
Abstract
Introduction:
C1 lateral mass (C1LM) screw is a common procedure in spine surgery. However, related studies are lacking in Asia. We aim to determine the safety of C1LM screw for the Chinese, Indians, and Malays.
Methods:
Three-dimensional computed tomographies of 180 subjects (60 from each ethnic) were analyzed. The length and angulations of C1LM screw and the location of internal carotid artery (ICA) in relation to C1LM were assessed and classified according to the classification by Murakami et al. The incidence of ponticulus posticus (PP) was determined and the differences among the population of these three ethnics were recorded.
Results:
The average base length was 8.5 ± 1.4 mm. The lengths within the lateral mass were between 14.7 ± 1.6 mm and 21.7 ± 2.3 mm. The prevalence of PP was 8.3%. 55.3% (199) of ICA were located in zone 0, 38.3% (138) in zone 1-1, 6.4% (23) in zone 1-2, and none in zone 1-3 and zone 2. The average angulation from the entry point to the ICA was 8.5° ± 6.4° laterally. The mean distance of ICA from C1 anterior cortex was 3.7 ± 1.7 mm (range: 0.6∼11.3). There was no difference in distribution of ICA in zone 1 among the three population (Chinese–47%, Indians–61%, and Malays–53%; p > 0.05).
Conclusions:
No ICA is located medial to the entry point of C1LM screw. If bicortical purchase of C1LM screw is needed, screw protrusion of less than 3 mm or medially angulated is safe for ICA. The incidence of PP is 8.3% with higher prevalence among the Indian population.
Keywords
Introduction
C1 lateral mass (C1LM) and C2 pedicle screw systems are the methods of fixation for posterior C1/C2 instrumentation. It is getting more popularity because of the superior biomechanical advantage. 1,2 C1LM screw is challenging due to the close proximity of internal carotid artery (ICA) and vertebral artery (VA). Violation of VA by C1 screws is uncommon compared to C2 screws. However, approximately 5% of C1LM screw violation into the VA foramen were reported by Yeom et al. 3 Currier et al. reported a case of ICA impingement by a well-positioned C1-C2 transarticular screw. 4 Bogaerde et al. presented a case of ICA pseudoaneurysm causing repeated cerebral infarcts secondary to C1-C2 transarticular screw. 5 Previous publications have reported on the vascular anatomy, safety, and feasibility of C1LM screws. 6 –9 However, there are few studies which analyzed the safety of C1LM screws in Asians and specifically in Chinese, Indians, and Malays who represent the majority of the population in the Southeast Asia region. 10 Hence, this study was designed to determine the feasibility and safety of C1LM in these Asians, with reference to the C1 vertebral morphometry, presence of ponticulus posticus, and the relation of ICA to the C1LM.
Methods
Ethical approval was obtained from our institution to retrieve computed tomography (CT) scans which was performed from June 2010 to December 2013. Only CT scans of cervical spine with 1 mm slice and of patients aged above 20 years were included in the review. The exclusion criteria were medical or surgical conditions distorting the anatomy of C1 vertebra (e.g., arthritis, tumor, infection, acquired or congenital deformity, and trauma), abnormality of the ICA (aneurysm and stenosis), and suboptimal quality of the CT scans. A total of 180 subjects were included; 60 subjects from each ethnic that is, Chinese, Indian, and Malay. The male to female ratio was 1:1 (90 each). They were analyzed for left and right sides, that is, 360 measurements for each parameter. The mean age of the study population was 50.6 ± 16.5 years (range: 20–92 years).
All the CT scans were analyzed using the Mimics® version 15.0 (Materialise, Belgium). Mimics is a software program thath allows conversion of CT images into three-dimensional (3D) models with delineation of the soft tissue structures, that is, vessels using different range of thresholding. It also allows reslicing of the 3D model in the direction of the preferred screw entry point and trajectories. Hence the measurement can be made accurately and reliably.
