
Abstract
Purpose:
Classification of femoral trochanteric fractures is usually based on plain X-ray findings using the Evans, Jensen, or AO/OTA classification. However, complications such as nonunion and cut out of the lag screw or blade are seen even in stable fracture. This may be due to the difficulty of exact diagnosis of fracture pattern in plain X-ray. Computed tomography (CT) may provide more information about the fracture pattern, but such data are scarce. In the present study, it was performed to propose a classification system for femoral trochanteric fractures using three-dimensional CT (3D-CT) and investigate the relationship between this classification and conventional plain X-ray classification.
Methods:
Using three-dimensional (3D)-CT, fractures were classified as two, three, or four parts using combinations of the head, greater trochanter, lesser trochanter, and shaft. We identified five subgroups of three-part fractures according to the fracture pattern involving the greater and lesser trochanters. In total, 239 femoral trochanteric fractures (45 men, 194 women; average age, 84.4 years) treated in four hospitals were classified using our 3D-CT classification. The relationship between this 3D-CT classification and the AO/OTA, Evans, and Jensen X-ray classifications was investigated.
Results:
In the 3D-CT classification, many fractures exhibited a large oblique fragment of the greater trochanter including the lesser trochanter. This fracture type was recognized as unstable in the 3D-CT classification but was often classified as stable in each X-ray classification.
Conclusions:
It is difficult to evaluate fracture patterns involving the greater trochanter, especially large oblique fragments including the lesser trochanter, using plain X-rays. The 3D-CT shows the fracture line very clearly, making it easy to classify the fracture pattern.
Introduction
The incidence of femoral trochanteric fractures is rapidly increasing with the growth of the elderly population. Classification of femoral trochanteric fractures is usually based on plain X-ray findings 1 using systems such as the Evans classification, 2 Jensen classification, 3 and AO/OTA classification. 4 However, complications such as delayed union, nonunion, malunion, and cut out of the lag screw or blade are sometimes seen in fractures classified using X-rays, even in stable fractures. 5,6 These complications are partly caused by technical problems associated with surgery. Another factor that may hinder diagnosis is a misunderstanding of the fracture pattern by plain X-rays because femoral trochanteric fractures are sometimes very difficult to precisely diagnose, especially those involving the trochanteric fragment. Computed tomography (CT) may provide more information about the fracture pattern, especially in the trochanteric area; however, no fracture classification systems using CT have been established.
The first objective of this study was to propose a classification of femoral trochanteric fractures using three-dimensional CT (3D-CT). The second objective was to investigate the relationship between this classification and conventional plain X-ray classification.
Materials and methods
The 3D-CT classification was based on the combination of four major fragments: the head (H), greater trochanter (G), lesser trochanter (L), and shaft (S) (Figure 1). Each fracture was classified as a two-, three-, or four-part fracture according to the classification reported by Nakano 7 in Japan. A schema of our 3D-CT classification is shown in Figure 2 and actual images of 3D-CT of each type are shown in Figure 3.

Fracture is classified using a combination of four major fragments. (a): anterior aspect; (b): posterior aspect; H: head; G: greater trochanter; L: lesser trochanter; S: shaft. three-dimensional computed tomography (3D-CT) classification is also based on the combination of four major fragments.
Fracture classification with three-dimensional computed tomography (3D-CT). Three-part fracture is divided into five subgroups.

