
Abstract
Background:
One of the major challenges to total knee arthroplasty (TKA) is optimal pain control. Effective analgesia is capital in fast-track surgery programs to allow patient’s early functional outcomes.
Objectives:
Compare length of stay (LOS) short-term pain control, and patients’ satisfaction at 1 month between local infiltration analgesia (LIA) combined with femoral nerve block (FNB) and FNB only in patients undergoing TKA.
Patients and methods:
Two hundred and fifty-four patients were included in a randomized prospective study and distributed in two groups. The first group received an intraoperative LIA (150 mL mixture of ropivacaine 2.0 mg/mL + ketorolac 30 mg + adrenaline 10 μg/mL) combined to an FNB. The control group had only an FNB. Demographical data and visual analog scale (VAS) score were obtained preoperatively, at 36 h after surgery and at the 15-day follow-up. Patients’ satisfaction at 1 month was also evaluated. Statistical analysis data was performed.
Results:
No differences in demographical data and preoperative VAS score were observed between both groups. LIA group had a lower VAS score at 36 h after surgery (1.34 ± 1.31 vs. 3.68 ± 1.932 in the control group, p = 0.00), but these differences were not maintained at the 15-day follow-up (4.51 ± 1.889 vs. 4.11 ± 1.940 in the control group, p > 0.05). LOS and patients’ satisfaction were comparable between groups. Patients with LIA had no additional complications.
Conclusions:
LIA is a safe adjuvant to FNB to reduce perioperative pain during the first 36 h after TKA. Its effects wean with time, but do cover the first crucial hours of rehabilitation in a fast-track program. LIA seems don’t modify postoperative course nor patient’s satisfaction at short-term follow-up. The final impact of LIA on surgical outcome is still to be determined.
Introduction
In recent years, many innovations and advances in total knee arthroplasty (TKA) procedures were improved as implant designs and surgical techniques as well as more interest in perioperative and postoperative analgesic and rehabilitation programs; 1,2 however, in most cases, perioperative pain control continues to be suboptimal in patients receiving TKA. 1
As such, many different multimodal perioperative care models were developed to enhance recovery (also known as “fast-track methodology”). These included strategies to improve pain control, reduce surgical stress responses and organ dysfunction, and permit early mobilization. 2 These principles, applied to TKA, resulted in improvements in multimodal opioid regimens including local infiltration analgesia (LIA) technique and peripheral nerve blocks. The ultimate goal is to facilitate early mobilization and function gain, finally leading to a reduction of length of stay (LOS) and improvements in overall surgical outcomes 3,4,5 such as LOS reduction of 2–4 days with these programs compared to standard care. 5,6,7
Bianconi et al. 8 first described LIA technique in knee replacement surgery. Kerr and Kohan 5 and Kehlet and Andersen 9 performed a systematic infiltration of a mixture of ropivacaine, ketorolac, and adrenaline into tissues surrounding the surgical incision. These local infiltrations of analgesic and anesthetic were initially thought to provide effective pain relief permitting faster rehabilitation. 4
Currently, there is no consensus on their effectiveness compared to other anesthetic techniques or placebo, or what effect they may have on hospital stay. 10,11
The aim of this study is to evaluate if LIA combined to a femoral nerve block (FNB) technique offers any advantage when compared to FNB alone, in terms of pain relief in first hours after TKA surgery. Also, overall patients’ satisfaction at short-term follow-up will be studied. We hypothesize that LIA—as coadjuvant of FNB—would improve patients’ pain control in first 36 postoperative hours and improve overall patients’ satisfaction.
Materials and methods
We performed a randomized prospective controlled single blind trial of patients undergoing total knee replacement at a single institution between July 2013 and December 2013. Hospital ethical committee approved the study protocol prior to implementation. Patient’s database was done to obtain demographic characteristics (sex, age, laterality, etc.). Inclusion criteria were set to include patients with tricompartmental osteoarthritis of the knee with no anesthetic or surgical contraindications to TKA. Known allergies to the medications used in the study were considered to be absolute exclusion criteria. Finally, patients with emerging medical comorbidities or intraoperative complications that would limit postoperative physical therapy participation were considered individually and excluded from the final analysis.
The study protocol was explained to enrolled patients, and both oral and written consent was obtained from all patients before surgery. In addition, visual analog scale (VAS) score (range from 0 (no pain) to 10 (worst pain)) was also collected at the last preoperative visit.
