
Abstract
Background: Patients with inflammatory arthritis are at increased risk of prosthetic joint infections (PJIs), but diagnosis in these patients can be challenging because active inflammatory arthritis produces elevated inflammatory markers that may mimic those seen in PJI. Purpose: In this pilot study, we sought to identify the clinical, microbiologic, and histopathologic features of culture-positive and culture-negative PJI in patients with inflammatory arthritis who underwent total hip arthroplasty (THA) or total knee arthroplasty (TKA). We also sought to obtain preliminary data to support a definitive study of optimal methods for PJI diagnosis in patients with inflammatory arthritis. Methods: We performed a retrospective analysis of TKA and THA patients treated for PJI from 2009 to 2018 at a single tertiary care orthopedic institution. Data were extracted from a longitudinally maintained hospital infection database. We reviewed hematoxylin and eosin slides of osteoarthritis and inflammatory arthritis PJI cases matched 3:1, respectively, by age, sex, and culture status. Clinical characteristics were evaluated using the Fisher exact test, χ2 test, Student t test, and Mann-Whitney U test where appropriate. Results: A total of 807 PJI cases were identified (36 inflammatory arthritis and 771 osteoarthritis cases). Patients with inflammatory arthritis presented younger, had a higher Charlson Comorbidity Index, more frequently used glucocorticoids, were more likely women, and had a higher proportion of culture-negative PJI compared with osteoarthritis patients. Of the 88 inflammatory arthritis cases reviewed for histopathology, a higher proportion of culture-positive than culture-negative PJI cases had >10 polymorphonuclear leucocytes per high-power field and met Musculoskeletal Infection Society criteria but presented with less chronic inflammation. Conclusions: This retrospective prognostic study suggests that culture-negative PJI may be more frequent in patients with inflammatory arthritis than in those with osteoarthritis. Chronic infections, antibiotic use, or misdiagnosis may be contributing factors to unclear PJI diagnoses among culture-negative cases. This preliminary work supports the need for further studies to assess the differences in clinical features between culture-negative and culture-positive PJI in patients with inflammatory arthritis and the ability of biological diagnostic markers to discriminate between them in this population.
Keywords
Approximately 1 million total hip arthroplasties (THAs) and total knee arthroplasties (TKAs) are performed in the United States each year; for patients with advanced symptomatic arthritis, these procedures effectively decrease pain and improve function [5,16]. Prosthetic joint infection (PJI), a rare but devastating complication, occurs in 0.8% to 1.9% of TKAs and 0.3% to 1.7% of THAs, is the most common cause of TKA failure, and is the third most common cause of THA failure [6]. The risk of PJI after TKA or THA has been reported to be 50% to 80% higher for patients with inflammatory arthritis (IA) conditions, such as rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE) [4,19,21]. Epidemiologic studies have identified differences in the onset of PJI between osteoarthritis (OA) and RA patients; OA patients are at highest risk of PJI within 2 years of surgery, whereas for RA patients the risk of PJI persists for the life of the implant [3]. The increased risk of PJI in IA patients may be related to pharmacologic immunosuppression, immune dysregulation, and high disease activity [17,20,22]. However, the diagnosis of PJI in patients with IA is challenging because aseptic RA or SLE flares may mimic PJI both clinically (joint pain, swelling, and fever) and diagnostically (elevated C-reactive protein [CRP] level, erythrocyte sedimentation rate [ESR], and synovial leukocytosis) [12]. In addition, PJI diagnostic criteria do not provide guidance on differentiating PJI from RA flares, and few studies have comprehensively characterized PJI in patients with RA and SLE. Thus, there is a large knowledge gap in differentiating PJI in IA and OA patients (PJI-IA and PJI-OA). To date, little is known of the differences in clinical presentation, biomarkers, and histopathology.
We therefore sought to conduct a pilot study to provide baseline information for future research in the diagnosis and treatment of these complex cohorts. We sought to examine the histopathologic features of surgically managed total joint replacements for infection in IA and OA patients who had a secondary diagnosis of PJI—specifically, the effect of bacterial presence (positive intraoperative culture) on histological features within each diagnosis. In addition, we sought to gather patient demographics, clinical presentation, and treatment of IA patients with PJI.
Methods
We performed a retrospective analysis of TKA and THA patients treated for PJI from 2009 to 2018 at a single tertiary care orthopedic institution. Data were extracted from records in a longitudinally maintained hospital infection database. Institutional review board approval was waived for this study. Patients were included if they had an International Classification of Diseases (ICD) code denoting a diagnosis of PJI (ICD-10-CM T84.50XA) and the presumed PJI was managed surgically in conjunction with an infectious disease specialist. Inclusion criteria required at least 2 years of clinical and radiographic follow-up. Surgical treatment consisted of (1) debridement, antibiotics, and implant retention (DAIR); (2) 2-stage exchange arthroplasty; or (3) 1-stage exchange arthroplasty followed by at least 6 weeks of intravenous antibiotics in all cases prescribed by an infectious disease specialist. In addition, patients who retained hardware after irrigation and debridement were prescribed at least 6 months of suppressive oral antibiotics. The IA patients were defined as any patient with an ICD diagnosis code for RA (ICD-10 MO5-) or SLE (ICD 10-M32-) who received a prescription for disease-modifying antirheumatic drugs (DMARDs), biologics, or SLE-specific medications within 1 year of surgery [17,18]. Patients with no IA diagnosis were considered to have OA. Culture-negative (CN) patients had negative culture growth intraoperatively or preoperatively through aspirate culture growth [20,22]. For those with culture mismatch (preoperative and intraoperative findings that did not agree), an infectious disease specialist confirmed infection status through clinical evaluation of symptoms (erythema and systemic symptoms), medical history, and physical examination. Culture-positive (CP) patients had at least 1 preoperative or intraoperative aspirate culture growing any microorganism. Additional information collected from the hospital record included Musculoskeletal Infection Society (MSIS) major and minor criteria, prior history of orthopedic infection, chronic glucocorticoid use, type of DMARDs used, tobacco use, and Charlson comorbidities.