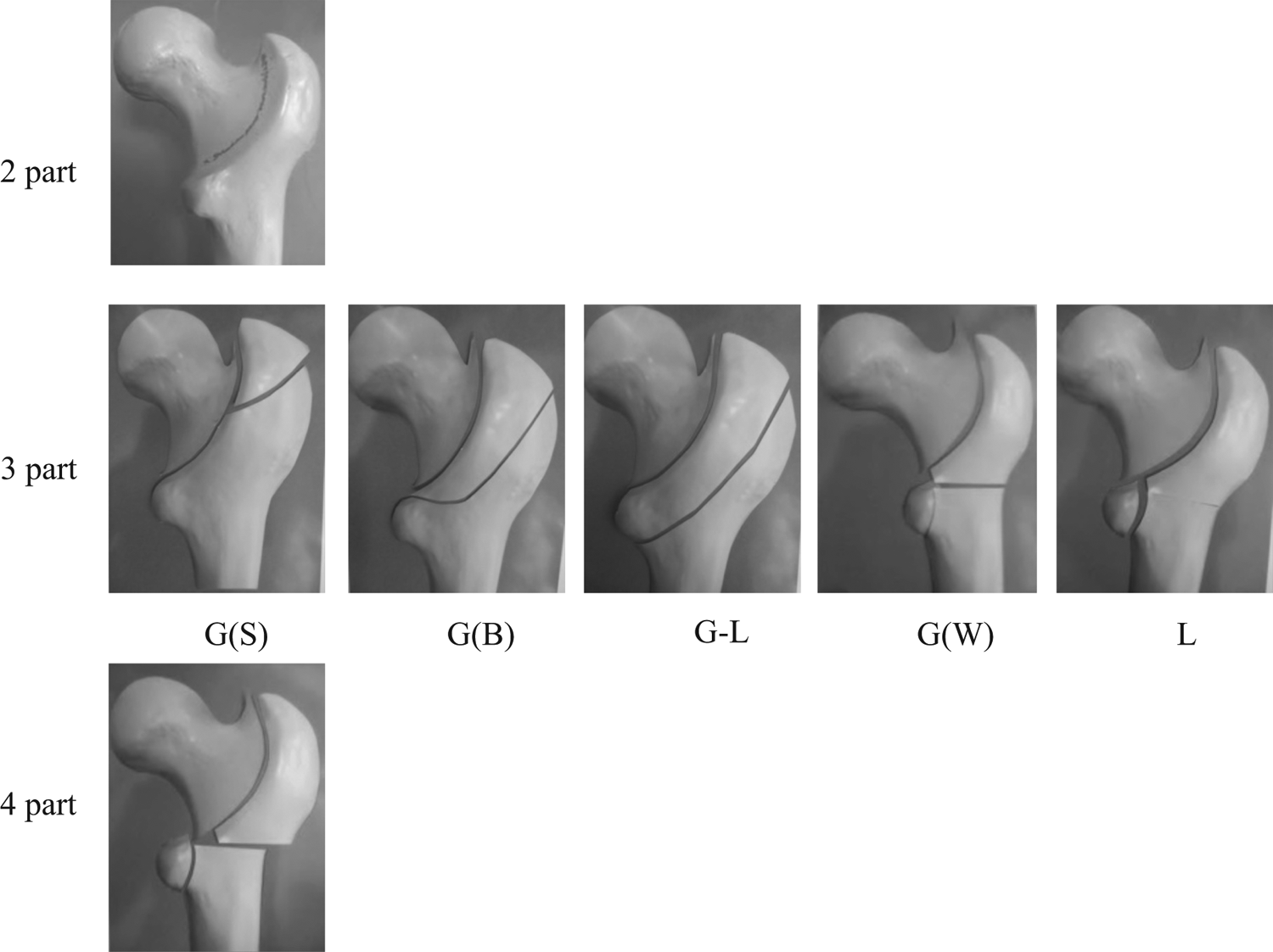
Actual images of three-dimensional computed tomography (3D-CT) in each group.
A two-part fracture is a simple fracture, similar to an Evans type 1, group 1 fracture; the anterior fracture line is on the intertrochanteric line, the posterior fracture line is in the intertrochanteric fossa, and the lesser trochanter is intact. In a four-part fracture, both the greater trochanter and lesser trochanter are fractured and displaced. Such fractures are consistent with an Evans type 1, group 4 fracture or Jensen type 5 fracture.
