
Abstract
Purpose:
The objective of this study is to assess artifact reduction and image quality using dual-energy computed tomography (DECT) and metal artifact reduction techniques in patients with metallic implants.
Methods:
Forty patients with metallic implants, who had targeted CT performed by DECT during March to September 2018, were prospectively recruited. Post-processing with monoenergetic extrapolation at 70 and 150 keV was performed. Forty matched controls with metallic implants with single-energy CT (SECT) performed were selected. Attenuation value, noise, and signal-to-noise ratio (SNR) at the site of maximal artifact were measured at muscle and fat areas. Image quality of three sets of images (70 keV, 150 keV, and SECT) was assessed by two independent reviewers using a 5-point Likert-type scale. Statistical analysis of measured values, Likert-type scales, and radiation doses (volume CT dose index (CTDIvol)) of DECT and SECT were performed with Mann–Whitney U test.
Results:
As compared to SECT, high keV reconstruction of DECT show (1) significantly higher values within muscle and fat surrounding the implant (DECT vs. SECT—muscle: −96 Hounsfield units (HU) vs. −405 HU, fat: −115 HU vs. −301 HU; p < 0.001), (2) significantly lower mean image noise (75 HU vs. 129 HU; p = 0.02), and (3) higher SNR (−0.8 vs. −4.3; p < 0.001). In addition, image quality of high keV reconstruction was rated superior to the other two groups on Likert-type scales (p < 0.001). The mean radiation doses (CTDIvol) were comparable between DECT and SECT (14.2 mGy vs. 19.3 mGy; p = 0.08).
Conclusion:
For patients with metallic implants, monoenergetic extrapolation of DECT at high keV can reduce metal artifacts, increase SNR, and improve qualitative image quality at comparable radiation dose.
Introduction
Computed tomography (CT) is commonly performed for postoperative evaluation in orthopedic patients with metallic prosthesis or osteosynthetic material. 1 CT is desirable for the evaluation of the implant integrity and alignment and the surrounding soft tissue for postoperative complications such as fluid collections. 2 However, metallic artifacts as a result of implanted orthopedic devices impose a significant diagnostic challenge in this group of patients.
Metallic artifact consists of two main components, which are photon starvation and beam hardening effects. These effects can be theoretically reduced by higher energy photons. 3,4 Hence, conventional metallic artifact reduction techniques often rely on altering scanning parameters such as increasing tube current and peak kilovoltage, which come at the cost of increasing radiation dose to patients. 3,5
Dual-energy CT (DECT) is a relatively new technology in clinical CT application. It uses two beams at lower and higher tube voltages, typically at 80 and 140 kVp. 5 The atomic number and attenuation difference between the low- and high-energy beams give rise to unique spectral properties and dual-energy index for different materials. 6 –8 Current clinical applications of DECT include generation of material-specific images, such as material decomposition within renal stones, virtual unenhanced imaging, and automated bone removal. 6,7,9 Another important usage of DECT is the ability to perform synthetic monoenergetic extrapolation, which uses the change in attenuation between 80 kVp and 140 kVp to extrapolate and generate monochromatic images with discrete photon energy from 40 keV to 190 keV . 5,9,10 Hence, theoretical high keV image can be achieved without increasing the actual tube voltage and patient radiation dose.
In the current literature, evidence has shown that DECT has the advantage of reducing metallic artifacts compared to single-energy CT (SECT). 3,5 There are also existing studies that compared the different incremental values in monoenergetic extrapolation in terms of volume of artifacts. 10 However, evidence is lacking in a direct comparison between different monochromatic images with different photon energies on DECT and SECT in terms of diagnostic performance and radiation dosage.
Since DECT is a rather new technique, our study aims to evaluate whether the use of DECT with different energy levels in monoenergetic extrapolation can provide CT images with lower metallic artifacts, lower noise, and better image quality in orthopedic patients with metallic prosthesis or osteosynthetic material.
