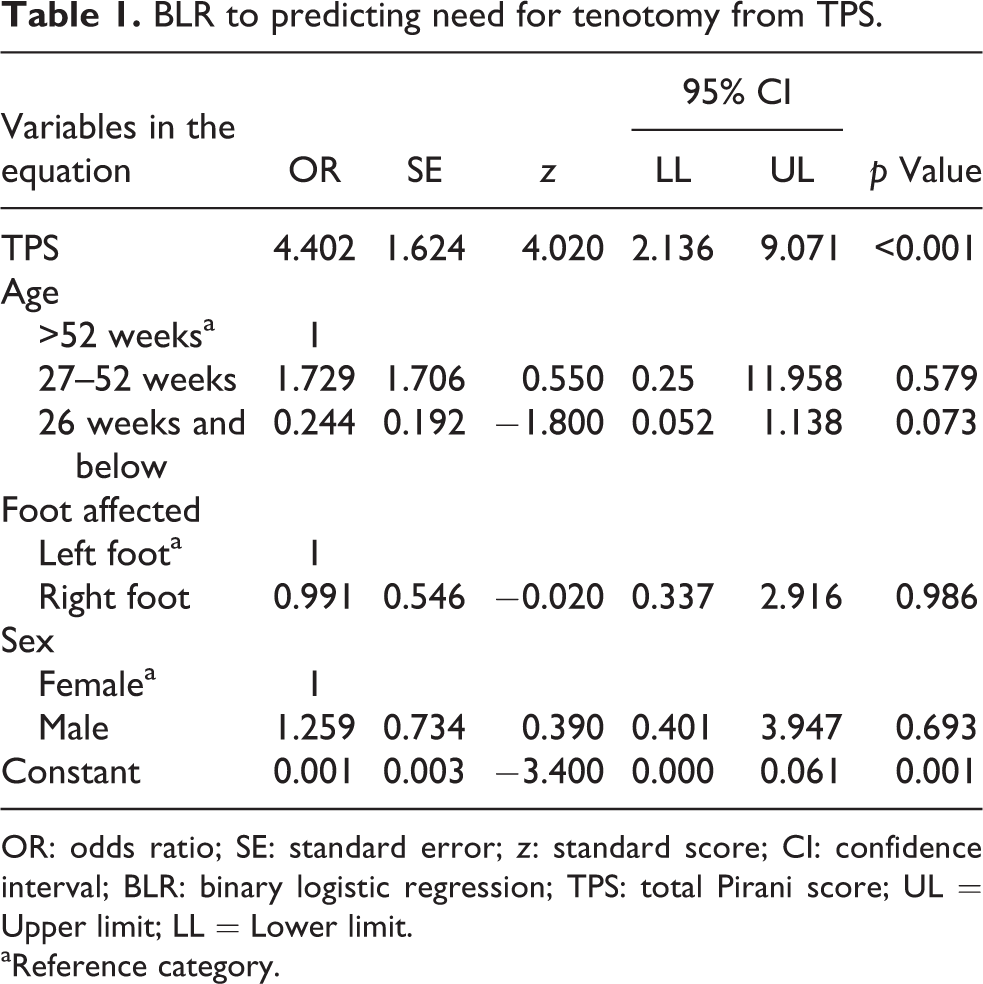
OR: odds ratio; SE: standard error; z: standard score; CI: confidence interval; BLR: binary logistic regression; TPS: total Pirani score; UL = Upper limit; LL = Lower limit.
aReference category.
The predicted value for whether or not tenotomy will be required from the above model was derived. The model predicted correctly 76.2% of the time among these patients whether or not tenotomy was done (R = 0.531, p < 0.001; κ = 0.526, p < 0.001), having taken account for age, sex, total Pirani score (TPS), and foot affected. When no other predictors apart from TPS are included in a BLR model, a similar result is gotten as shown in Table 2.
BLR to predicting need for tenotomy from TPS.

BLR: binary logistic regression; TPS: total Pirani score; OR: odds ratio, SE: standard error, z: standard score; CI: confidence interval.