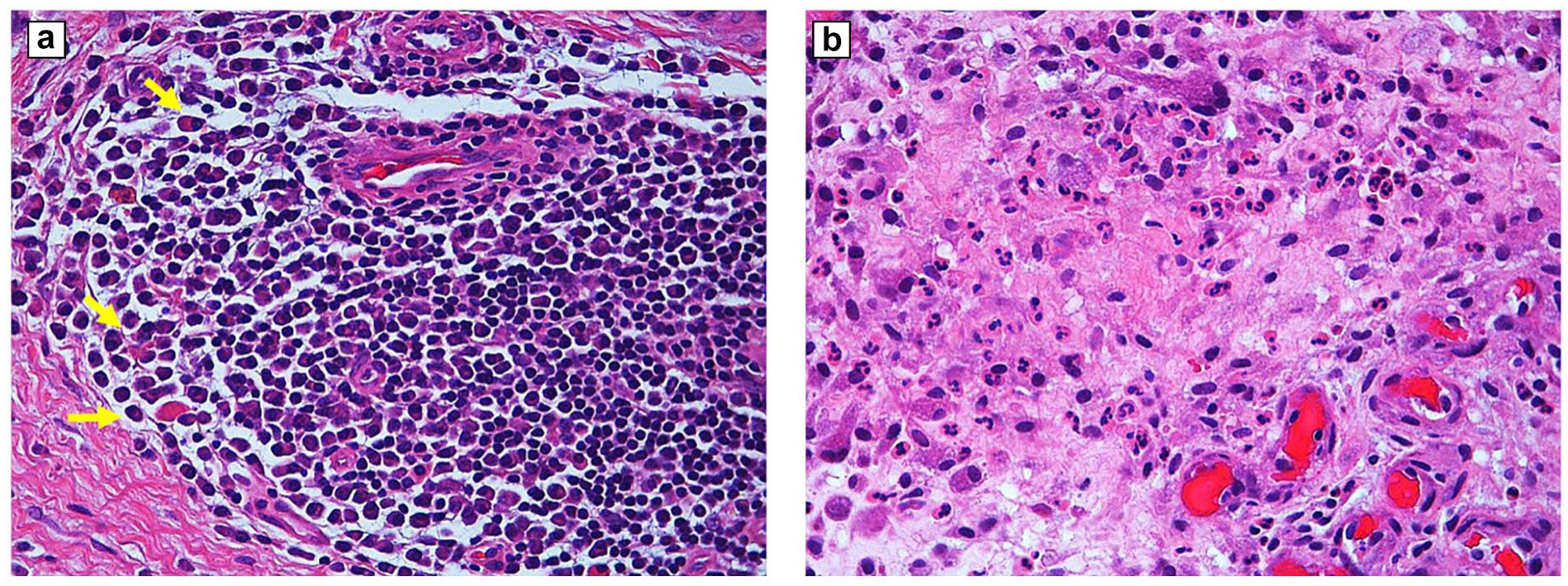
Hematoxylin and eosin (H&E)-stained slides of PJI cases in OA and IA patients were matched 3:1, respectively, by age (±5 years), sex, and culture status, and the available matched cases were then reviewed by an experienced musculoskeletal pathologist (T.P.) for histological evidence of infection. Following American Academy of Orthopaedic Surgeons (AAOS) guidelines, a polymorphonuclear leukocyte (PMN) count ≥10 per 5 high-power fields (HPFs) was considered positive histological evidence of infection and confirmed PJI diagnosis [15]. The 5 fields selected were the busiest in the section and, when possible, nonconsecutive. Chronic inflammation was reviewed according to the following scoring parameters: absent chronic inflammation = 0, scattered chronic inflammatory cells = 1, at least 1 lymphoid aggregate in 2 separate fields = 2, and more than 2 aggregates in 2 separate fields or a band-like pattern = 3. Tissue necrosis containing PMNs was reviewed according to the following parameters: absent = 0, small rare microabscesses = 1, visible areas of necrosis with purulent material = 2, and excessive purulent necrosis = 3 (Fig. 1). The study cohort was then subdivided into 4 groups for further comparison. Patients diagnosed with IA and OA were stratified by intraoperative culture results: IA and culture-positive (IA-CP, N = 26); IA and culture-negative (IA-CN, N = 10); OA and culture-positive (OA-CP, N = 662); and OA and culture-negative (OA-CN, N = 109).