Methods
Patient population
The study was approved by the ethics committee of our institution. Our inclusion criteria include all subjects with metallic implants, who had targeted plain DECT performed in our department during March to September 2018. All patients were prospectively recruited after CT scan referral by the Orthopedics department. The exclusion criteria were patients under the age of 18 years. A matched number of controls with metallic implants who had conventional SECT performed at the same targeted body regions were retrospectively selected and compared. All patients included in both the study and control groups had metallic implants consisted of stainless steel or titanium alloy. All CT examinations were requested with clinical indications, and no CT was performed merely for study purpose.
CT image acquisition and reconstruction
All CT examinations were performed on Siemens SOMATOM Definition Flash CT (Siemens Medical, Forchheim, Germany) at Pamela Youde Nethersole Eastern Hospital. For the DECT protocol, 140 and 80 kVp were performed with standard tube current (mAs) and pitch values according to the different body regions (Table 1). The beam collimation was 128 × 0.6 mm2. Images were reviewed on a Syngo Dual Energy Software in a three-dimensional (3-D) image workstation (Syngo.Via Client 2.0, Siemens HealthCare, Erlangen, Germany). Monoenergetic application with extrapolation of low photon energy (70 keV) and high photon energy (150 keV) was performed.
Dual-energy CT protocol used in Siemens SOMATOM definition flash CT.
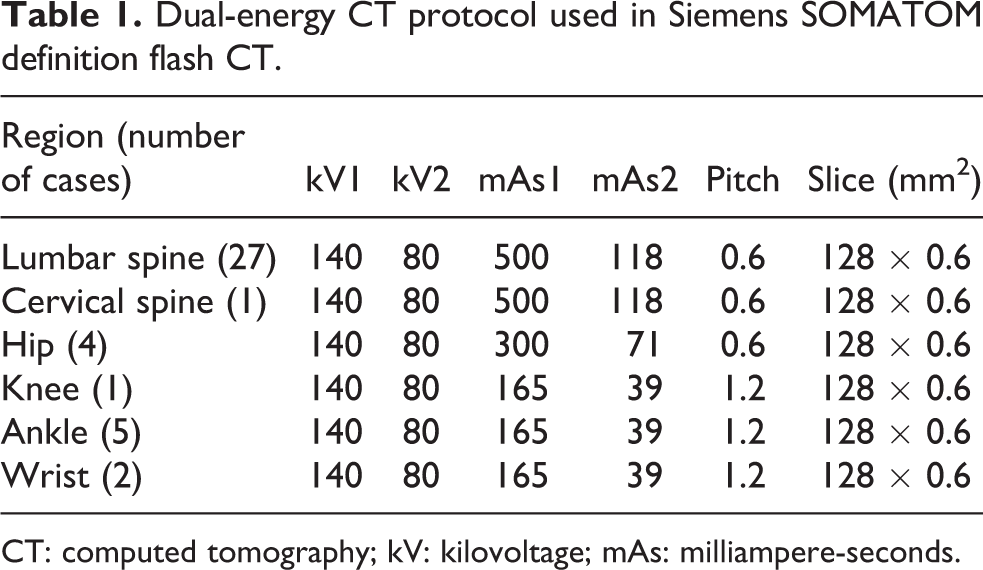
CT: computed tomography; kV: kilovoltage; mAs: milliampere-seconds.
For the control group with conventional SECT performed, tube voltage of 120 kVp and automatic exposure control for tube current modulation were used. The pitch and beam collimation were the same as those in the DECT protocol. No specific post-processing was performed after image acquisition. The images were reviewed on the same 3-D image workstation as those with DECT performed.