In this study, we identified five subgroups of three-part fractures according to the fracture pattern of the greater and lesser trochanters. The first subgroup involved a small fragment of the greater trochanter in addition to a two-part fracture: 3-part G(S), where S indicates small. The second subgroup involved a big oblique fragment of the greater trochanter that does not include the lesser trochanter: 3-part G(B), where B indicates big. The third subgroup involves a large oblique fragment of the greater trochanter including the lesser trochanter: 3-part G-L. In this type, the large trochanteric fragment is sometimes divided into two fragments between the greater and lesser trochanter. The fourth subgroup involves a fragment of the whole greater trochanter, but the lesser trochanter is intact: 3-part G(W), where W indicates whole. This type includes some Evans type 2 fractures and AO/OTA A-3 fractures. Finally, the fifth subgroup comprises fractures of the lesser trochanter in addition to two-part fractures: 3-part L. These fractures do not involve the greater trochanter.
According to the classification described by Nakano, 7 2-part, 3-part G(S), and 3-part G(B) fractures are considered stable and 3-part G-L, 3-part G(W), 3-part L, and 4-part fractures are considered unstable.
In total, 239 femoral trochanteric fractures (45 men, 194 women; average age 84.4 years) treated with the Asian proximal femur intramedullary nail antirotation system: PFNA-II (DePuy Synthes Trauma, PA, USA) from April 1, 2011, to December 31, 2014, in four hospitals were investigated and classified with this 3D-CT classification. Each fracture was also classified by the AO/OTA, Evans, and Jensen classifications. First author, one orthopedic specialist and two residents classified these fractures. The relationship between each of these classifications and our 3D-CT classification was investigated.
Results
Using our 3D-CT classification, the numbers of each fracture type were as follows: 2-part, n = 49; 3-part G(S), n = 30; 3-part G(B), n = 37; 3-part G-L, n = 82; 3-part G(W), n = 17; 3-part L, n = 8; and 4-part, n = 16 (Table 1). We identified 116 stable fractures in the 3D-CT classification (2-part, 3-part G(S), and 3-part G(B)) and 123 unstable fractures (3-part G-L, 3-part G(W), 3-part L, and 4-part). The relationship between the 3D-CT classification and the AO/OTA, Evans, and Jensen classifications is shown in Tables 2, 3, and 4. Fifty (41%) of 123 unstable fractures in the 3D-CT classification were classified as stable in the AO/OTA classification (Table 2). Forty-four (88%) of these 50 fractures were of the 3-part G-L type. Additionally, 87 (71%) of 123 unstable fractures according to the 3D-CT classification were classified as stable in the Evans classification (76 were 3-part G-L fracture: 87%) (Table 3), and 47 (38%) of 123 unstable fractures according to the 3D-CT classification were classified as stable in the Jensen classification (40 were 3-part G-L fracture: 85%) (Table 4). Almost all mismatched fractures between the 3D-CT and X-ray classifications (unstable in 3D-CT, stable in X-ray) were 3-part G-L fracture (AO/OTA: 88%, Evans: 87%, Jensen: 85%). Conversely, only 1 of 116 stable fractures according to the 3D-CT classification was classified as unstable in the AO/OTA classification. Similarly, one fracture was unstable in the Evans classification and six were unstable in the Jensen classification.