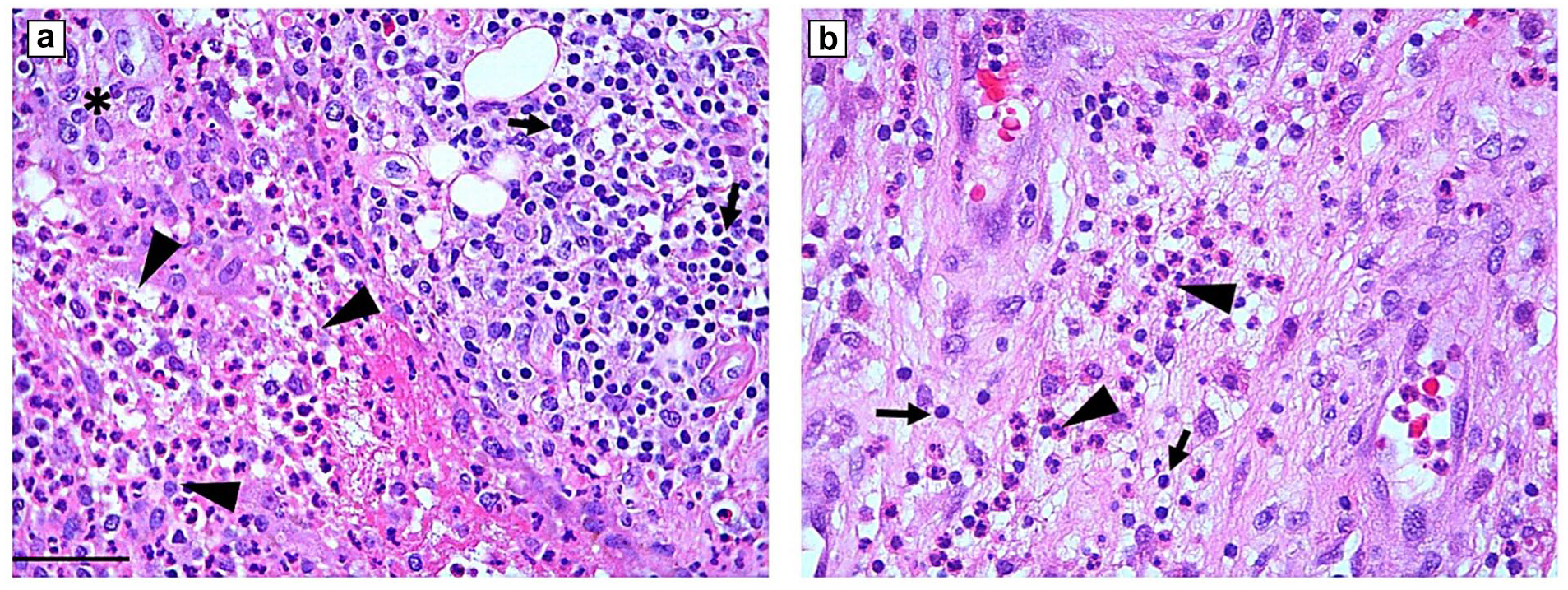
Hematoxylin and eosin slides demonstrating overlapping features of chronic and acute inflammation, showing high field image with more than 10 PMNs (arrowheads) meeting criteria for infection and confirming PJI. (a) A dense infiltrate of lymphocytes (arrows) and monocytes (*) typical of chronic inflammation in addition to the features of acute inflammation. (b) The majority of inflammatory cells are granulocytes and scattered chronic inflammatory cells (arrows). 400× magnification. Bar = 50 µm. PMN polymorphonuclear leucocyte, PJI prosthetic joint infection.
Debridement, antibiotics, and implant retention involved complete synovectomy and exchange of modular components. Two-stage revision consisted of initial removal of components, total knee or hip replacement bone resection cuts, placement of a high-dose antibiotic spacer, 6 weeks of intravenous or oral antibiotics followed by minimum 2-week antibiotic holiday, and definitive prosthetic joint insertion after reassessment for persistent infection. One-stage revision consisted of complete synovectomy, removal of components, total knee or hip replacement cuts, preliminary wound closure with re-sterilization and draping, and placement of definitive prosthesis components [6].
Statistical Analysis
Descriptive statistics were used to characterize histopathological presentation for each group. Demographics and clinical characteristics were analyzed using the following: categorical data were analyzed with the Fisher exact square tests or the χ2 test, and continuous data were analyzed using a Student t test or Mann-Whitney U test based on data distribution. Significance was set at α < 0.05. Statistical analyses were performed using SAS 9.4.
Results
A total of 807 cases of PJI were identified, including 36 cases of IA (33 had RA and 3 had SLE) and 771 cases of OA (Table 1). Among the 807 PJI cases, the CN rate was 14.7%, and the rate was significantly higher (P = .024) in patients with IA (27%, n = 10) than in patients with OA (14%, n = 109). Histopathology from age, sex, and culture-matched OA-IA cohorts (n = 88 PJIs; 31 IA and 57 OA) was reviewed. Histological signs of high chronic inflammation (scores of 2 or 3) were significantly higher in the IA group than in the OA group (74% vs 23%, P < .001) (Tables 2 and 3).
