
Abstract
Purpose:
The risk of superficial surgical site infection (SSI) and periprosthetic joint infection (PJI) after glove perforation is not evident. This study was to identify risk factors for glove perforation in primary TKR (total knee replacement) and the risk of subsequent superficial SSI and PJI.
Methods and materials:
Results of visible glove perforation of both inner and outer gloves during TKR were reviewed. A case–control analysis was performed on the preoperative and operative variables to identify predictive risk factors for glove perforation. Rate of SSI and PJI was compared between perforation and non-perforation groups, including 1226 series and 183 case–control subset.
Results:
One thousand two hundred twenty-six primary TKR from 2011 to 2014 was reviewed. Fifty-five knees had visible glove perforations. The operation perforation rate was 4.5%. Risk factors identified were body mass index (BMI) > 30, bilateral surgery, operation time >120 min and non-trainee surgeons. Superficial SSI was significantly higher in glove perforation group (9.15 vs. 0.51% and 0.55%). PJI was not significantly different (1.82% vs. 0.60% and 1.1%). The adjusted odds ratio for superficial SSI after perforation was 15.2, independent of BMI and operation time.
Conclusion:
Visible glove perforation in TKR is associated with several risk factors. The risk of superficial SSI is higher after perforation.
Keywords
Introduction
Glove perforation poses a significant risk in total joint arthroplasty. Not only are surgeons exposed to the risk of blood-born infectious disease like human immunodeficiency virus and hepatitis B, C or D, 1 patients are also exposed to the risk of superficial surgical site infection (SSI) and deep periprosthetic joint infection (PJI). The consequence could be disastrous, requiring removal of prosthesis, prolonged antibiotic treatment and further revision surgeries. Even after successful eradication of infection, the final functional outcome may likely be worse than an uneventful primary arthroplasty. 2
In fact, glove perforation is quite common in surgery. The perforation rate per glove ranged from 3.5% to 22.7% 3 –14 and the perforation rate per surgery ranged from 18.3% to 73%. 3,10 –12,14 –16 Major orthopaedic surgeries like total joint arthroplasty which involves contact with objects such as sharp bone edges, pins, osteotomes and metallic implants are particular susceptible. 9,12 –14,16 Nevertheless, the implication of glove perforation with regard to superficial SSI and deep PJI is not evident. 5,17,18 The reported incidence of infection after perforation ranged from 0% 5,17 to 7.5%. 18 Although there were a number of studies on glove perforations, only very few reported the clinical outcome of patients with perforated gloves during total joint arthroplasty. 5,17
The aim of the study was to identify risk factors for glove perforation in total knee arthroplasty and to review the clinical outcome of involved patients in terms of superficial SSI and deep PJI.
Materials and methods
Patients with primary total knee arthroplasty performed in our institute from October 2011 to September 2014 were reviewed. Revision cases of unicompartment arthroplasties were excluded.
Operative protocol
All knee arthroplasties were performed with the use of prophylactic antibiotics, body exhaust suits, impermeable drapes, pulsatile lavage and non-antibiotic-impregnated cement. Implants used were uniformly posterior-stabilized prostheses with all-poly patella. All had medial parapatellar approach, blood tourniquet until wound dressing, skin closure with staples and compressive wound dressing. All procedures including wound closure were done by the chief surgeons. Drain was used in all cases and was routinely removed on post-operative day 1. Prophylactic antibiotic regime was cephazolin 1 g on induction, then 1-g 8-hourly for two dose after operation. Vancomycin 500-mg infusion in 2 h was used instead if there was drug allergy to penicillin group. All surgeries were performed with double gloves. Separate gloves were worn for draping. Surgery began after changing of all gloves for draping. Outer gloves were changed before cementation. In the case of any noticeable perforation in either outer or inner gloves, both inner and outer pairs of gloves were changed together.