Quantitative image analysis
To quantitatively assess the metallic artifacts produced by the implants on CT, the mean attenuation values, image noises, and signal-to-noise ratios (SNRs) were assessed in all three sets of images, including the DECT in 150 and 70 keV reconstructions and SECT. The image plane which the artifact was most pronounced was assessed. The mean attenuation values in Hounsfield units (HU) within the adjacent muscle and fat were measured by drawing regions of interest (ROIs) along the most hypodense streak by a standardized manner as shown in Figure 1. The ROIs in the muscle were placed at 1 cm from the edge of the implant. The ROIs in the fat were placed at 1 cm from the fat and muscle interface. Each ROI was limited to an area of 0.2 cm. 2 The mean image noise was defined as the standard deviation (SD) of HU within the same ROI. The SNR was defined as mean HU divided by image noise as measured in the ROI.
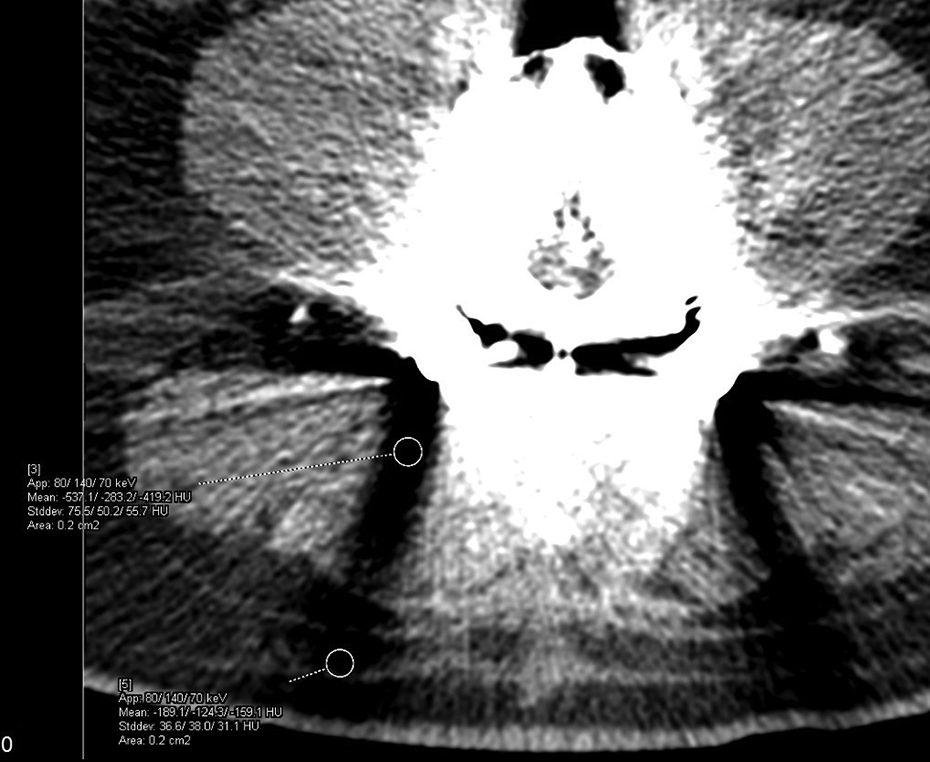
CT lumbosacral spine performed with dual-energy CT protocol. ROIs drawn at the surrounding muscle and fat along the most hypodense streak produced by the metallic implant. Mean attenuation values and image noise (standard deviation) within the muscle and fat are obtained from the ROIs. CT: computed tomography; ROI: region of interest.