Patient characteristics in inflammatory arthritis and osteoarthritis PJIs. a
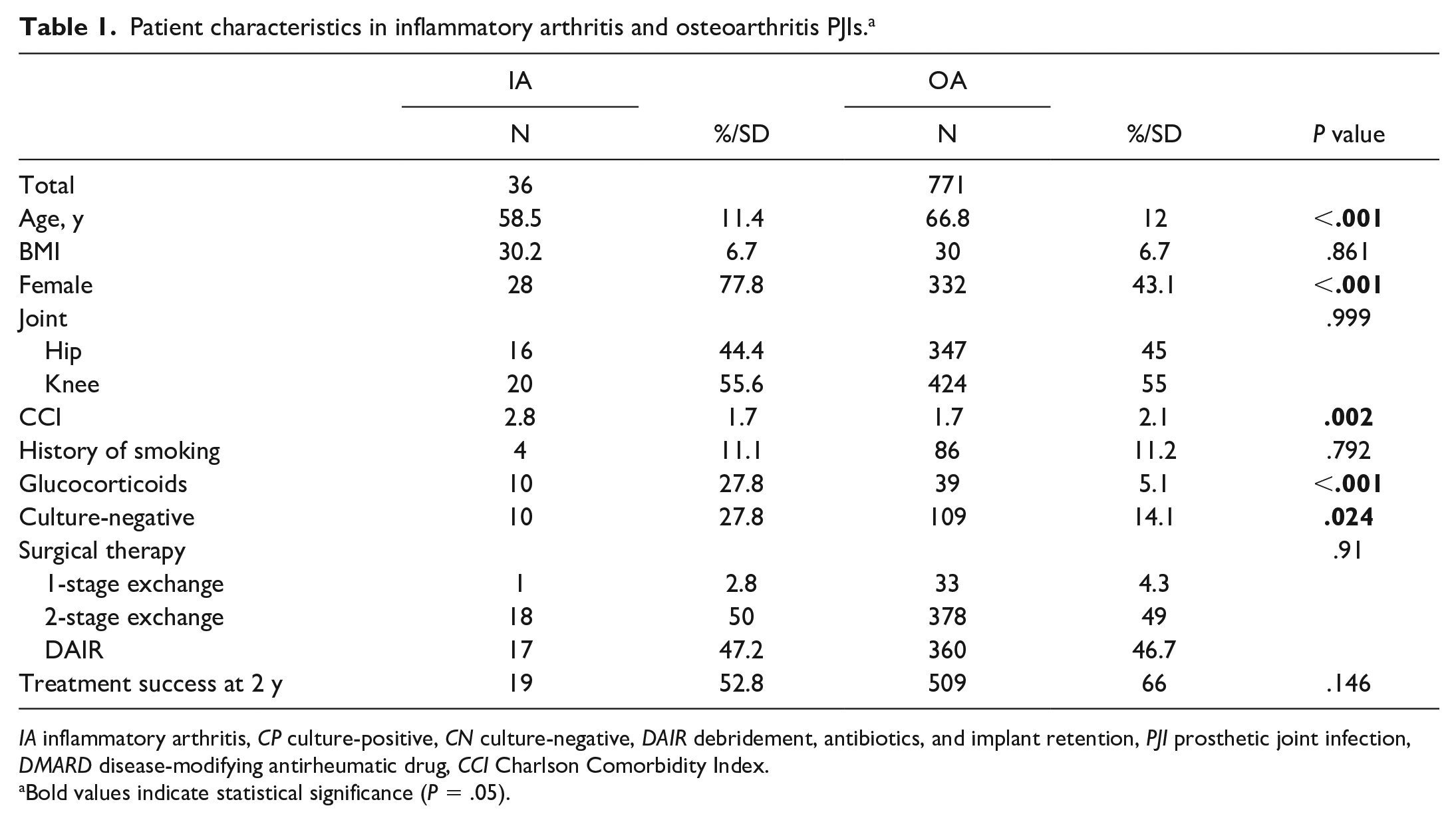
IA inflammatory arthritis, CP culture-positive, CN culture-negative, DAIR debridement, antibiotics, and implant retention, PJI prosthetic joint infection, DMARD disease-modifying antirheumatic drug, CCI Charlson Comorbidity Index.
Bold values indicate statistical significance (P = .05).
Patient characteristics of PJI-IA stratified by intraoperative culture results.
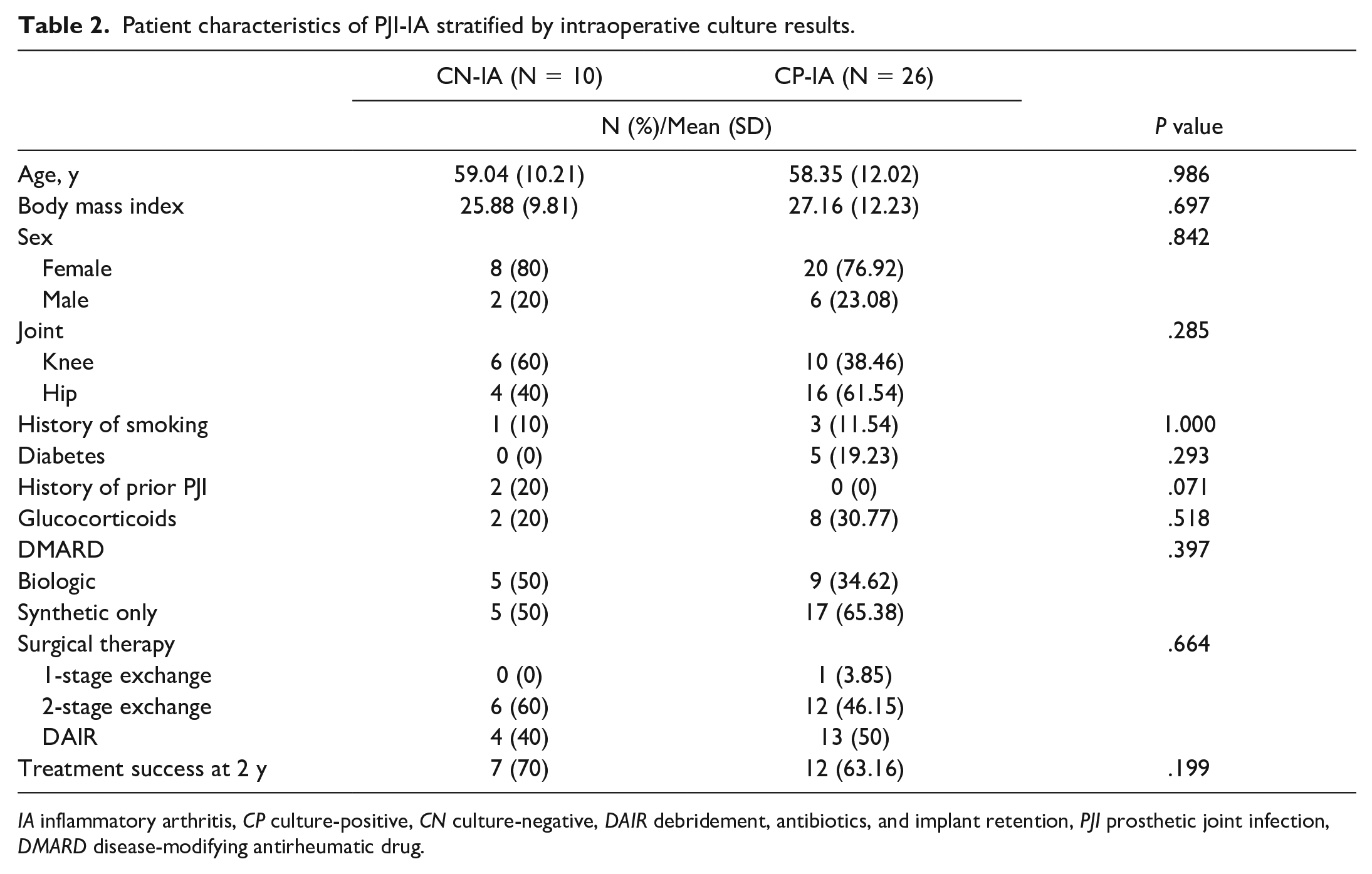
IA inflammatory arthritis, CP culture-positive, CN culture-negative, DAIR debridement, antibiotics, and implant retention, PJI prosthetic joint infection, DMARD disease-modifying antirheumatic drug.