Evaluations
Glove perforation of any members involved in surgery was recorded in the computerized operation record. This was one of the obligatory report items of surgical audit checklist in our institute. Detection of perforation was made by direct vision by individual surgical member. Perforation was confirmed by the presence of holes on both gloves or the presence of fluid inside the inner gloves. 17
Diagnostic criteria for PJI were based on guidelines from the Musculoskeletal Infection Society workgroup, 19 which defines three grounds on which a joint may be considered to be infected: (1) a sinus tract in communication with the implant is noted; (2) two separate fluid or tissue cultures from the joint yield a pathogen; or (3) at least four of the following six criteria are met: (a) elevated serum erythrocyte sedimentation rate (> 30 mm/h) or C-reactive protein level (>10 mg/L), (b) any elevated leukocyte count in the synovial aspirate, (c) any increased PMN percentage in the synovial aspirate, (d) gross purulence in the synovial aspirate, (e) one fluid or tissue culture yielding a pathogen, or (f) frozen tissue sections with more than five PMNs per high power field in at least five fields.
Diagnostic criteria for superficial SSI were according to CDC: 20 infection occurs within 30 days after the operation and infection involves only skin or subcutaneous tissue of the incision and at least one of the following: (1) purulent drainage, with or without laboratory confirmation, from the superficial incision; (2) organisms isolated from an aseptically obtained culture of fluid or tissue from the superficial incision; (3) at least one of the following signs or symptoms of infection: pain or tenderness, localized swelling, redness, or heat and superficial incision is deliberately opened by surgeon, unless incision is culture negative; (4) diagnosis of superficial incisional SSI by the surgeon or attending physician.
All outcome measurements were performed by independent observers (orthopedic specialist nurses) who were blinded to the operation detail.
Data retrieval was performed through clinical data analysis and reporting system in our institute. Keywords for data search were primary knee arthroplasty and glove perforation.
Statistical analysis
A case–control analysis was performed on the preoperative and operative variables to identify predictive risk factors for glove perforation. Consecutive primary knee arthroplasties without glove perforations performed in October 2012 and March 2013 (6 months) were used as control. Since there were around 30 cases of primary arthroplasties performed each month in our institute, the 6-month period would include 183 cases as control with 1:3–1:4 case–control ratio. Since there was no change in any surgical practice and perioperative protocol during this period from the rest of the study period, this cohort of control was assumed to be representative of the study base. Potential risk factors analysed included sex, age, body mass index (BMI), bilateral surgery, use of navigation, operation time, complex surgery, trainee surgeons and surgeon number. Bilateral surgery was defined as sequential surgeries on both knees under single anaesthesia. Complex surgery was defined as surgery involving ligament repair or additional implants such as screws, stems or augments. Surgeon number was inclusive of chief and assistant surgeons. Data analysis was performed by SPSS 20. Univariate analysis was performed with χ2 test and unpaired t-test for categorical and continuous data, respectively. To adjust for the confounding effects of multiple variables, multivariate analysis with multiple logistic regressions was performed. Statistical significance was defined as p < 0.05.
Results
There were 1226 knees from October 2011 to September 2014. There were 432 NexGen Legacy PS Knee (Zimmer, Warsaw, Indiana, USA), 540 Triathlon PS Knee (Stryker, Mahwah, New Jersey, USA) and 254 PFC Sigma PS Knee (Depuy, Leeds, England). Three hundred two knees were performed with ASM navigation guidance (Stryker). The mean follow-up period was 22.7 months (6–41). Fifty-five knees had visible glove perforation during operation. The perforation rate per operation was 4.5% (55/1226).
Risk factors for perforation
Case–control analysis showed no significant difference in the incidence of preoperative comorbidities among two groups (Table 1). Significant risk factors for glove perforation identified χ2 or t-test included young patient age, high BMI, bilateral surgery, navigation surgery and non-trainee surgeons. Significant risk factors identified by multiple logistic regression included BMI > 30, bilateral surgery, operation time >120 min and non-trainee surgeons (Table 2).
Basic demographic parameters of case–control subset.

BMI: body mass index.
a p < 0.05.