Qualitative image analysis
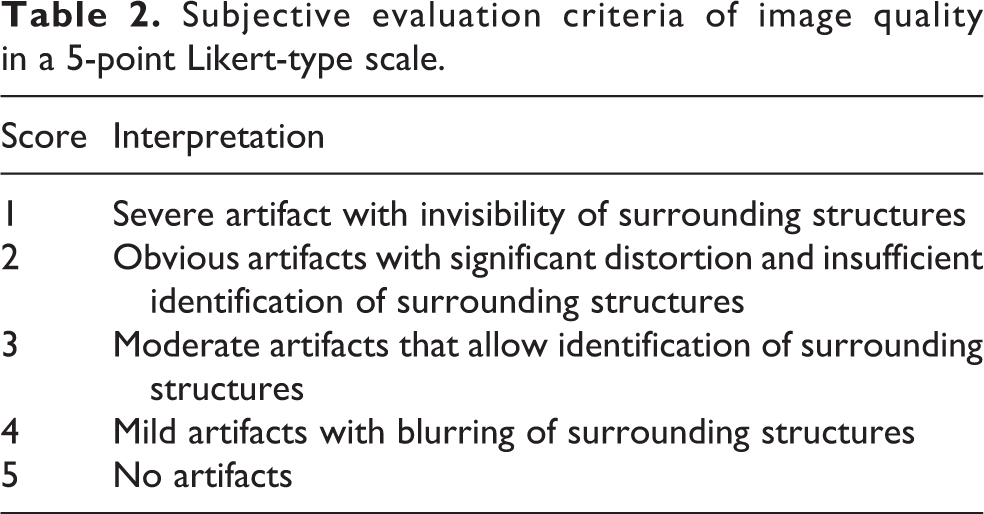
Subjective image quality was assessed by two independent radiologists with 3 and 6 years of experience in musculoskeletal radiology, respectively. All three sets of images were evaluated in the same soft tissue window settings (window width: 350 HU, center: 40 HU). The degree of artifact and diagnostic interpretability were evaluated using a 5-point Likert-type scale (Table 2).
Subjective evaluation criteria of image quality in a 5-point Likert-type scale.
Radiation dose measurement
Radiation dose measurements were obtained from our picture archiving and communication system, which were compared in terms of volume CT dose index (CTDIvol).
Statistical analysis
Descriptive statistics are expressed in mean ± SD. Statistical analysis of the measured values (including mean attenuation value, image noise, and SNR), Likert-type scales, and radiation doses of DECT and SECT was performed with Mann–Whitney U test. All statistical analyses were performed by statistics software (SPSS, version 25, IBM Software). Statistical significance was defined as p < 0.05.
Results
Patient demographics
A total of 40 patients with metallic implants (male (M):female (F) = 17:23) and a mean age of 66.3 years (range 27–89 years) had targeted CT performed by DECT protocol in our department during March to September 2018. There were a total of 6 scanned regions, which include the lumbosacral spine (27 cases), cervical spine (1 case), hip (4 cases), knee (1 case), ankle (5 cases), and wrist (2 cases). All patients included had metallic implants consisted of stainless steel or titanium alloy.
Forty controls (M:F = 16:24) with a mean age of 67.5 years (range 35–92 years) who had SECT performed in our department were retrospectively selected from May to December 2017, matching to the scanned regions of the study subjects. These patients also had metallic implants consisted of stainless steel or titanium alloy.
Quantitative image analysis
Assessment of metallic artifacts by mean attenuation values within muscle and fat at image plane with implant has shown significantly higher values in DECT high keV (150 keV) reconstruction compared to SECT. The mean HU within muscle in DECT and SECT were −96 and −405 HU, respectively (p < 0.001). The mean HU within fat in DECT and SECT were −115 and −301HU, respectively (p < 0.001) (Table 3). Significantly higher mean attenuation values were also noted in high keV (150 keV) compared to low keV (70 keV) reconstruction of DECT in the surrounding muscle and fat (both p < 0.001; Table 4).
Comparison of measured values between DECT high keV reconstruction (150 keV) and SECT.a

DECT: dual-energy CT; SECT: single-energy CT; CT: computed tomography; HU: Hounsfield units.
aData are shown as mean ± standard deviation. Statistically significant findings are indicated in italics.
Comparison of measured values between DECT high keV reconstruction (150 keV) and low keV reconstruction (70 keV).a

DECT: dual-energy CT; CT: computed tomography; HU: Hounsfield units.
aData are shown as mean ± standard deviation. Statistically significant findings are indicated in italics.