The detailed step of the image reproduction and measurement technique using this software is outlined below: All CT scans were downloaded as Digital Imaging and Communications in Medicine (DICOM) images and imported into the Mimics interface. Segmentation was done to extract 3D information from 2D images. Thresholding was used to define the bone by selecting appropriate range of pixel-gray values. For this study, we used threshold value between 226 and 1600 Hounsfield units. Dynamic growing was done to differentiate arteries from the surrounding tissues. 3D calculation was performed and 3D model was displayed in the Mimics interface. Reslicing was performed in order to get precise anatomical alignment.
The entry point for C1LM described by Currier and Yaszemski 11 was applied. In this technique, a 4-mm burr was used to remove the lower portion of posterior arc until the lateral mass is reached. This entry point is represented as X point in the study (Figure 1).
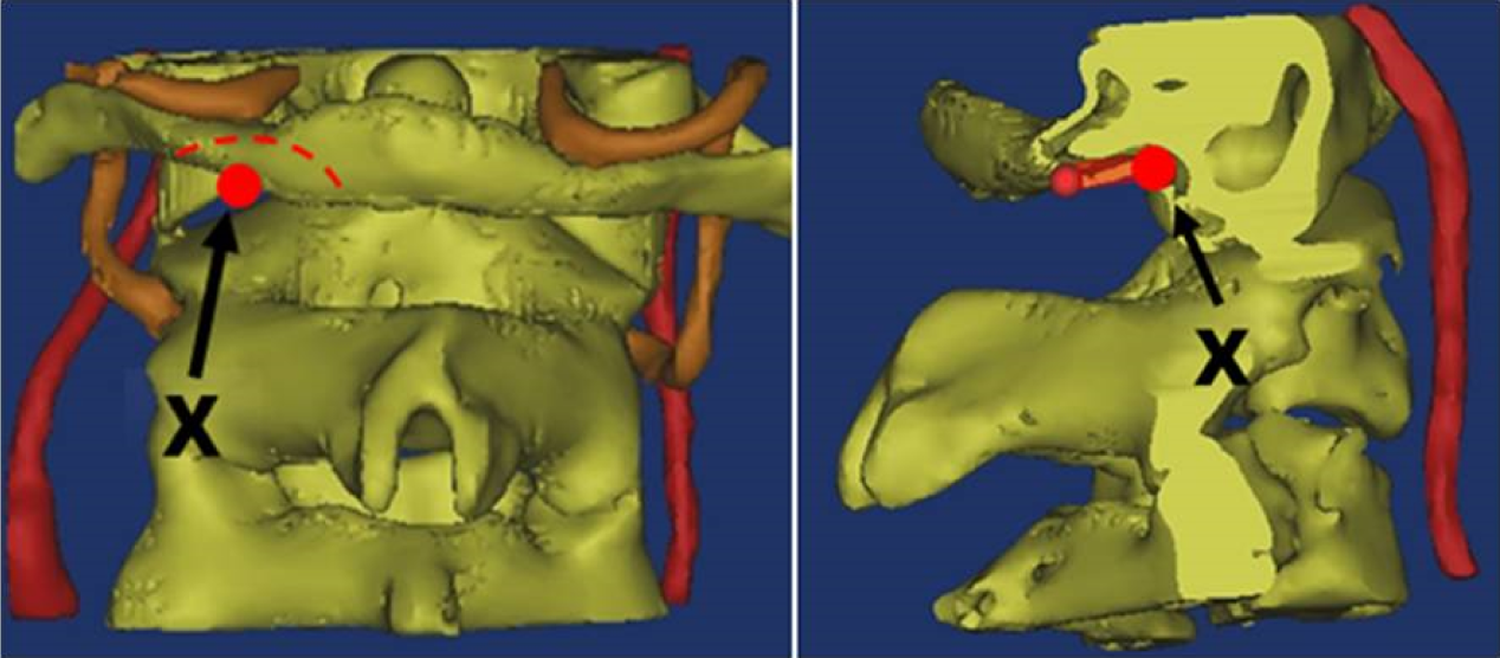
The entry point (X) for C1 lateral mass screw following Currier’s technique. Using a 4 mm burr, the lower portion of posterior arch (shaded area) is burred until the lateral mass is reached, the X point.