Histopathology and clinical presentation in inflammatory arthritis and osteoarthritis PJIs.
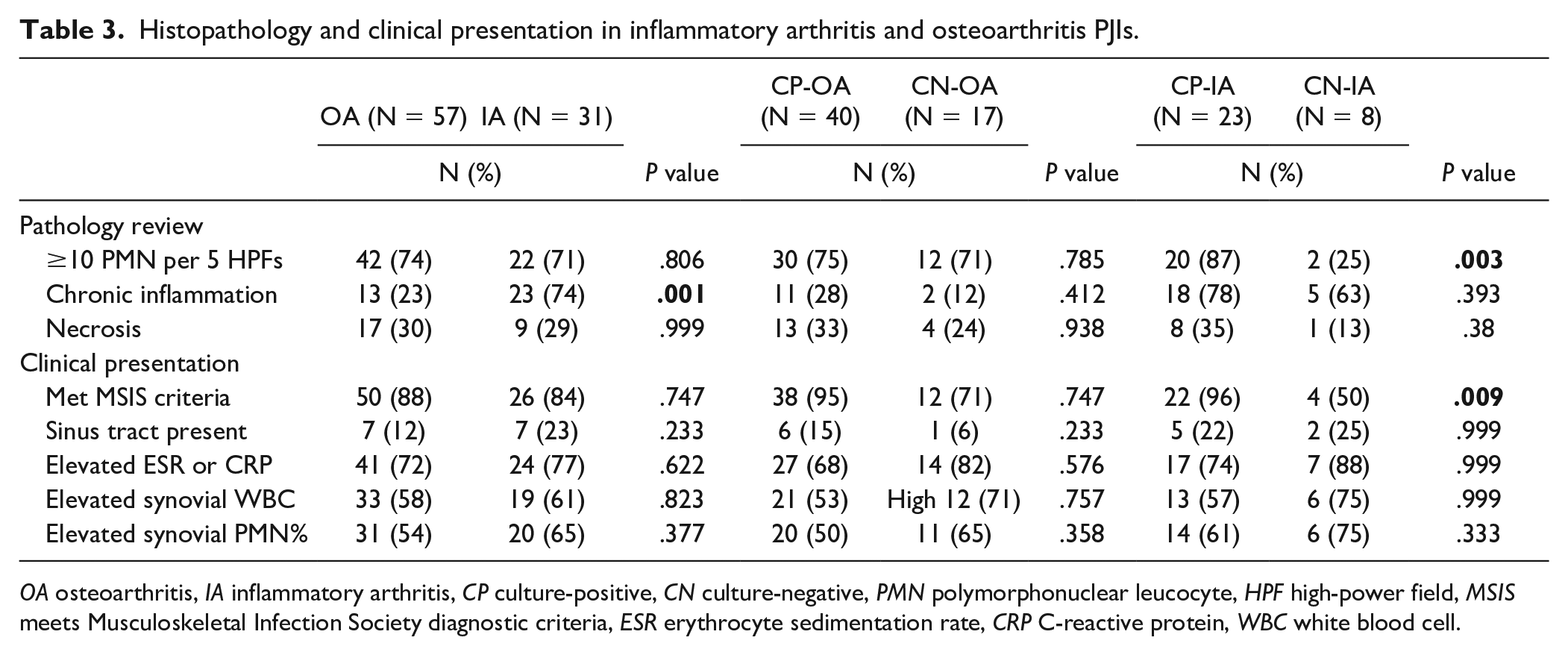
OA osteoarthritis, IA inflammatory arthritis, CP culture-positive, CN culture-negative, PMN polymorphonuclear leucocyte, HPF high-power field, MSIS meets Musculoskeletal Infection Society diagnostic criteria, ESR erythrocyte sedimentation rate, CRP C-reactive protein, WBC white blood cell.
When the PJI-IA cohort was stratified by intraoperative culture results, there were no differences between CN and CP at baseline (Table 2).
When evaluated, OA and IA patients were similar in presentation. The only statistically significant difference between the groups was the presence of chronic inflammation (P = .0001); other characteristics reviewed were found to be nonsignificant.