We followed the standard perioperative standards of care established at our institution. Peridural block was performed prior to the intervention. Three different surgeons performed surgical procedure. They followed the same surgical technique (detailed below) and used similar implant (NexGen® cemented PS TKA (Zimmer® Inc., Warsaw, Indiana, USA)). TKA was performed through an anterior approach with medial parapatellar arthrotomy. The incision extends caudally and reaches at most 1 cm proximal to the patella, as to protect local soft tissues. Tourniquets were used from skin incision to wound close. Intraoperative tranexamic acid single dose (10 mg/kg in 50 mL) was administrated 30 min before wound closing and no drainage was left.
Prior to surgery, patients were randomized into two groups by an independent investigator (computerized blocked random number list) and the randomization branch was communicated to the surgeon and anesthesiologist before surgery starts. The same-blinded nurse obtained all VAS results before and after surgery. Only the surgeons and anesthesiologists were knowledgeable about the patient’s group during all phases of the study. Other personnel involved in patient’s care remained blind throughout the study. Patients were made aware of the randomization group at the end of the study.
All patients received a femoropopliteal nerve block after surgery as part of our hospital’s standard of care. In addition, the intervention group received an intraoperative LIA as per randomization. The remaining patients did not receive any further injection and were considered to be the control group. The injected mixture of LIA consisted of 150 mL ropivacaine hydrochloride (Naropin®, AstraZeneca® London, UK) 2.0 mg/mL mixed with 30-mg ketorolac tromethamine and 1 mL (10 μg/mL) of adrenaline. Half mixture volume was injected (75 mL) in the surgical field in previously designed points (periosteal borders, intramedullary bone, synovial tissue, posterior capsule and extensor apparatus, and subcutaneous wound tissue; Figure 1 (Image 1)).

Intraoperative infiltration technique. (a) Posteromedial and posterior articular capsule. (b) Peripatellar tissue and quadricipital tendon. (c) Pes anserine, medial collateral ligament (MCL), and tibial periosteum. (d) Proximal MCL and supracondylar periosteum. (e) lateral collateral ligament (LCL), popliteal insertion, and posterolateral capsule. (f) Intramedullary cutted bone.
Postoperative care was identical in both groups. Standard postoperative painkillers were prescribed equally to both groups and consist on intravenous administration first 24 h after surgery and oral administration posteriorly. Protocol include acetaminophen 1 g/8 h combining every 4 h with non steroidal antiinflamatories drugs (NSAIDs) (dexketoprofen 25 mg/8 h) and tramadol 50 mg/8 h. Patients with allergies to any of these medications received metamizol 2 g iv/8 h (oral prescription dosage was 1250 mg/8 h) instead. Heparin and gastric protection was also provided in all patients. As per the rehabilitation protocol, patients were instructed to start smooth knee flexion 8 h after surgery and weight bearing was allowed the day after. As per the institutional fast-track protocol, rehabilitation process was performed for 2–3 days after surgery depending on quadriceps weakness after FNB, and then, patients were evaluated for discharge if adequate pain control was achieved, autonomous transfers and assisted deambulation (at least 10 m with crouches). Other discharge criteria included ROM of at least 75° of flexion and no wound problems.
Patients’ VAS score and ROM were collected by an independent and blinded investigator at the last clinical visit prior to surgery, 36 h after surgery, at discharge, and during patients clinical visit 15 days after surgery. The ROM was used as a metric reference for good progression of postoperative physical therapy. We considered satisfactory evolution as ROM of at least −5/80° at the 15-day follow-up. Total LOS was also documented, and patient’s satisfaction was collected at 1-month follow-up using four-item test (poor, acceptable, good, and excellent) for the overall process, emphasizing in pain control and rehabilitation timing.
Demographics were reported as percentages for nominal variables and as mean (SD) or as a median (range) for continuous variables. Differences between the groups were analyzed using Student’s t-test and Mann–Whitney U-test. Analysis of age, sex, and satisfaction distribution was analyzed by χ 2 test. Statistical analysis was performed using IBM SPSS Statistics version 17.0.