This implies that the initial TPS is a very strong predictor of the future requirement for tenotomy, with a prediction correctness of 72.6%. Further analysis was carried out using the components of the TPS (midfoot score and hindfoot score) separately as predictors for the need for tenotomy. The result indicated that the hindfoot score was a much better predictor for the need for tenotomy than both the total score and the midfoot score with the model correctly predicting 75% of the time compared to the midfoot (67% correct prediction) and the total score (72.6% correct prediction).
An ROC curve was used to derive a cutoff point above which the need for tenotomy can be confidently predicted as illustrated in Figure 1. The ROC curve for determining the cutoff value for whether or not tenotomy will be done yielded an area under the curve of 0.801 (95% confidence interval, 0.707–0.894, p < 0.001) with a standard error of 0.048.
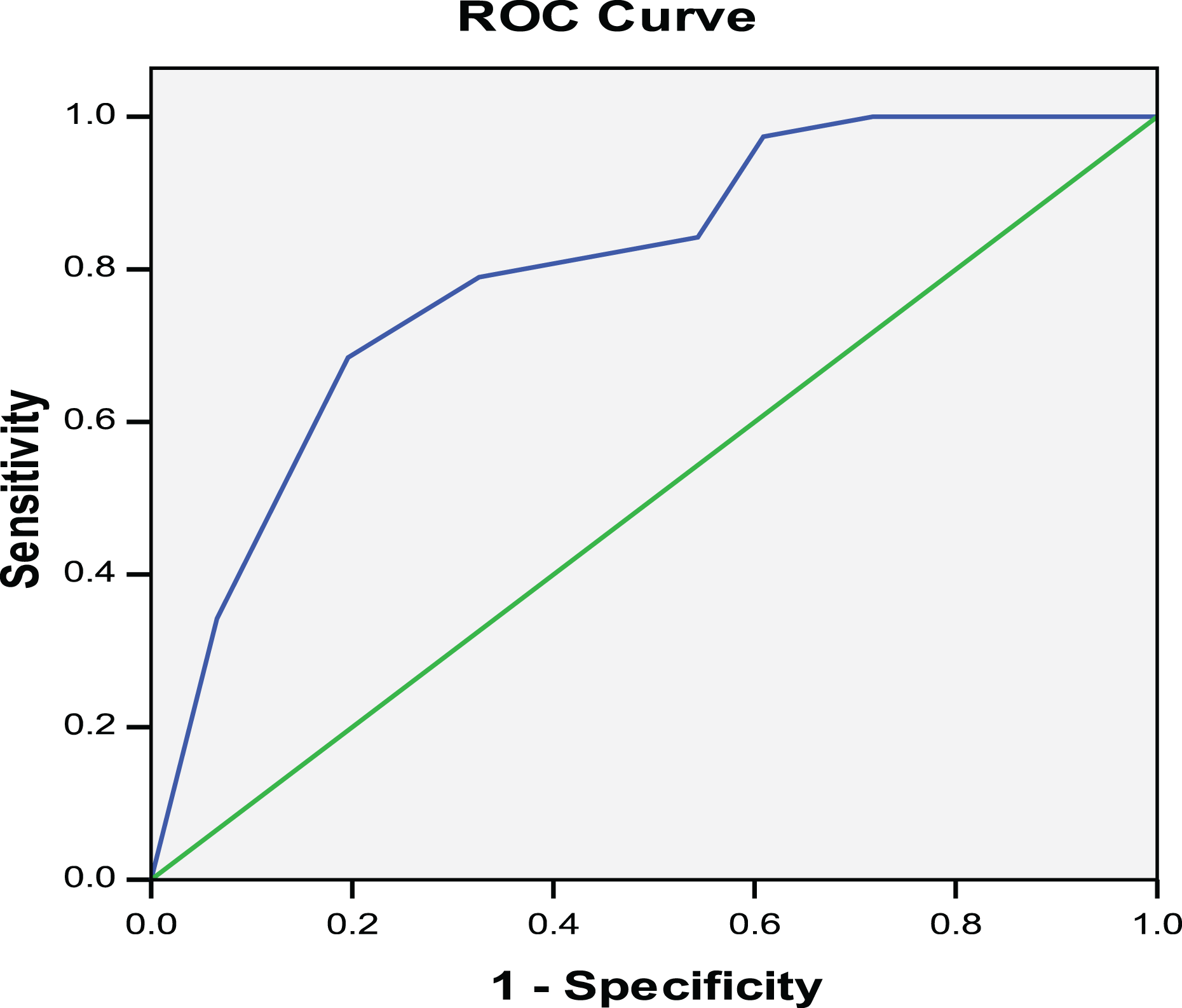
Deriving cutoff for TPS. Diagonal segments are produced by ties. TPS: total Pirani score; ROC: receiver operating characteristic.