For measurements in the axial plane, the 3D CT models were resliced according to the neutral sagittal plane of C1LM (Figure 2). Likewise when sagittal measurements were performed, the 3D models were resliced according to the vertical axis of C1LM on each side (Figure 3).

Landmarks and measurements on C1 axial plane, which were resliced according to the neutral sagittal axis of C1 lateral mass (C1LM). The X represented the entry point of C1LM screw. The shortest length, that is, SLa and the longest lengths, that is, LLa are represented using small and large dotted lines. The gray- and black-shaded areas represent their corresponding trajectories (SAa and LAa). SAa: axial plane trajectory (maximum lateral angulation); LAa: axial plane trajectory (maximum medial angulation).

Landmarks and measurements on C1 sagittal plane which were resliced according to the vertical axis of C1 lateral mass at X point. The shortest length, that is, SLs and the longest lengths, that is, LLs are represented using small and large dotted lines. The gray- and black-shaded areas represent their corresponding trajectories (SAa and LAa). BL illustrates the measurement for base length.
Length
i. S length (SL) is defined as the shortest distance from X entry point to anterior cortex of C1, with an allowance of 2.25 mm (accounting for half of the diameter of a 4.5-mm C1LM screw) from the cortices to avoid cortical breach.
SLa refers to distance in the axial plane (Figure 2), whereas SLs refers to distance in the sagittal plane (Figure 3).
ii. L length (LL) is defined as the longest distance from X to anterior cortex of C1, with an allowance of 2.25 mm from the cortices to avoid cortical breach.
LLa refers to distance in the axial plane (Figure 2), whereas LLs refers to distance in the sagittal plane (Figure 4).
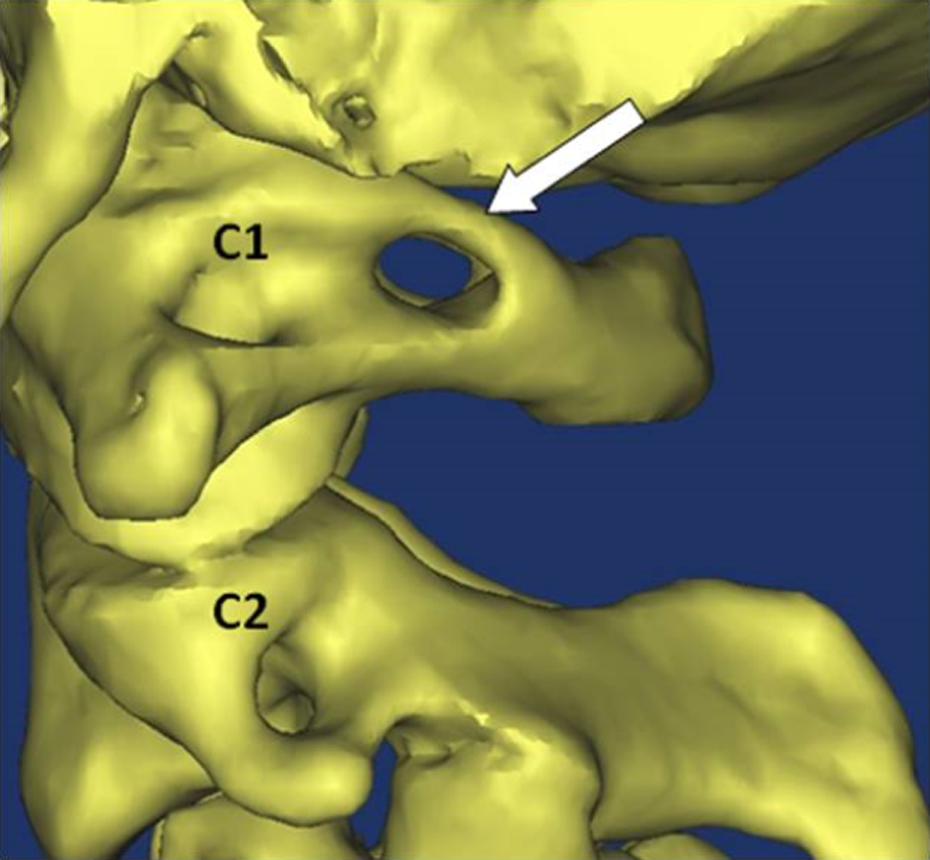
Abnormal bony bridge (arrow) over the superior surface of C1 posterolateral arc, that is, ponticulus posticus.