Results
From July 2013 until December 2013, a total of 270 patients received a TKA at our institution. Only 259 of these met inclusion criteria (189 women and 70 men) and were randomized into two groups. One hundred and twenty-one patients received an LIA and 138 patients were included in the control group. Postoperatively, two patients suffered postoperative periprosthetic fracture in the first 48 h and three suffered wound problems (one of which required surgical debridement for acute surgical site infection). These patients were excluded from the final analysis because of these morbidities complicating the postoperative course. A separate analysis was done for these five patients to determine harm and failed to prove any relationship with the intervention received.
A total of 254 patients were finally available for analysis, 120 in the LIA group and 134 in the control group (Figure 2). Mean age of patients was 69.9 ± 7.9 years (70.6 ± 7.7 in infiltration group and 69.2 ± 8.1 in no infiltration group with a range of 47–87 years (p = 0.167). Out of the 134 patients in the control group, 104 were females and 30 were males, with a knee proportion of 77:57 (R:L). The LIA group was composed by 83 women and 37 men showing 8:7 proportion (R:L). No differences between both groups in demographic data were observed (Table 1).

Flow chart.
Demographic data.
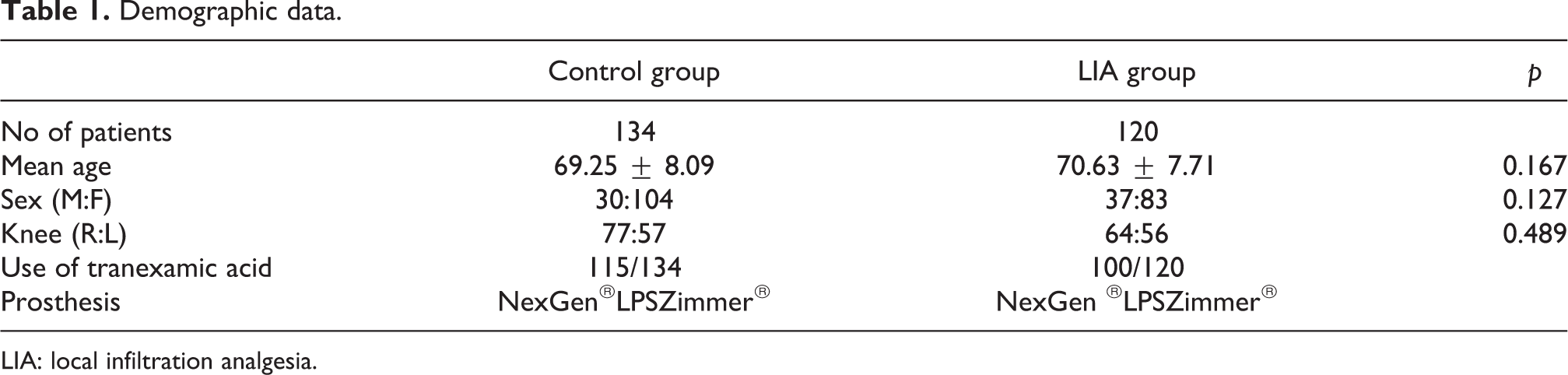
LIA: local infiltration analgesia.
Mean preoperative VAS in both groups was 6.3 ± 2.5, and no differences could be found between LIA (6.4 ± 2.5) and control group (6.2 ± 2.6, p = 0.067). On the other hand, VAS at 36 h after surgery was 1.34 ± 1.31 in the study group, whereas it was 3.7 ± 1.9 in the control group reaching statistical significance (p < 0.001). VAS at 15 days was higher in the LIA group (4.5 ± 1.9) than in the control group (4.1 ± 1.9). This difference however did not reach statistical significance though (Table 2).
Results of ROM, LOS, and VAS measurements in both groups.