In a sub-analysis of CN IA and OA patients, fewer IA-CN patients were found positive for PJI based on PMN count compared with OA-CN patients, but the difference was not significant (P = .08). Patients with IA-CN were younger than those with OA-CN (59 vs 69 years, P = .01).
In a sub-analysis of CP IA and OA patients, there was no difference in diabetes, comorbidities, smoking, or history of PJI, but more patients with IA-CP were women (P < .001), younger (P < .001), and used glucocorticoids (P < .001) as is typical for RA and SLE. Across all CP cases, 57% were staphylococcal infections, with no differences between groups. Overall, surgical treatment included 2-stage exchange (55%), DAIR (39%), and 1-stage exchange (4.5%), with no difference between groups (P = .8). There was a trend toward treatment failure for IA-CP, but the difference was not significant (P = .2).
Comparing CN and CP IA patients, no differences were observed in age, smoking, diabetes, or Charlson comorbidities, but there was a trend toward higher prevalence of prior PJI in the CN group (Table 2). No differences were found in surgical treatment or use of biologics and DMARDs between IA-CN and IA-CP patients. A lower proportion of patients with IA-CN had positive histology for acute infection—that is, ≥10 PMN per 5 HPFs (0.003) and met MSIS criteria (0.009)—than did those in the IA-CP cohort (Table 3). There was no statistically significant difference in ESR, CRP, or WBC count between CN and CP IA patients (Table 4). The majority of the IA-CN group (63%) had signs of high chronic inflammation (scores of 2 or 3) and only 25% had histological signs of acute infection compared with 87% of the IA-CP group (P = .003). The cases of IA with only chronic inflammation had typical perivascular or interstitial chronic lymphocytic infiltrate, with differing amounts of plasma cells. They showed a minor component of PMN cells, although not reaching the cutoff for acute infection (Fig. 2).
Preoperative presentation of PJI-IA patients.
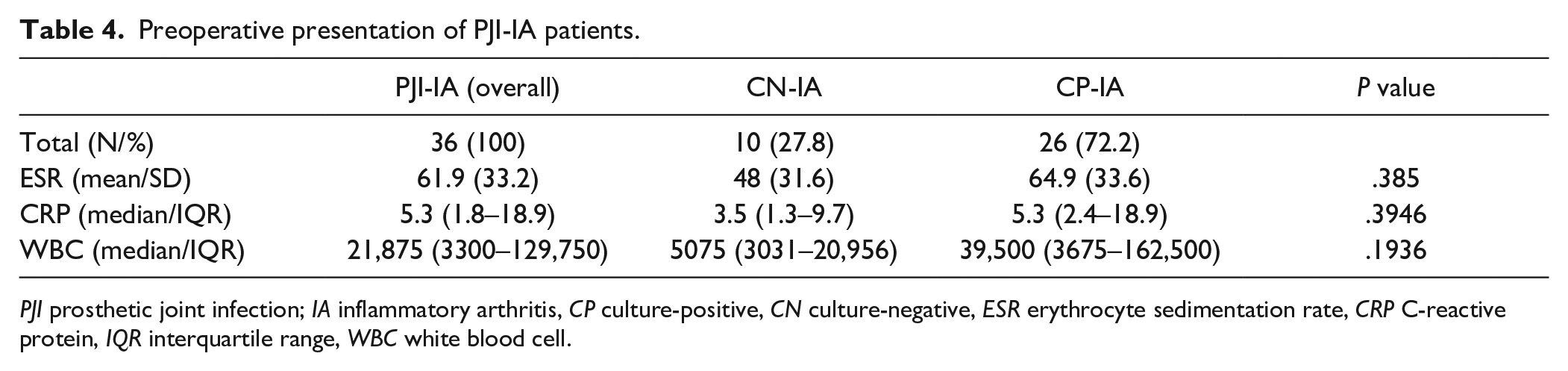
PJI prosthetic joint infection; IA inflammatory arthritis, CP culture-positive, CN culture-negative, ESR erythrocyte sedimentation rate, CRP C-reactive protein, IQR interquartile range, WBC white blood cell.
An example of chronic inflammation in IA-CN case (a), demonstrating heavy perivascular chronic inflammation, including numerous plasma cells (arrows). PMNs are above the threshold in a few fields (b), but do not meet the 5 fields’ cutoff. 200× magnification. Bar = 50 µm. IA-CN, inflammatory arthritis and culture-negative, PMN polymorphonuclear leucocyte.
Discussion
To our knowledge, this is the first study that compares the histopathology of IA-CP with that of IA-CN. In this retrospective study, we found that, within a 9-year period, 5% of our PJI cases were patients with IA and that those with RA or SLE had a significantly higher rate of CN cases compared with patients with OA (P < .02). Fewer IA-CN cases met MSIS criteria for PJI compared with OA-CN cases (IA-CN 50% vs OA-CN 71%). Of those who did not meet MSIS criteria, 25% within the IA-CN cohort had PMN infiltrates defining PJI. Histopathology of surgical specimens revealed differences between the IA-CN and the OA-CN cohorts. For example, 75% of the IA-CN group did not have PMN infiltrates defined as PJI on histopathology. However, for OA, there was no significant difference in histopathology findings of PMN infiltrates defined as PJI between OA-CP and OA-CN.
Furthermore, 50% of the IA cases did not meet MSIS criteria for infection, although all were treated as a PJI. Our findings indicate that some IA-CN PJI may have alternate noninfectious diagnoses, including flares of underlying IA.
