
Abstract
Neck manipulation is associated with spinal cord injury. However, occurrence of such cases is infrequent. This article presents a 33-year-old gentleman who sustained acute tetraplegia after neck manipulation. The aim of this case report is to create awareness that vigorous neck manipulation could cause injury to the spinal cord.
Introduction
Neck manipulation is part of complementary treatment for neck pain and stiffness. It is a manual treatment where a vertebral joint is passively moved between the normal range of motion and the limits of its normal integrity, though a universally accepted definition does not seem to exist. Neck and spinal manipulation is associated with many adverse effect including vertebral artery dissection, spinal cord injury, cervical subluxation or cerebrovascular accidents. 1 –3 Although chiropractitioners, physical therapist or traditional healers are familiar to perform such manoeuvres, serious adverse effects can still occur in experienced hands. Spinal cord injury occurs when there is dysfunction of the spinal cord with loss of sensory and motor function distal to the lesion.
Case report
We introduce a case of a 33-year-old truck driver, who was otherwise healthy, presented with paralysis of all four limbs for 2 days after neck manipulation. He gave account of neck and shoulder manipulation done by a certified traditional healer for shoulder spasm and pain. Soon after the manipulation, he experienced tingling and numbness at both of the lower limbs up to knee level. The numbness gradually progressed to weakness of both lower limbs, subsequently involving the upper limbs. On the third day of post neck manipulation, patient developed urinary and bowel incontinence, for which patient presented to hospital for medical attention.
Patient was alert and conscious upon presentation to hospital. His blood pressure was hypotensive requiring inotrope support shortly after being hospitalized. Examination revealed mild paraspinal tenderness at mid cervical region which resolved after third day of admission, otherwise no bruising or obvious deformity noted.
Neurological examination revealed sensations diminished at C6 dermatome and no sensation (touch and pain) felt from C7 below, motor of both upper limbs and lower limbs was grade 0, based on Medical Research Council (MRC) grading (C5 to T1, and L2 to S2 myotome: grade 0 bilaterally), consistent with American Spinal Injury Association A: Complete lack of motor and sensory function below the level of injury (Including the anal area) (ASIA A). Both upper and lower limbs were hypotonic and hyporeflexic. Anal tone was absent with bulbocavernosus reflex. Blood investigations revealed platelet counts within normal range and a normal coagulation profile. Patient denied of taking aspirin, any traditional medications or other anticoagulant medications.
Radiograph of cervical spine revealed irregular and narrowing of facet joint of C4/C5 vertebrae without any vertebral fracture. The cervical Magnetic Resonance Imaging (MRI) showed large heterogeneous collection within right lateral epidural space of C4 till C7 (see Figures 1 & 3) in keeping with hyperacute epidural haematoma, with cord oedema at the mentioned level. The haematoma had caused spinal canal narrowing, with narrowest at spinal canal C6/C7 measuring 6.2 (Antero-posterior dimension [AP]) × 12.2 mm2 (Width [W]). The haematoma also appears to extend into the right exit foramen of C5/C6 and C6/C7 with impingement of the respective nerve roots (see Figures 2 & 4). There were no evidence of vertebral body fracture or subluxation.

Sagittal MRI of cervical spine (T2-weight), showing an area of increased intensity from C4–C7 level.
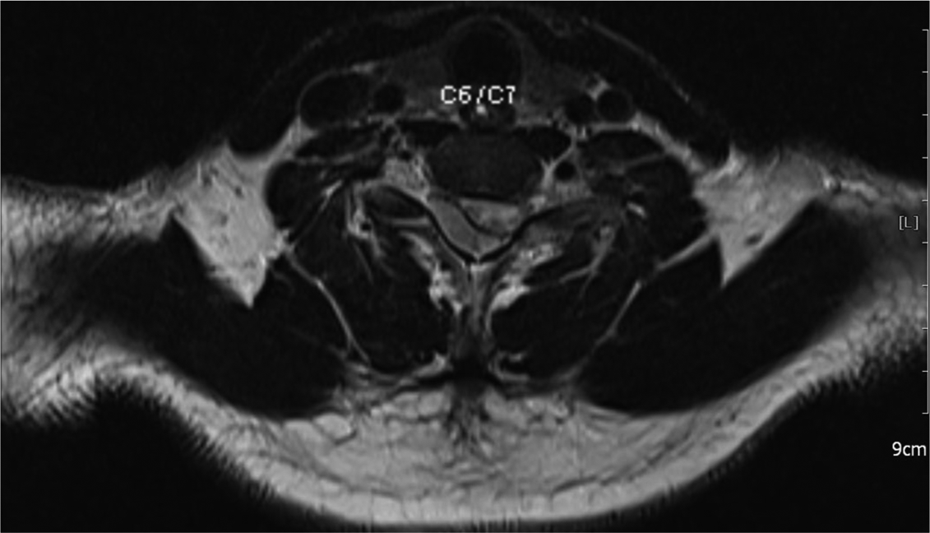
Transaxial MRI of cervical spine (T2-weight), showing compression over right posterolateral aspect of spinal cord at C6/C7 level.

Sagittal MRI of cervical spine (T1-weight), showing a hypointense collection over the posterior aspect of the spinal cord with cord oedema.