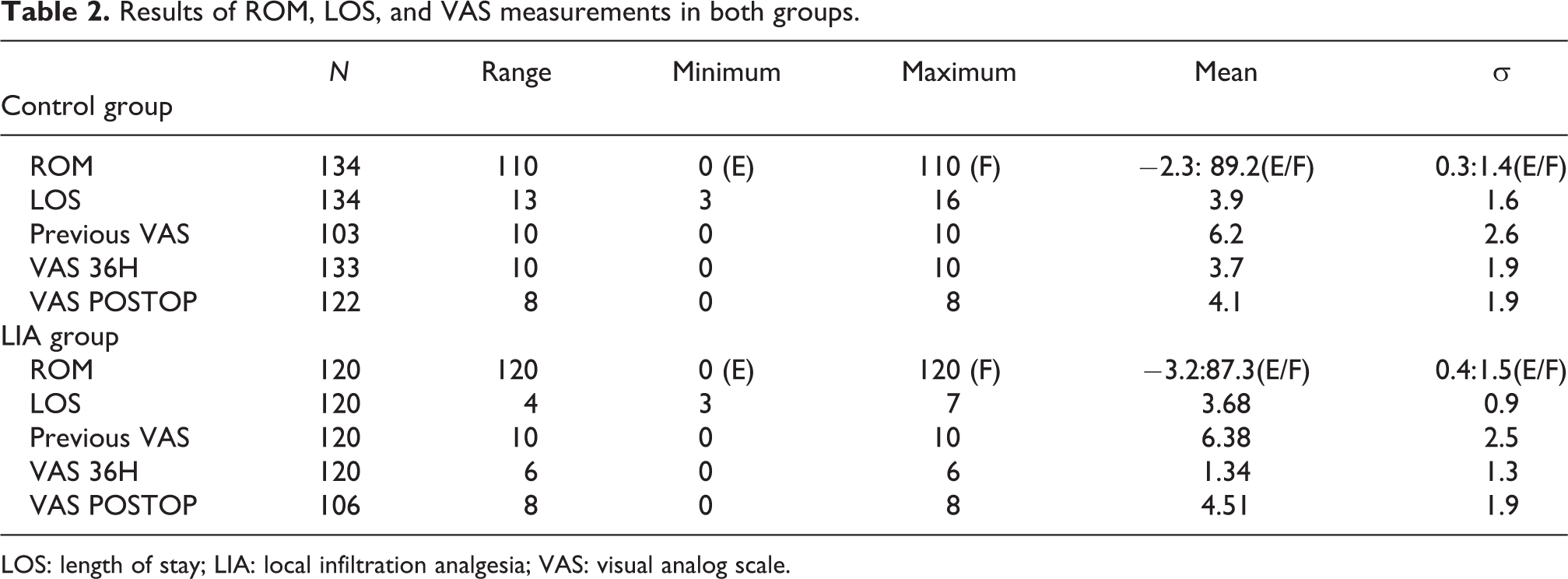
LOS: length of stay; LIA: local infiltration analgesia; VAS: visual analog scale.
Analyzing the results of both groups, we could detect statistical significance in both groups using nonparametric (Mann–Whitney U-test) and Student’s t-tests comparing VAS prior to surgery and VAS at 36 h after TKA (p < 0.001). However, we didn’t find differences between groups (p = 0.115), when comparing preoperative VAS and VAS at 15 days.
No statistical differences could be detected in terms of LOS between the LIA group (3.7 ± 0.9 days (range 3–7)) and the control group (3.9 ± 1.6 days (range 3–16) (p = 0.24).
Both groups reached ROM objectives (−5/80° at 15-day follow-up) satisfactorily. In the LIA group, we observed a mean flexion of 87.3° ± 16.8° and −mean extension of 3.2° ± 4.3°. Likewise, in the control (FNB) group, the recorded flexion was 89.2° ± 16.2° and knee extension was −2.3° ± 3.4°. No statistically differences between the two groups could be detected in terms of ROM (extension and flexion p = 0.066 and p = 0.376, respectively).
With regard to patients’ satisfaction at 1 month after surgery, we had 224 questionnaires available for analysis with 30 items being lost (11.8%) almost equally between both groups. There was no difference between groups with regard to satisfaction (p = 0.082) with both good (Table 3; Figure 3).
Satisfaction results were analyzed by χ 2 test and showed no statistically significant differences between both groups.

LIA: local infiltration analgesia; FNB: femoral nerve block.
χ = 6.713.
p = 0.082.

Satisfaction graph. Results from satisfaction analysis in both groups are shown in the graph. Major part of patients were acceptable and good satisfied in both groups. Instead, there are no differences between groups; the results in LIA group tend to be better. LIA: local infiltration analgesia.
We had no local or systemic complication due to the administration of LIA.