iii. Base length (BL) is defined as the distance from the posterior arc to X entry point, which is measured on sagittal plane (Figure 3).
Trajectory
i. S angle (SA) is defined as the angulation for the shortest C1LM screw length.
SAa refers to axial plane trajectory (maximum lateral angulation) (Figure 2), whereas SAs refers to sagittal plane trajectory (maximum caudal angulation) (Figure 3).
ii. L angle (LA) is defined as the angulation for the longest C1LM screw length.
LAa refers to axial plane trajectory (maximum medial angulation) (Figure 2), whereas LAs refers to sagittal plane trajectory (maximum cephalad angulation) (Figure 3).
iii. T angle (TA) is the summation of SA and LA for safe screw insertion.
TAa refers to the safe zone in the axial plane, whereas TAs refers to the safe zone in the sagittal plane.
Identification of ponticulus posticus (PP)
PP is defined as abnormal formation of bony bridge over the superior surface of the posterolateral C1 arch 12 (Figure 4).
Relation to ICA
The center of ICA was taken as the reference for location which was divided into three zones as described by Murakami et al. 13 (Figure 5). The zones were created by vertical lines over the medial border of lateral mass and over the medial border of foramen transversarium of C1.

Internal carotid artery location according to zones as described by Murakami et al. 13
The edge of ICA was taken as the reference for distance whereby the shortest distance to anterior cortex of C1LM was measured (ICA-C1D). The center of the ICA was taken as the reference for trajectory whereby the angle form in between the line connecting the C1LM screw entry point to the ICA and the vertical line was measured (ICA-C1A) (Figure 6).
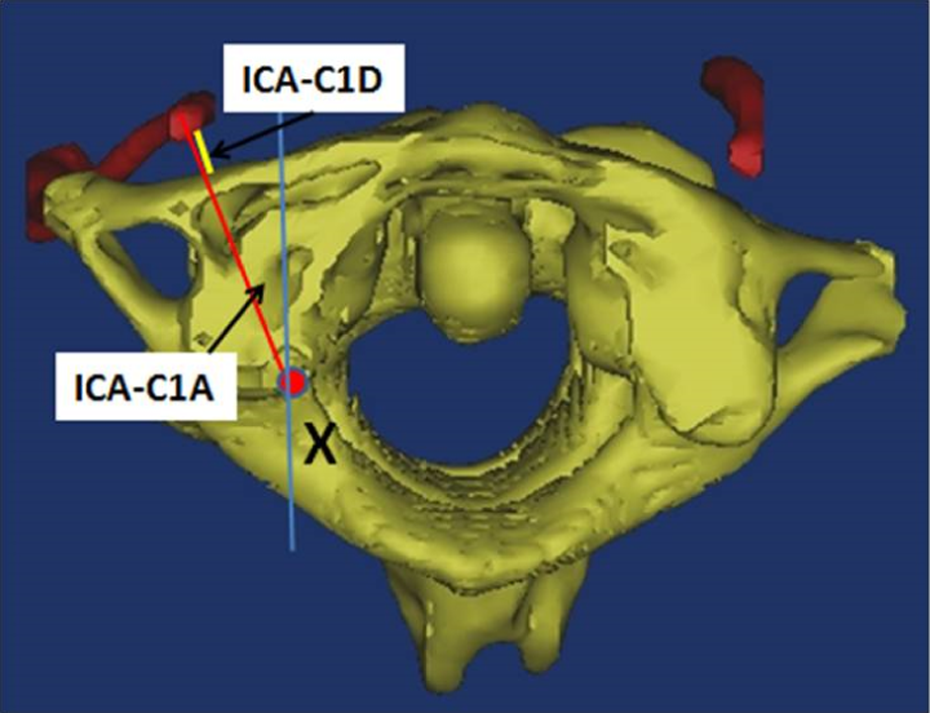
Internal carotid artery (ICA)-C1D is the shortest distance of ICA to anterior cortex of C1 lateral mass (C1LM). ICA-C1A is the angulation form in between the line connecting the C1LM screw entry point to the ICA and the vertical axis.