Possible risk factors for glove perforation.a
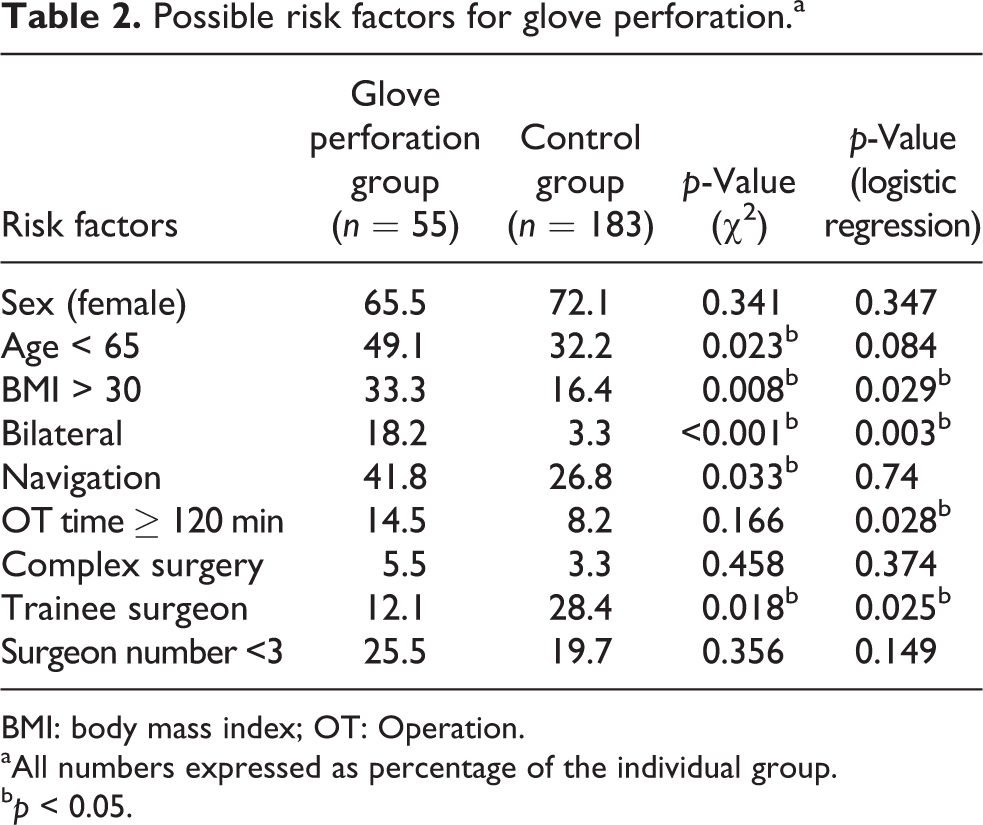
BMI: body mass index; OT: Operation.
aAll numbers expressed as percentage of the individual group.
b p < 0.05.
Infection after perforation
The rate of superficial SSI was 9.1% (5/55) in perforated cases. In contrast, it was 0.5% (6/1171) in all non-perforated cases and 0.5% (1/183) in the subset control group (Table 3). All except one of the SSI cases in the perforated group were successfully treated with 1 week of oral antibiotic. The failure case initially responded to 1 week of antibiotic with good skin union. She developed subsequent chronic PJI.
Infection complications.
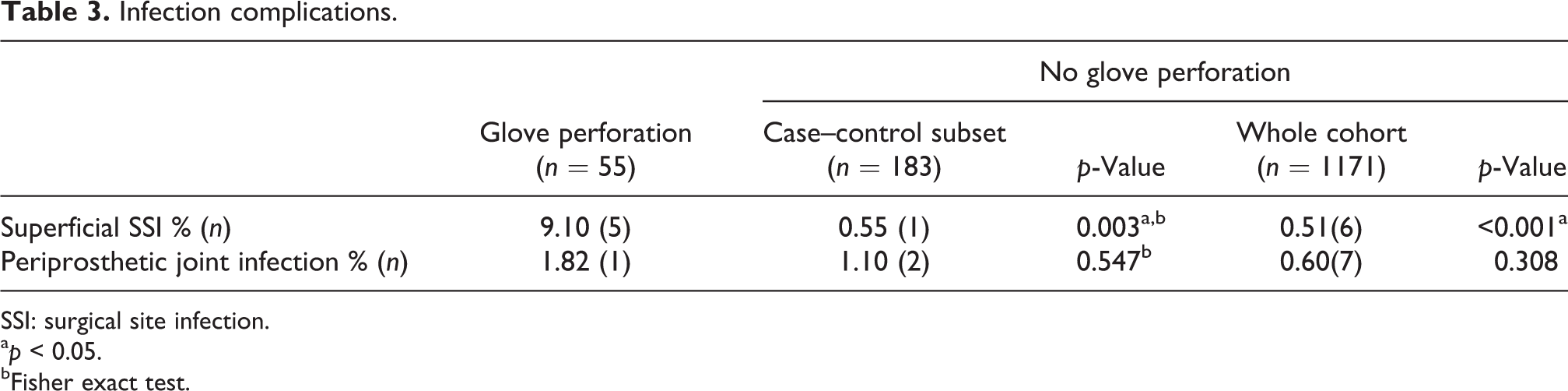
SSI: surgical site infection.
a p < 0.05.
bFisher exact test.