Separate analysis of the complications suffered during the study (one periprosthetic joint infection, two wound problems, and two periprosthetic fractures) showed no association between type of complication and study group. Also, our complication rate was comparable to the published literature. 31,32
Discussion
This is not the first study to analyze the effects of LIA in the literature, but we only find few studies analyzing patients’ satisfaction after this procedure. Moghtadaei et al. 34 show good results on patients’ satisfaction at 48 h after surgery but didn’t found statistical differences between groups. Mulford et al. 36 also study postoperative satisfaction in their study with a four-item score such as our system asked during short-term follow-up to 6 weeks postoperatively with no statistically differences between placebo injection versus LIA mixture. In our case, we measure patient’s satisfaction after 1 month after surgery when acute postop pain has gone and patient may review all the procedures. In our series, there are no statistical differences regarding patient’s satisfaction but seem to see a trending relation between good and excellent satisfaction and LIA group and poor results with FNB only (Figure 3).
Gibbs et al. 10 report a review of the literature up to 2012. The analyzed studies were heterogeneous and compared different techniques, from placebo to FNB and showed varying results. Also, the LIA mixture used in the different studies included different analgesics concentrations, commonly high volumes of local anesthetic such as bupivacaine and ropivacaine with long-term action NSAIDs like ketorolac or COX-2 and adrenaline. The most effective technique consisted of infiltrating a mixture of high-dose ropivacaine with adrenaline and ketorolac. 10 Single intra-articular versus continuous perfusion were also studied, 19 but no differences were observed between these two techniques. A single LIA intraoperative injection seems to be the most effective treatment. 10,20 –23,33 Delayed infiltration during postoperative care doesn’t seem to be more effective. 4,26,27
We decide to compare FNB associating LIA because previous studies had well indicated the effectiveness of these two methods in relieving pain after knee replacement surgery. 18,20,22,35,37
Andersen and Kehlet 13,14 28 and Xu et al. 29 published recent reviews and studies about the effects of LIA in TKA. They concluded that LIA provides effective analgesia in the initial postoperative period after TKA in most randomized clinical trials even when combined with multimodal systemic analgesia.
It is still controversial if LIA reduces the utilization of conventional and opioid analgesia. Whereas some studies report that LIA was beneficial in providing adequate analgesia, 20 –22,30 others found no additional benefit to conventional analgesia. 23 –25 Drawing any solid conclusion from these studies remains very difficult due to methodological insufficiencies in most studies and especially due to heterogeneity of administered mixtures and anesthesia between studies and groups.
Although one of the objectives in fast-track programs is decrease LOS and early discharge, 7,12,15,16,17 in our study, LOS was recorded to evaluate fast-track protocol, but the results didn’t show differences, because we agree preoperatively discharge criteria with patients and established standard LOS according to discharge criteria with no changes between both groups.
Basing on our clinical impression, we think that local infiltration (LIA) may be a good adjuvant to FNB in postoperative care. This study was therefore established to investigate if this combined administration (femoral block and LIA) offered any real advantage in terms of optimal pain control, faster rehabilitation (and therefore discharge), and higher patients’ satisfaction.
We could significantly demonstrate better pain control during the first 36 h after surgery. This benefit was not maintained upon discharge however, and both groups were comparable at posterior checkpoints. Furthermore, we observed a possible rebound effect in the group treated with LIA at 15 days, even if the difference did not reach statistical significance. LIA however did not significantly improve ROM or overall patients’ satisfaction at 1 month.
There are limitations to our study. First, the administration of LIA has performed as described by Kerr and Kohan 5 except for inject volume, but don’t know if this is the optimal dosage, volume, and site injection. In addition, the combination of LIA and FNB can be a bias to obtain the pain control’s power of LIA alone, but we describe LIA technique in this study such as adjuvant to FNB for a better pain control together. Another limitation can be the subjectivity of primary studied items like VAS or satisfaction and their variability between subjects, but we analyzed VAS during time in the same subject trying to avoid this variability.
LIA is safe adjuvant to FNB to reduce perioperative pain in TKA. Its effect covers the crucial first 36 h after surgery and would facilitate the patients’ participation in fast-track rehabilitation programs. Nevertheless, caution should be taken as we did observe a certain rebound effect of LIA that did not reach statistical significance. LIA’s effect on ultimate functional results is still to be determined.
Conclusions
In conclusion, it seems that LIA may offer good pain control when combined with FNB in first 36 postoperative hours. However, it neither modifies postoperative course nor patient’s satisfaction at short-term follow-up. Further studies are still needed to link patient’s pain with increased collaboration with physical therapy and improved overall clinical results.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.