SPSS® version 22 was used for statistical analysis. Descriptive statistic was performed first for all parameters. Independent sample t-test was used when comparing gender and side, while one-way analysis of variance (ANOVA) test was performed when comparing the population of the three ethnics, that is, Chinese, Indian, and Malay. A factorial ANOVA test was used to assess any confounding factors. When comparing the incidence of PP, chi-square test was used.
Results
The mean C1LM BL was 8.5 ± 1.4 mm. The shortest length within lateral mass (SLa) averaged 14.7 ± 1.6 mm with lateral angulations (SAa) of 11.0° ± 7.7°. Medial angulation increased screw length, with longest screw length (LLa) of 21.7 ± 2.3 mm and screw trajectory of 29.1° ± 6.2° medially. In the sagittal plane, cephalad angulation (LAs) of 20.9° ± 7.8° to caudal angulation (SAs) of 37.0° ± 10.2° with total trajectory angle (TAs) of 57.9° ± 9.0° was safe. There were 30 PP detected, with the incidence of 8.3% (Table 1).
The C1 parameters in length and angulation, the incidence of PP, and the comparisons in between genders, sides, and ethnics.

PP: ponticulus posticus; ANOVA: analysis of variance; SD: standard deviation; SAa: axial plane trajectory (maximum lateral angulation); SLa: distance in the axial plane; SLs: distance in the sagittal plane; LLa: distance in the axial plane; LLs: distance in the sagittal plane; BL: base length; LAa: axial plane trajectory (maximum medial angulation); TAa: the safe zone in the axial plane; TAs: the safe zone in the sagittal plane; SAs: sagittal plane trajectory (maximum caudal angulation); LAs: sagittal plane trajectory (maximum cephalad angulation).
ƨThe incidences of PP were 5.8%, 14.2%, and 5.0% for Chinese, Indians, and Malays respectively. Both Chinese and Malays had lower incidence of PP as compared to the Indians (p = 0.031, 0.016, respectively).
The location of ICA in relation to C1LM was classified according to Murakami et al. 13 In all, 44.7% of ICAs were located within zone 1 and the remaining 55.3% were within zone 0. There was no ICA in zone 2 in this study. When zone 1 (n = 161) was further analyzed according to its subzone, 85.7% (n = 138) was within subzone 1-1, 14.3% (n = 23) in subzone 1-2, and none in subzone 1-3. The mean distance of ICA to anterior cortex of C1LM (ICA-C1D) was 3.7 ± 1.7 mm (range 0.6–11.3 mm). The mean ICA trajectory, that is, ICA-C1A was lateral angulation of 8.5° ± 6.4° (range: 0°–32.2°) (Table 2). When the ICA-C1D was further analyzed according to the zonal distribution, the average distance was noted closest at zone 0 (3.5 ± 1.8 mm) and furthest at zone 1-2 (5.1 ± 1.5 mm). However, the ICA could be located as close as 0.9 mm at zone 1-1 and 0.6 mm at zone 0. For those ICAs with ICA-C1D of less than 3 mm, 67.9% were located in zone 0, 31.3% in zone 1-1, and only 0.8% in zone 1-2. Of the 23 ICAs located at zone 1-2 (neutral direction), 1 (4.3%) was located less than 3 mm from anterior cortex (Table 3).