In terms of image noise, high keV (150 keV) reconstruction of DECT demonstrated a significantly lower noise level as compared to SECT (75 HU vs. 129 HU, p = 0.02) within the surrounding muscle. High keV reconstruction of DECT has also shown a lower mean image noise compared to SECT (51 HU vs. 89 HU, p = 0.089) within the surrounding fat despite not achieving statistical significance (Table 3). Statistically significant lower image noise is also seen with 70 keV as compared to SECT in the surrounding muscle and fat (58 HU vs. 129 HU, p < 0.001; 37 HU vs. 89 HU, p = 0.017, respectively; Table 5). No significant differences between image noise between 70 keV and 150 keV reconstructions are noted (p = 0.45 and p = 0.18 in muscle and fat, respectively; Table 4).
Comparison of measured values between DECT low keV reconstruction (70 keV) and SECT.a

DECT: dual-energy CT; SECT: single-energy CT; CT: computed tomography; HU = Hounsfield units.
aData are shown as mean ± standard deviation. Statistically significant findings are indicated in italics.
Significantly higher SNRs on the same image plane are seen in high keV reconstruction of DECT compared to SECT within both the surrounding muscle and fat (−0.8 vs. −4.3; p < 0.001, −3.1 vs. −19.1; p=0.03, respectively; Table 3). Significantly higher SNRs are also seen in high keV (150 keV) compared to low keV (70 keV) reconstruction in the surrounding muscle and fat (−0.8 vs. −7.1 and −3.1 vs. −13.9 in muscle and fat, respectively; both p < 0.001; Table 4).
Qualitative image analysis
Comparison of subjective image quality assessment for DECT high keV reconstruction (150 keV), low keV reconstruction (70 keV), and SECT is presented in Table 6. A significant improvement in image quality in terms of degree of artifact and diagnostic interpretability was noted comparing DECT high keV (150 keV) reconstruction to both SECT and DECT low keV (70 keV) reconstruction (p < 0.001). No significant difference in image quality is seen between DECT low keV (70 keV) reconstruction and SECT.
Results of subjective image quality assessment for DECT high keV reconstruction (150 keV), low keV reconstruction (70 keV), and SECT by a 5-point Likert-type scale.a

DECT: dual-energy CT; SECT: single-energy CT; SD: standard deviation; CT: computed tomography.
aData are shown as mean ± standard deviation. Statistically significant findings are indicated in italics.
Radiation dose measurement
Comparison of radiation dose between DECT and SECT was performed in terms of CTDIvol. DECT has shown a lower mean CTDIvol compared to SECT with no statistically significant difference noted between the two groups (14.2 ± 7.1 mGy vs. 19.3 ± 5.0 mGy; p = 0.08).
Discussion
In this study, we have provided evidence that metal artifacts can be significantly reduced with the use of high-energy monoenergetic extrapolation in DECT. Compared to conventional SECT, high-energy monoenergetic extrapolation in DECT allows improved diagnostic assessment of the implant. With reduced artifacts, the implant integrity and alignment can be better assessed (Figure 2). Moreover, improved detection of the peri-prosthetic complication such as fluid collection or hematoma can be achieved with decreased artifacts in the surrounding muscle and fat (Figure 3).

CT images of two patients with pedicle screws. (a) and (b) Conventional single-energy CT in soft tissue and bone windows, respectively. (c) to (f) Same set of CT images reconstructed in different energy levels. (c) and (d) Dual-energy CT in low energy (70 keV) reconstruction in soft tissue and bone windows, respectively. (e) and (f) Dual-energy CT in high-energy (150 keV) reconstruction in soft tissue and bone windows, respectively. Significant interval decrease in metallic artifacts and less obscuration of surrounding muscle and fat are seen in (e) and (f). The malposition of the left pedicle screw is clearly visualized. CT: computed tomography.