The rate of PJI was 1.8% (1/55) in perforated cases, while it was 0.65% (8/1226) in all non-perforated cases and was 1.1% (1/183) in the subset control group. The organisms involved in PJI were Staphylococcus aureus (50%), coagulase-negative Staphylococcus (25%), Pseudomonas (one case) and methicillin-resistant S. aureus (one case).
Among the three possible risk factors for superficial SSI, glove perforation was identified as the only significant independent factor with adjusted odds ratio of 15.2 (95% confidence interval: 1.6–141.5; Table 4).
Adjusted risk and possible confoundings for superficial SSI with glove perforation.a

SSI: surgical site infection; BMI: body mass index; OT: operation.
aMultivariate analysis with multiple logistic regressions.
b p < 0.05.
Discussion
In the present study, the 4.5% glove perforation rate per surgery was quite low compared with the literature. 3,10 –12,14 –16 The high perforation rate of 18.3–73% in most studies was based on the water-leak test 21 rather than gross inspection by direct vision. Based on the water-leak test, the sensitivity of gross inspection was reported to be only 10–37%. 6,10 –12,15,16 However, the water-leak test is a manufacturing standard. The distention of glove with 1 L of water and the leakage of water from inside out under high pressure might not be a good representation of real clinical setting. So far, no association has been established between the water-leak test and the risk of wound complication or SSI. Instead, Misteli et al. 17 suggested that glove perforation defined by gross inspection might be of greater clinical relevance.
The study has identified several risk factors for glove perforation: young patient age, high BMI, bilateral surgery, navigation surgery and non-trainee surgeons were identified by χ2 test or t-test; BMI > 30, bilateral surgery, operation time >120 min and non-trainee surgeons were identified by multiple logistic regressions.
The average age of the glove perforation group was lower (66 vs. 69.5) and age <65 was found be a significant risk by χ2 test. One explanation could be younger patients with higher bone density led to greater risk of glove perforation due to micro-trauma by harder bone. There is no study in literature having identified this association so far. The other explanation could be the selection bias in bilateral surgery. For obvious reasons, patients with younger age and better fitness were chosen for bilateral surgery. The lack of statistical significance of age in multiple regressions suggested the latter explanation a higher possibility.
Consistently, high BMI (29 vs. 27) was identified by t-test and BMI > 30 was identified by multiple regressions as significant risk factors. These agree indirectly with the finding by Palmer and Rickett 12 that operations requiring manipulation of instruments deeper within the wound had a higher rate of perforation. The present study could be the first to report the direct association between high BMI and the risk of glove perforation in total joint arthroplasty.
Bilateral surgery was identified as risk factor by both χ2 test and multiple regressions. The proportion of bilateral surgery was 18.2% in the perforation group versus 3.3% in the control. This finding could also be the first in the literature. As a routine in our institute, gloves were changed after the first surgery before starting the second in bilateral surgery. Also the recorded operation time was counted for each knee. Therefore, the higher risk of perforation in bilateral surgery could not be explained by the doubled operation time. One possibility was the reduced dexterity of surgeons due to fatigue during the sequential surgery because all the bilateral cases had both knees performed by the same surgeon. Nevertheless, Demircay et al. 7 has found more glove perforation in the first half of surgery in hip and knee arthroplasty. The present study however did not study the timing of perforation during the bilateral surgery.
Navigation was found to be a significant risk factor by χ2 test. The use of sharp metal pins and repeated assembly and disassembly of instruments during navigation might have increased the perforation risk. However, the lack of statistical significance in multiple regressions suggested a confounding factor behind. One possibility was that all our bilateral surgery cases were performed under navigation guidance such that bilateral surgery could be the culprit rather than navigation itself.