The ICA-C1 relation in zonal location, distance, and angulation with their comparisons in between genders, sides, and races.

ICA: internal carotid artery.
The distance of ICA to anterior cortex of C1 (ICA-C1D) based on the location of ICA (ICA-C1 Zone) according to Murakami et al. 13

ICA: internal carotid artery; SD: standard deviation.
Comparison between genders
Males had significant larger length in SLa, SLs, and LLs (p < 0.05). They also had significant larger angulations and safe zones in SAa, SAs, TAa, and TAs. Although the incidence of PP was higher in males than in females, it was not statistically significant (p > 0.05) (Table 1). There was no difference in the location of ICA among the genders (p = 0.112). The mean ICA-C1D was 4.0 ± 1.9 mm in males and 3.5 ± 1.6 mm in females, a difference that was statistically significant (independent samples t test, p = 0.012). There was no difference in ICA-C1A among the genders (p = 0.517) (Table 2).
Comparison between right and left side
The right side was significantly longer in SLs, LLs, and BL. In the axial plane, the right side had larger lateral angulation but the left side had larger medial angulation. The left side also had larger cephalad angulation and sagittal safe zone. There was no significant difference in the incidence of PP when comparing the right side and left side (Table 1). For the right ICA, its location was equally distributed in zone 0 and zone 1 (49.4% and 50.6%, respectively). For left ICA, 38.9% were within zone 1, while the remaining 61.1% were within zone 0. The mean ICA-C1D for right side and left side were 3.8 ± 1.6 and 3.6 ± 1.9 mm, respectively. No significant difference was noted when the right side and left side were compared (paired t test, p > 0.05) (Table 2).
Comparison between ethnics
The mean BL was 8.7 ± 1.4 mm for Chinese, 8.3 ± 1.3 mm for Indians, and 8.6 ± 1.4 mm for Malays (Table 1). The SLa was 14.9 ± 1.5, 14.0 ± 1.5, and 15.2 ± 1.5 mm in Chinese, Indians, and Malays, with corresponding lateral angulations of 10.9° ± 7.2°, 9.2° ± 6.6° and 13.0° ± 8.8°, respectively. The LLa of 22.1 ± 2.2 mm with medial angulations of 29.6 ± 5.4° for Chinese, length of 20.6 ± 1.9 mm with medial angulations of 29.9° ± 6.5° for Indians, and a length of 22.3 ± 2.3 mm with medial angulations of 27.9° ± 6.4° for Malays were noted. In the sagittal plane, the safe trajectories were between cephalad angulation of 22.6° ± 7.0° to caudal angulation of 36.4° ± 10.8° with total trajectories of 58.9° ± 9.2° for Chinese. In Indians, it was between cephalad angulation of 20.8° ± 8.0° to caudal angulation of 35.4° ± 9.8° with total trajectories of 56.2° ± 8.9°, whereas for Malays it was between cephalad angulation of 19.5° ± 8.1° to caudal angulation of 39.1° ± 9.6° with total trajectories of 58.6° ± 8.7°. In general, the Malay and Chinese groups allowed statistically longer screw than the Indians. However, in terms of zone of safe trajectories, only marginal difference was detected in the sagittal plane (TAs, p = 0.043).
The incidences of PP were 5.8%, 14.2%, and 5.0% for Chinese, Indians, and Malays respectively. Both Chinese and Malays had lower incidence of PP as compared to the Indians (p = 0.031, 0.016, respectively) (Table 1).