Axial DECT images with (a) 70-keV and (b) 150-keV reconstruction in soft tissue window of a patient with left hip unipolar arthroplasty. At 150 keV, reduced artifact and better appreciation of the collection at left gluteal region are noted. DECT: dual-energy computed tomography.
Metallic artifacts consist of two main components. The first being photon starvation effect, which is the full absorption of X-ray photons leading to zero transmission behind high attenuation area, particularly behind metal implants. The other component is beam hardening effect, which is the absorption of low-energy photons when polychromatic X-ray energy passes through an object. In theory, increasing the energy of the X-ray photons can reduce these effects. 3,4 Hence, conventional metallic artifact reduction techniques often rely on altering scanning parameters such as increasing tube current and peak kilovoltage, which come at a cost of increasing radiation dose to patients. 3,5,11
Synthetic monoenergetic extrapolation in DECT offers the ability to extrapolate and generate monochromatic images with discrete photon energy from 40 keV to 190 keV. 5,9,10 Hence, theoretical high keV image can be achieved without increasing actual tube voltage and patient dose. Lewis et al. had demonstrated the use of high keV monoenergetic reconstruction of DECT in successfully reducing metallic artifacts in phantoms of total hip replacements. 10 Analysis of reconstructed images at 10-keV intervals was performed between 40 keV and 190 keV. His study concluded that at 150 keV, the volume of streak artifact was the least with an increase in the overall artifact observed in higher energy level thereafter. 10 Hence, 150 keV was chosen as the level for higher keV reconstruction in our study.
In terms of background attenuation, different in vivo phantom and in vivo studies of monoenergetic extrapolation of DECT have demonstrated a lowest level of image noise at 70 keV. 10,12 –14 In our study, low keV (70 keV) reconstruction also demonstrates the lowest image noise compared to both high keV (150 keV) reconstruction and SECT. However, in terms of mean attenuation values at the site of greatest artifact, 150 keV have shown significantly higher values in the surrounding muscle and fat compared to both 70 keV and SECT. In addition, no statistically significant benefit can be observed in 70 keV compared to SECT. Hence, high keV (150 keV) reconstruction demonstrates the least effect from dark streak artifact on the surrounding tissue in a quantitative manner. In terms of SNR, high keV (150 keV) reconstruction demonstrates a statistically significant advantage compared to both SECT and low keV (70 keV) reconstruction within the surrounding muscle and fat.
Although DECT involves two energy levels during the examination, no statistical difference in radiation dose in terms of CTDIvol was observed compared to conventional SECT in our study. The main reason was the tube current selected tailored to each peak kilovoltage used (140 kVp and 80 kVp in our study) to ensure no excessive dose was administered compared to conventional SECT.
This study has several inherent limitations. First, the patient population was small with a heterogeneous distribution regarding anatomic location of the targeted CT performed for the site of implant. The small sample size also limited our ability to statistically analyze the effect of DECT on different sites of implants. Second, despite the use of metallic implant consisting of stainless steel or titanium alloy in patients of both the study and the control patient groups, the wide range of metallic implants being used did not allow an exact match between the study and the control subjects in terms of specific type of implant chosen for the operation. Further studies would be needed to address the metallic artifact on CT in each specific type of metallic implant. Furthermore, the two levels of keV reconstruction of DECT were used arbitrarily based on previous studies with no incremental levels studied in between. There are currently still controversies regarding the optimal energy level for monoenergetic extrapolation for patients with metallic implants, with quoted optimal levels between 105 keV and 150 keV in the current literature. 10,15 –20 Further studies with a larger sample size and studies about the use of optimal keV reconstructions are recommended.
Conclusion
Our study shows that for patients with metallic implants, monoenergetic extrapolation of DECT at high theoretical energy level (150 keV) can reduce metal artifacts, increase SNR, and improve qualitative image quality compared to conventional SECT at comparable radiation dose.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.