The TPS maximizes sensitivity and at the same time minimizes “1-specificity” is 4.75. Thus, it can be concluded that 4.75 is the TPS above or below which the requirement for tenotomy can be confidently predicted. Using the cutoff point of 4.75, all patients with TPS less than 4.75 were categorized as having low Pirani scores, and all patients with TPS more than 4.75 were categorized as having high Pirani scores. Low Pirani here means that the patient will not require tenotomy, while high Pirani means the patient will require tenotomy. Sensitivity and specificity were then calculated using the clinically observed data as the gold standard for which to compare the derived TPS cutoff.
The sensitivity using 4.75 as cutoff is 78.9%, while the specificity is 67.4%
Discussion
Congenital talipes equinovarus (clubfoot) is the most common congenital abnormalities presenting to the orthopedic surgeon 8 and a major cause of concern to the parents of such patients, being a structural deformity clearly visible to all. In view of the growing interest in the management of clubfoot using the Ponseti method, various scoring systems were also established, one of which is the Pirani scoring system due to the simplicity of its application. In order to determine the predictability for the need for tenotomy based on the Pirani score at presentation, the difference between the mean score for the group which had tenotomy and those who did not have tenotomy was found to be positive. This implies that patients who have a higher Pirani score at presentation are more likely to have a tenotomy. This is in agreement with Dyer and Davis 5 in their study on the role of the Pirani scoring system in the management of clubfoot by Ponseti method where they reported a significant difference between the mean initial Pirani scores for the tenotomy (4.96; 2–6) and non-tenotomy (4; 1–6) groups, respectively (p = 0.012).
On further analysis using the BLR, the odds of requiring a tenotomy increases by more than fourfold for every unit increase in Pirani score. When the age of patients was considered, it was noted that those who are 6 months old or below are less likely to need tenotomy as compared to patients who are older than 1 year of age as seen in Table 1. Sex and foot affected were found not to be significant predictors of the need for tenotomy as reported in earlier studies. 5,9,10
Using the regression model to predict the need for tenotomy showed both a strong correlation and an agreement between the model’s prediction and the observed need for tenotomy in idiopathic clubfoot. A predictive value as high as 76.2% when all variables were considered and a value of 72.6% when Pirani score was singled out as the only variable considered implies that the initial TPS is a very strong predictor of the future requirement for Tenotomy as shown in Table 3. We also established the hindfoot score to be a better predictor for the need for tenotomy than both the TPS and the midfoot score supported by Dyer and Davis. 5 This stands to reason as the hindfoot score includes an assessment of the DF which is primarily influenced by the tightness of the Achilles tendon.
Prediction based on singular independent variable model (TPS).a

TPS: total Pirani score.
a R = 0.462; p < 0.001; κ = 0.456; p < 0.001.
Conclusion
In this study, a Pirani score above the cutoff point of 4.75 can confidently predict the need for tenotomy. This is similar to the value of 5 obtained by Scher et al. 11 where they compared Pirani and Dimeglio scores. In that study, 85% of patients with scores above 5 required tenotomy. Our findings therefore correlate with previous studies and affirm the value of the TPS and hindfoot score in predicting correctly whether or not a patient will need tenotomy in the correction of an idiopathic clubfoot. This will guide both the surgeon and parents on the management needs right from the patients’ first clinic visit.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.