For the Chinese, 60.8% (73) of the ICAs were located in zone 0 and 39.2% in zone 1. Among the Indians, 49.2% (59) were located within zone 0 and 50.8% (61) were located within zone 1 whereas for the Malays, it was 55.8% (67) and 44.2% (53), respectively. There was no significant difference in zonal location among the races (p = 0.190). The mean ICA-C1D was 3.4 ± 1.8 mm for Chinese, 3.7 ± 1.7 mm for Indian, and 4.2 ± 1.6 mm for Malay and the difference was statistically significant (p = 0.001). While the mean ICA-C1A was laterally 10.2° ± 6.9°, 6.7° ± 5.2°, and 8.7° ± 6.5° for Chinese, Indians, and Malays, respectively. These were also significantly different (p < 0.001) (Table 2).
Factorial ANOVA
Factorial analysis for variance was performed to assess for any interaction between the factors, namely, gender, side, and ethnic for the parameters that showed significant difference (p < 0.05). However, there were no interaction (all the results were independent of each other).
Discussions
C1LM screw has become the preferred method for C1 instrumentation. Despite its popularity for the past decade, there is still controversy regarding its safe trajectories and screw length, as different entry points have been advocated by different surgeons. 11,14,15 Numerous anatomic and clinical studies were published regarding its surgical morphometry. However, most of them were studies carried out in the Caucasian population, and only few studies were performed in the Asian population. 14,16
Different methods and entry points have been described for C1LM screw. In the current study, the technique described by Currier and Yaszemski 11 was used for surgical morphometry measurement. In this study, the C1 screw length within the lateral mass in axial plane ranged from 14.7 ± 1.6 mm (SLa) to 21.7 ± 2.3 mm (LLa). This was not affected by change in sagittal angulation. With the BL of 8.5 ± 1.4 mm, the actual screw length to be used during surgery should be between 23 mm (BL + SLa) and 30 mm (BL + LLa) for the Asian population. Longer screw lengths corresponded to a more medially angulated trajectory with a mean of 29.1° ± 6.2°. Maximum lateral angulation of 11.0° ± 7.7° was noted to be safe from perforation. In the sagittal plane, only cephalad angulation would have clinical importance by using Currier’s technique 11 because the superior part of the posterior arch would prevent any caudal angulation. In this study, the maximum cephalad angulation was 20.9 ± 7.8 (Table 1).
No existing surgical morphometric studies using Currier’s technique 11 are available in the literature (Table 4). This makes a direct comparison with other published reports difficult. 8,14,16,17 The lateral mass length has been reported to be in the range of 14.4–28.6 mm. The medial angulation ranged from 9.8° to 33°, while lateral angulation ranged from 6.6° to 13°. The cephalad angulation ranged from 2.4° to 22.1°. The findings (SLa and LLa) in the current study are within the range reported in the literatures but are relatively smaller and shorter. The wide range of reported measurements is due to the different methods of study, screw diameter, entry point, and population. Tan et al. 14 and Ma et al. 16 studied on the Chinese and the rest of the studies were carried out in the Caucasian population. In the study by Ma et al., 16 the author fixed the angulations at 10° medial and 5° cephalad for length measurement. The longest C1 screw length of 30 mm (BL + LLa) in the current study was similar to the findings reported by Tan et al. 14 and Gebauer et al. 6 because both used the entry point on the posterior arch of C1. Even though the entry point described by Currier and Yaszemski 11 is anterior to the entry point described by Tan et al., 14 the actual screw length should be similar because the screw head would still sit on the surface of the posterior arch in both the techniques.
Summary of the related literatures for C1 lateral mass morphometric measurements and the current study.

N/A: not available; CT: computed tomography; M: male; F: female; ‡: in relation to horizon; S: shortest; L: longest; Φ: fixed by author; Lt: left; Rt: right.