Our results add to the limited literature on PJI in patients with IA. Whereas patients with IA-CN who were diagnosed and treated for PJI without having met MSIS criteria may have been experiencing a flare rather than infection, other possibilities leading to a diagnosis of PJI without fulfilling MSIS criteria may include chronic PJI or antibiotic therapy before surgery [2,14]. A retrospective study by Berbari et al [1], looking at a cohort of 200 patients with RA and PJI, found that only 9% were CN and RA was not an independent risk factor for CN PJI. In another retrospective analysis by Hseih et al [8], of 46 RA patients with PJI, none were CN. Schrama et al [21] report a 37% CN rate in 49 RA patients, a high percentage that they attribute to possible prior antimicrobial therapy. All of these studies lack histopathological analysis; thus, our study adds to the limited and conflicting studies available and provides evidence of a statistically significant higher rate of CN PJI in the IA group (27.8%) than the OA group (14.1%), while identifying differences in histopathology. The challenge of diagnosing PJI in patients with IA underscores the importance of future prospective studies for assessing PJI in these patients, especially if MSIS criteria are not present.
The incidence of PJI among patients with RA and other forms of IA is 50% to 80% greater than it is in patients with OA [24]. This may be attributed to the immunosuppressive agents prescribed to patients with RA, which include glucocorticoids and DMARDs. In this retrospective review, 75% of the IA-CN group did not have PMN infiltrates diagnostic of PJI on histopathology and 50% did not meet MSIS criteria for infection, although all were treated as a PJI by infectious disease and orthopedic specialists. A histological diagnosis is very important in the assessment of possible PJI as it forms part of the minor MSIS diagnostic criteria at a threshold of 5 PMNs per HPF [16]. A study of prosthetic knee infection concluded that knee PJI was more often confirmed by MSIS histological than microbiological criteria; thus, histology aids in distinguishing between aseptic and septic cases [9]. The AAOS recognizes that 5 PMN per HPF confers a likelihood ratio of 13.82 (7.29, 26.19); however, 10 PMN/HPF in 5 fields confers a likelihood ratio of 56.5 (20.3, 157.2) [15]. Given the high sensitivity and specificity of histopathology for PJI, it is important to note that 75% of IA-CN patients did not have positive histology and 63% had signs of lymphoplasmacytic chronic inflammation, a pattern that is classically seen in established RA, rather than in an infective process [7]. In patients with RA, the usefulness of histology for predicting infection remains unclear. Research suggests that, whereas RA can be a cause of false-positive histology for the diagnosis of PJI during hip or knee revision, using a combination of clinical and laboratory diagnostic markers, including cultures, fistula formation, ESR, and CRP level as reference, allows for strong consideration of a negative histological result [13].
As previously mentioned, a major limitation of this study is that half of our IA-CN cohort did not meet MSIS criteria for PJI but were included in the database because they were treated for PJI by the attending orthopedist and an infectious disease specialist. This indicates that differentiating between a septic joint and an IA flare is challenging in patients presenting with an acutely inflamed prosthetic joint. Standard diagnostic tests (such as levels of serum and synovial white blood cell counts) and biomarkers (such as ESR, CRP, leukocyte esterase, or alpha-defensin) may be similar in both and therefore may be misleading in the diagnostic process. In a systematic review on the efficacy of synovial biomarkers for diagnosing PJI in patients with IA, Mirza et al [12] found that, whereas the sensitivities are high for many serum and synovial tests, specificities in this patient population are low. They showed that although levels of synovial white blood cells, interleukin (IL)-6, IL-8, and serum CRP are elevated in infected patients with IA, there is overlap with those who are not infected. The poor specificity of standard diagnostic tests contributes to the notion that a proportion of IA patients are not infected but are flaring.
Importantly, cases are included in the database through diagnosis and treatment by an attending orthopedist and infectious disease specialist with expertise in the diagnosis and therapy of PJI, and not all cases meet MSIS criteria for PJI. Evaluation of a patient’s clinical symptoms, medical history, and comprehensive physical examination guides diagnostic strategy and screening for PJI, as in the presence of erythema and swelling about the joint associated with systemic symptoms. Moreover, the urgency of making a PJI diagnosis to optimize outcomes may contribute to incorrect diagnosis. As Kim and Cho have summarized, many factors affect the clinical presentation of PJI, including “the virulence of the etiological agent involved, the nature of the infected tissue, the infection acquisition route, and the duration of disease evolution” [10, 11].
However, we were intrigued by the high proportion of patients with IA-CN in this small retrospective cohort and, given the overlap in available diagnostic tests, found support for the idea that some IA patients treated for PJI may, in fact, have flares of IA. A larger, more detailed prospective study is warranted to further study patients with IA-CN who receive a presumptive diagnosis of PJI. New technologies, such as next-generation sequencing, hold promise as a useful adjunct in the identification of an organism in CN PJI and may provide increased sensitivity in isolating organisms that cannot be identified using conventional culture [22, 23].
Our study highlights a clinical issue relevant to patients with IA with a single inflamed joint after arthroplasty. Standard diagnostic criteria do not clearly apply to this patient population, and scant data are available to guide clinicians. It remains challenging to manage these patients, particularly those with negative cultures. This preliminary work supports the need for further studies to assess the differences in clinical features between CN and CP PJI in patients with IA and the ability of biological diagnostic markers to discriminate between them in this population. A robust PJI diagnostic algorithm specifically for IA patients is needed to ensure rapid and accurate diagnosis and optimize outcomes.