Transaxial MRI of cervical spine (T1-weight), showing compression over right posterolateral aspect of spinal cord at C6/C7 level.
Patient was started on intravenous prednisolone aimed to reduce the cord oedema while stabilized in the ward. It was aimed to proceed with an emergency decompression and laminoplasty of C3–C6. However, patient was only able to proceed for operation after 10 days due to family disputes and refused for any surgical intervention earlier on. However, in view of no improvement of neurology, patient was only agreed for a delayed decompression and laminoplasty (C3 to C6). Blood clot noted intraoperatively over the right epidural space extending from C3 to C6 and the spinal cord was not pulsatile.
Post-operatively, patient was able to be extubated, with vitals stable without requiring inotropic support. On post-operative day 1, there was some improvement in neurology, with returning of patchy sensation over C6-T1 dermatome, together with regain sensation (superficial touch and deep pain) from T2 to T12 dermatome and power grade 1 from C6 to C8 myotome. Unfortunately, on post-operative day 3 in Intensive Care Unit (ICU), patient developed sudden signs of neurogenic shock: hypotension, bradycardia and requiring ventilatory support, followed by asystole; though revived after CPR and ventilatory support in ICU, blood pressure was not able to be sustained with multiple high-dose inotropes. Patient succumbed on post-operative day 3 night for acute spinal compression, secondary to traumatic cervical injury and acute haematoma formation.
Discussion
Neck manipulation is a common practice done by either trained or untrained personnel, due to its relatively less invasive treatment modality. However, it is imperative to note that neck manipulative therapy is not risk-free. Although there have been cases reported on complications after neck manipulation, but till date, there is no definite incidence rate published. As estimated by Patijn, complication rate of post neck manipulation is around 1 in 518,886 cases. 1 However, we believed the estimated incidence rate could just be the tip of the iceberg. As estimated by multiple studies, the incidence rate varies from one per one to two million cases 2 to one serious complication per 383,750 cervical manipulations. 3 It was also concluded by Assendelft et al. that post spinal manipulation complication is usually underreported, due to physician unable to recall the cases and many minor cases were missed. 4 Thus, there is no accurate estimation of the complication rate till date. A large scale study should be conducted in order to estimate a more definite incidence rate for post-neck manipulation complication.
Generally, spinal manipulation-related complications had been classified by Assendelft et al. into vertebrobasilar accidents, cerebral accidents, hernia, cauda equina and other complications, such as myelopathy and radiculopathy as reported by Stevenson et al. 14 and Lee et al., 15 respectively. Vertebrobasilar accidents resulting in stroke were the most frequently reported, followed by intervertebral disc complications. 4 Only a very few cases of epidural haematoma have been reported after neck manipulation. 5
Epidural haematoma is a condition where there is accumulation of blood in the vertebral epidural space, which usually results from trauma or after iatrogenic procedure (i.e. lumbar puncture/epidural anaesthesia). Epidural haematoma may be associated with blood dyscrasia, coagulopathies, neoplasms and even with degenerative spinal disease. Epidural haematoma usually resulted from disc protrusion in the cases of degenerative spinal disease. 6,7
Epidural haematoma resulted from spinal manipulation is very rare, with only a handful of cases been reported worldwide. We have found a few cases of similar entity. The latest was reported by Tseng et al. from Taiwan. The reported patient was an elderly woman with underlying degenerative spinal disease who underwent neck manipulation. However, noted patient had an arteriovenous malformation, which ruptured and causing the epidural haematoma. 7 Most of the other case reports were more advanced age-group individuals with underlying long-standing degenerative spine conditions, 8 with one case report on an elderly patient with underlying atrial fibrillation on coumarin therapy with prolonged International Normalized Ratio (INR). 9 Unlike our case, who was a young individual without any underlying spinal pathology. Till date, most of the previous cases reported were associated with other risk factors, such as underlying arteriovenous malformation, degenerative spine disease and anticoagulative therapy. Another interesting case reported was in 2007, a pregnant patient at 29 weeks of gestation at the time of the unfortunate presentation. 10 This patient did not have any of the risk factors mentioned earlier. However, there had been a few case reports on spontaneous spinal epidural haematoma occurring in pregnant women. 11 Pregnancy by itself could predispose the patient to epidural haematoma formation. During pregnancy, due to the combination of altered venous dynamics and low venous pressure within the epidural space relative to venous pressure, resulting a higher pressure gradient across the epidural vessels, predisposes them to epidural hematoma. 12 There was however another similar case report in 1996 by Segal et al., with the patient seeking medical attention earlier on, with mild numbness and reduced muscle power (MRC 3/5), 13 a lesser severe form of presentation as compared to our patient.
This is the first case report of cervical epidural haematoma after neck manipulation, resulting in devastating tetraplegia and spinal shock; with the causative and resulting factors well correlated. This signifies that the complications from neck manipulation can occur in any individuals.
Unfortunately our patient succumbed to the complication, it was to our surprise by the immediate neurology recovery after a delayed decompression and laminoplasty (13 days after the initial presentation). We do believe an earlier surgical intervention would deliver a better outcome and improvements.
Conclusion
The public should be educated and made aware of the possible complications related to neck manipulation, in which some could be serious and life threatening.
For patients presented with pain and neurological deficit after a chiropractic manipulation, if suspected, an advanced diagnostic radiological investigations (MRI) should be carried out to investigate further.
It is recommended by the authors that in the future, all patients keen for chiropractic or neck massage therapy to be assessed by an orthopaedic surgeon preceding the therapy. If suspected, a neuroimaging (CT/MRI of spine) should be carried out.
An emergency decompression and laminoplasty should be considered for similar cases in the future; an earlier decompression would definitely be beneficial for the patient with a better neurology improvement.
A larger study should be conducted to determine a more definite incidence rate of post neck manipulation complications.
Footnotes
Acknowledgement
The authors would like express our gratitude to the Director General of Ministry of Health, Malaysia, for allowing the publication of this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.