To the best of our knowledge, this is the only study comparing C1 morphometry among the Asians. The Indians had shorter C1LM length by 2.0–2.5 mm as compared to the Chinese and Malays. The difference of about 2° found in medial, lateral, and cephalad angulations among the Asians should not have any clinical significance. There was no significant difference in their safety window (Table 1).
Subperiosteal dissection over the posterior arch of C1 is necessary to identify the entry for C1LM screw. Presence of bony anomaly such as PP can cause inadvertent VA injury during surgical exposure of the C1 posterior arc. Moreover, the possibility of inserting screw into the arcuate foramen should not be underestimated. The prevalence of PP, that is, 8.3% in this study, is lower than those reported in the literatures, that is, 9.4%–26.9%. 18 –21 The Indians had a significantly higher prevalence of this bony anomaly as compared to the Chinese and Malays.
Bicortical purchase of C1LM is sometimes necessary in patients with osteoporosis or those with severe instability. However, it is well known that the ICA may be injured by a bicortical screw tip leading to life-threatening hemorrhage, stroke, pseudoaneurysm, arteriovenous fistula, or stenosis. 4,5,22 Thus, location and distance of ICA from C1 anterior cortex need to be evaluated preoperatively. This study found that the mean ICA-C1D was 3.7 ± 1.7 mm with 55.3% of them located in zone 0 and the remaining located in zone 1. None of the ICA was located in subzone 1-3 and zone 2. Thus, any medial angulation of C1LM screw is safe to avoid ICA injury. In the event where a bicortical C1 screw is directed neutrally, screw protrusion beyond the anterior cortex of less than 3 mm is generally safe. However, the surgeon should be aware that 0.8% of ICA in zone 1-2 (directly neutral) had a distance of less than 3 mm from anterior cortex of C1. The mean ICA-C1A was 8.5° ± 6.4° laterally directed. This finding was very similar to the study by Estillore et al. 23 (Table 5). Variation in ICA location compared to our study was reported in the literature (Table 5) and is most likely due to the different reference points used in other studies. For instance, Currier et al. 24 and Murakami et al. 13 used the medial edge of ICA as the reference point, while Estillore et al. 23 and this study used the center of ICA as the reference point. Among the Indian population, there was a higher probability of ICA injury if bicortical C1LM screw was performed compared to the Chinese due to higher percentage of ICA in zone 1. Fifty-one percent of the former’s ICA were located in front of the lateral mass as compared to 39% in the latter (p = 0.028) (Table 2).
Summary of the related literatures for relation of ICA to C1 lateral mass and the current study.

ICA: internal carotid artery; N/A: not available; CT: computed tomography; Lt: left; Rt: right.
As with any study, there were limitations. The measurements in our study were done by a single assessor. This might lead to observer bias. A single method of screw entry point was applied for C1 morphometric measurements. Therefore, the results of our study might not be practical for surgeons who utilize a different entry point for C1LM screw insertion. The differences found in our study are very small in terms of length and angulations, which may not have any clinical significance.
Conclusions
Our study provides important reference values with regard to C1LM screw lengths and trajectories, prevalence of PP, and the relation of ICA to C1LM for the Chinese, Indians, and Malays. The estimated C1LM screw length among the Asian population was 23–30 mm with the safe zone in the axial plane of 11° lateral to 29° medial and sagittal safe zone of 21° cephalad. Ethnic differences exist in the morphometric measurements, with the Indians having shorter screw length. The incidence of PP was 8.3%. The Indians have a higher incidence of PP compared to the Chinese and Malay population; 55% of ICAs were located in zone 0 with a mean lateral angulation of 9° from the C1 entry point and 4 mm distance from anterior cortex of C1LM. Medial angulation of C1LM screw or bicortical purchase of less than 3 mm from anterior cortex would avoid injuring the ICA. The distribution of ICA in zone 1 among the different populations is Chinese–39.2%, Indians–50.8%, and Malays–44.2% (p > 0.05).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.