Operation time >120 min was found to be a significant risk by multiple regressions. This agrees with the findings in other studies. 4,14,16 Complex surgery was not found to be significant. So far, there was no research having included the complexity of the primary arthroplasty in the study of glove perforation, although Carter et al. 6 have found a higher rate of perforation in revision hip or knee cases. However, the number of complex primary surgery was small (three in perforation; six in control) such that there was inadequate power in the analysis.
Non-trainee was found to be a significant factor by both χ2 and multiple regressions. One possible explanation was a higher detection or reporting rate by non-trainee. There were conflicting evidences on this issue from different studies. While Palmer and Rickett 12 reported a higher risk of perforation in consultants than juniors, Maffulli et al. 16 reported a higher risk in residents in the first 2 years of their program.
The 25.5% of glove perforation group had surgeon number <3 versus 19.7% in the control group. Although the lower the number of surgeons involved in surgery, the more difficult the surgery might be for the surgeon, the difference was not significant. So far, there was no previous study correlating the number of surgeons with the rate of perforation.
The rate of superficial SSI was found in the present study to be significantly higher in the perforated group (9.1% vs. 0.51% in the whole cohort and 0.55% in the subset control). Analysis along with BMI > 30 and operation time > 120 min by multiple logistic regressions showed that glove perforation was the only significant independent risk factor for superficial SSI. The adjusted risk of superficial SSI in patients with visible glove perforation was 15 times of those without perforation. This finding suggested that the apparent higher risk of superficial SSI in patients with high BMI or prolonged operation reported in many studies could have been confounded by the factor of glove perforation, which was not included in most of these studies.
To one’s surprise, there were only very few studies reporting SSI as the outcome measure of glove perforation. Tanner and Parkinson 18 had reviewed 31 trials on glove perforation. Only two of the trials reported infection as the primary outcome. Both reported no infections. Misteli et al. 17 found that operation carried a fourfold increase of risk of SSI after glove perforation if no antibiotic prophylaxis was given. However, the risk in those with prophylactic antibiotics was not increased. The present study seems to be the first to report an independent association of glove perforation with SSI in joint arthroplasty surgery. Fortunately, the consequence of superficial SSI seemed favourable when appropriate treatment was given. Only 1 of 11 cases developed subsequent PJI. This agrees with the finding by Guirro et al. 22
The rate of deep PJI was not significantly different (1.8% vs. 0.6% in whole cohort and 1.1% in the subset control). However, due to the low incidence of PJI, the sample size in present study did not have adequate power for analysis. A post hoc calculation showed that a total sample size of around 10,000 is required to detect any significant difference with such low outcome incidence.
Because of the high rate of glove perforation along with the increased risk of disease transmission and wound contamination, double gloving 7,9,10,13 –15,18,23 with frequent glove change at regular interval 4,5,23 has been advocated by many authors. The present study further confirms the need for such practice in knee arthroplasty especially in patients with high BMI, long operation time and bilateral surgery. Surgeons are to be particularly vigilant in these ‘high risk’ arthroplasty cases. Specific types of glove to increase the awareness of glove perforation have been found effective, 11 while latex-free gloves are best avoided in such cases due to their higher risk of perforation. 3,8,24
There were several limitations of the present study. First, the data capture depended on volunteer record of perforation, which might result in under-reporting due to reasons like legal liability of the surgeons. Second, the causes of glove perforation were not reported as part of the audit. It was assumed different causes of glove perforation had similar bearing on the consequence. Future study may look into the question whether perforation due to needle puncture has different risk of superficial SSI than perforation due to prolonged surgery. Third, the mean follow-up period in the present study was 22.7 months with the shortest follow-up time of 6 months, which was adequate for most superficial SSI but a longer follow-up time would be more satisfactory for PJI. Finally, the rate of PJI in total joint arthroplasty is not high (0.60–1.8% in this study) such that a very large study sample was required to have adequate power to detect any significant difference. 18
Conclusion
The study has found the rate of visible glove perforation 4.5% in primary total knee arthroplasty. Risk factors for perforation identified were BMI > 30, bilateral surgery, operation time > 120 min and non-trainee surgeons. The consequence of perforation is increased the risk of superficial SSI.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.