Numbers of each type of fracture.a
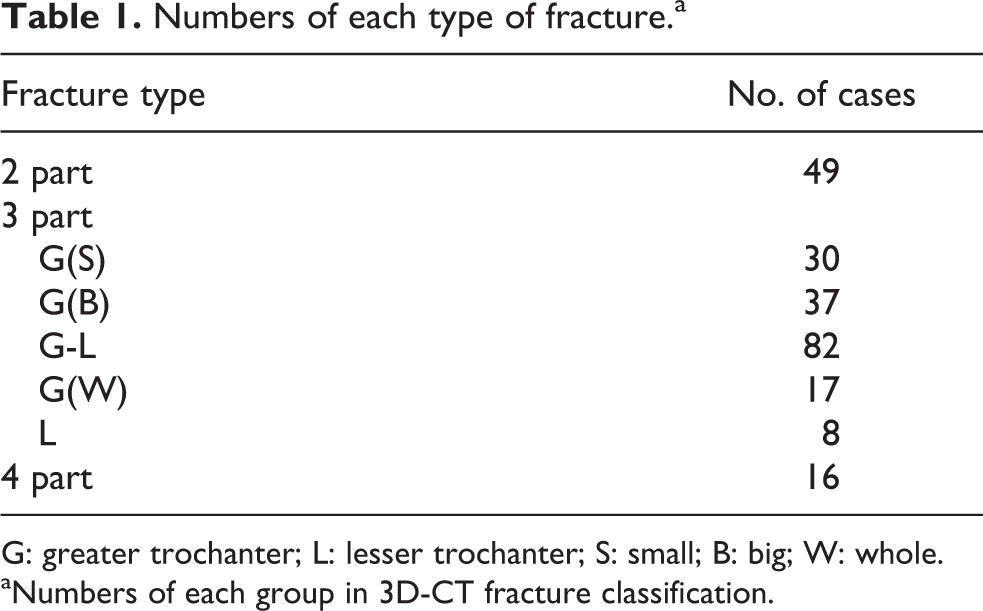
G: greater trochanter; L: lesser trochanter; S: small; B: big; W: whole.
aNumbers of each group in 3D-CT fracture classification.
Relationship between three-dimensional computed tomography (3D-CT) classification and AO/OTA classification.a
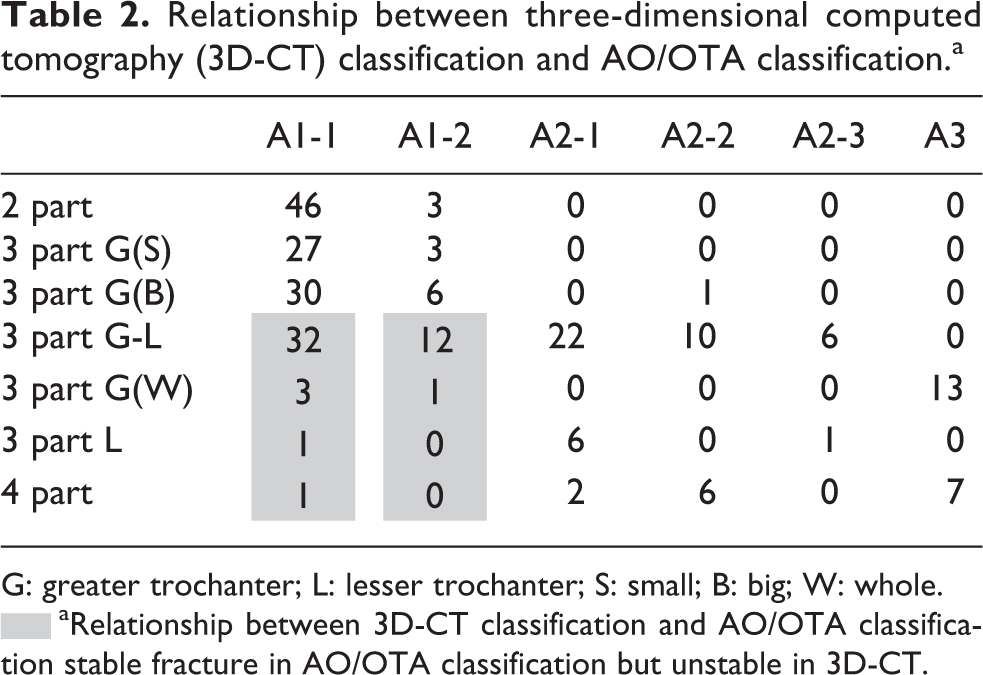
G: greater trochanter; L: lesser trochanter; S: small; B: big; W: whole.
▪aRelationship between 3D-CT classification and AO/OTA classification stable fracture in AO/OTA classification but unstable in 3D-CT.
Relationship between three-dimensional computed tomography (3D-CT) classification and Evans classification.a

G: greater trochanter; L: lesser trochanter; S: small; B: big; W: whole.
▪aRelationship between 3D-CT classification and Evans classification stable fracture in Evans classification, but unstable in 3D-CT.