Supplemental Material
sj-docx-1-hss-10.1177_15563316231153395 – Supplemental material for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis
Supplemental material, sj-docx-1-hss-10.1177_15563316231153395 for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis by Peter Sculco, Milan Kapadia, Carine J. Moezinia, Insa Mannstadt, Andy O. Miller, Laura Donlin, Michael Henry, Linda Russell, Mark Figgie, Allina Nocon, Tania Pannellini and Susan M. Goodman in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-10-hss-10.1177_15563316231153395 – Supplemental material for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis
Supplemental material, sj-docx-10-hss-10.1177_15563316231153395 for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis by Peter Sculco, Milan Kapadia, Carine J. Moezinia, Insa Mannstadt, Andy O. Miller, Laura Donlin, Michael Henry, Linda Russell, Mark Figgie, Allina Nocon, Tania Pannellini and Susan M. Goodman in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-11-hss-10.1177_15563316231153395 – Supplemental material for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis
Supplemental material, sj-docx-11-hss-10.1177_15563316231153395 for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis by Peter Sculco, Milan Kapadia, Carine J. Moezinia, Insa Mannstadt, Andy O. Miller, Laura Donlin, Michael Henry, Linda Russell, Mark Figgie, Allina Nocon, Tania Pannellini and Susan M. Goodman in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-12-hss-10.1177_15563316231153395 – Supplemental material for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis
Supplemental material, sj-docx-12-hss-10.1177_15563316231153395 for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis by Peter Sculco, Milan Kapadia, Carine J. Moezinia, Insa Mannstadt, Andy O. Miller, Laura Donlin, Michael Henry, Linda Russell, Mark Figgie, Allina Nocon, Tania Pannellini and Susan M. Goodman in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-2-hss-10.1177_15563316231153395 – Supplemental material for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis
Supplemental material, sj-docx-2-hss-10.1177_15563316231153395 for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis by Peter Sculco, Milan Kapadia, Carine J. Moezinia, Insa Mannstadt, Andy O. Miller, Laura Donlin, Michael Henry, Linda Russell, Mark Figgie, Allina Nocon, Tania Pannellini and Susan M. Goodman in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-3-hss-10.1177_15563316231153395 – Supplemental material for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis
Supplemental material, sj-docx-3-hss-10.1177_15563316231153395 for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis by Peter Sculco, Milan Kapadia, Carine J. Moezinia, Insa Mannstadt, Andy O. Miller, Laura Donlin, Michael Henry, Linda Russell, Mark Figgie, Allina Nocon, Tania Pannellini and Susan M. Goodman in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-4-hss-10.1177_15563316231153395 – Supplemental material for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis
Supplemental material, sj-docx-4-hss-10.1177_15563316231153395 for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis by Peter Sculco, Milan Kapadia, Carine J. Moezinia, Insa Mannstadt, Andy O. Miller, Laura Donlin, Michael Henry, Linda Russell, Mark Figgie, Allina Nocon, Tania Pannellini and Susan M. Goodman in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-5-hss-10.1177_15563316231153395 – Supplemental material for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis
Supplemental material, sj-docx-5-hss-10.1177_15563316231153395 for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis by Peter Sculco, Milan Kapadia, Carine J. Moezinia, Insa Mannstadt, Andy O. Miller, Laura Donlin, Michael Henry, Linda Russell, Mark Figgie, Allina Nocon, Tania Pannellini and Susan M. Goodman in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-6-hss-10.1177_15563316231153395 – Supplemental material for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis
Supplemental material, sj-docx-6-hss-10.1177_15563316231153395 for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis by Peter Sculco, Milan Kapadia, Carine J. Moezinia, Insa Mannstadt, Andy O. Miller, Laura Donlin, Michael Henry, Linda Russell, Mark Figgie, Allina Nocon, Tania Pannellini and Susan M. Goodman in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-7-hss-10.1177_15563316231153395 – Supplemental material for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis
Supplemental material, sj-docx-7-hss-10.1177_15563316231153395 for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis by Peter Sculco, Milan Kapadia, Carine J. Moezinia, Insa Mannstadt, Andy O. Miller, Laura Donlin, Michael Henry, Linda Russell, Mark Figgie, Allina Nocon, Tania Pannellini and Susan M. Goodman in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-8-hss-10.1177_15563316231153395 – Supplemental material for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis
Supplemental material, sj-docx-8-hss-10.1177_15563316231153395 for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis by Peter Sculco, Milan Kapadia, Carine J. Moezinia, Insa Mannstadt, Andy O. Miller, Laura Donlin, Michael Henry, Linda Russell, Mark Figgie, Allina Nocon, Tania Pannellini and Susan M. Goodman in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Supplemental Material
sj-docx-9-hss-10.1177_15563316231153395 – Supplemental material for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis
Supplemental material, sj-docx-9-hss-10.1177_15563316231153395 for Clinical and Histological Features of Prosthetic Joint Infections May Differ in Patients With Inflammatory Arthritis and Osteoarthritis by Peter Sculco, Milan Kapadia, Carine J. Moezinia, Insa Mannstadt, Andy O. Miller, Laura Donlin, Michael Henry, Linda Russell, Mark Figgie, Allina Nocon, Tania Pannellini and Susan M. Goodman in HSS Journal®: The Musculoskeletal Journal of Hospital for Special Surgery
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Peter Sculco, MD, reports relationships with EOS Imaging, Intellijoint Surgical, and Lima Corporate. Laura Donlin, PhD, reports relationships with Karius, Inc, and Stryker. Linda Russell, MD, reports a relationship with the Arthritis Foundation. Mark Figgie, MD, reports relationships with HS2, Insight, Lima, Mekanika, and Wishbone. Susan M Goodman, MD, reports relationships with Novartis and UCB. The other authors declare no potential conflicts of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human/Animal Rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2013.
Informed Consent
Informed consent was waived from all patients whose data were included in this study.
Level of Evidence
Level III, retrospective prognostic study.
Required Author Forms
Disclosure forms provided by the authors are available with the online version of this article as supplemental material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.