Relationship between 3D-CT classification and Jensen classification.a

G: greater trochanter; L: lesser trochanter; S: small; B: big; W: whole.
▪aRelationship between 3D-CT classification and Jensen classification stable fracture in Jensen classification but unstable in 3D-CT.
Discussion
Several plain X-ray-based classification systems for femoral trochanteric fractures are available. The Evans, Jensen, and AO/OTA classifications have been widely used in clinical practice. In 1949, Evans 2 developed a classification system based on the direction of the fracture line and the assessment of stability, determined according to the likelihood of fracture reduction and displacement. In 1980, Jensen 3 added evaluation of plain lateral X-rays to this classification system. Finally, the AO/OTA classification system 4 was introduced. These classification systems have been used for treatment planning and outcome prediction. In each classification system, fractures are mainly divided into two groups: stable or unstable. In the Evans classification, groups 1 and 2 of type 1 fractures are stable, and others are unstable. In the Jensen classification, types 1 and 2 are stable and types 3, 4, and 5 are unstable. In the AO/OTA classification, type 31-A1 is stable and types A2 and A3 are unstable. However, complications including delayed union, nonunion, malunion, and cut out of the lag screw or blade are sometimes seen on plain X-rays, even in stable fractures. This may make it difficult to distinguish stable versus unstable fractures on plain X-rays. CT may provide more information about the fracture pattern, especially in the trochanteric area.
CT is usually used for femoral neck fractures or for diagnosis of occult fractures of the proximal femur. 8,9 However, there are only a few reports of CT for evaluation of femoral trochanteric fractures. 10,11 Nakano 7 proposed a 3D-CT classification system in Japan. Our classification is a modification of his classification. In his classification, two-part fractures are the most stable, and four-part and type II (reverse oblique type) are the most unstable. Nakano also pointed out that many fractures have a large oblique fragment that includes the lesser trochanter on 3D-CT (our 3-part G-L fracture) and this type is equally as unstable as a four-part or type 2 fracture.
Unstable trochanteric fractures may exhibit (1) posteromedial large separate fragmentation, (2) a basicervical pattern, (3) a reverse obliquity pattern, (4) a displaced greater trochanter (lateral wall fracture), or (5) the inability to be reduced before internal fixation. Of the above characteristics, 3-part G-L type fracture is considered to have posteromedial large separate fragmentation. So 3-part G-L type is recognized as unstable type because of this definition and Nakano’s article. However, classification of this fracture is impossible using plain X-rays. In the present study, 50, 87, and 47 fractures that were classified as stable using the AO/OTA (41%), Evans (71%), and Jensen classifications (38%) were classified as unstable using the 3D-CT classification. Additionally, almost all fractures in each group were 3-part G-L fractures using 3D-CT (AO/OTA: 88%, Evans: 87%, Jensen: 85%). This result shows that 3-part G-L fractures tend to be misdiagnosed as stable fractures on plain X-rays. However, there is no study on how to manage this fragment.
Overall, our findings indicate that it is very difficult to evaluate the fracture pattern of the greater trochanter on plain X-rays and that our 3D-CT classification system may be necessary for more precise diagnosis of trochanteric fractures. There is no clinical results relation to this 3D-CT classification in this article. Another study on how to treat this fragment and clinical investigation based on this classification is necessary in next stage. However, whether this classification system has acceptable reliability when applied by all orthopedic surgeons remains to be determined, because intra- and interobserver variations are not measured in this study.
After solution of these problems, this 3D-CT classification should be one of the treatment guidelines.
Conclusion
3D-CT classification system for femoral trochanteric fractures has been proposed in this study. This study has shown that it is difficult to evaluate the fracture pattern of the greater trochanter, especially large oblique fragments that include the lesser trochanter, on plain X-rays. 3D-CT shows the fracture line very clearly, making it easy to classify the fracture pattern.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was supported by AOTAP Research Seed Grants 2010.
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics statement
This project was approved by the ethical committee of Hyogo Prefectural Nishinomiya Hospital.