
Abstract
Purpose:
Coracoid morphology has been related to coracoid impingement mainly resulting in anterior shoulder pain aggravated by forward flexion and internal rotation. However, the coracoid process morphology can also affect the inclination of the coracoacromial ligament and subsequently the subacromial space in the same way that acromial slope does. The purpose of this study was to evaluate the influence of the coracoid body–glenoid surface, coracoid tip–glenoid surface, and coracoid body–coracoid tip angles (coracoid inclination angles) on rotator cuff tears (RCTs).
Methods:
Fifty patients with documented RCT and 50 patients with normal rotator cuff (control) were included. The coracoid inclination angles were determined in both groups by measuring on computed tomography scans the angle created by the coracoid body and the glenoid surface (A1), the angle created by the coracoid tip and the glenoid surface (A2), and the angle created by the coracoid body and the coracoid tip (A3).
Results:
All angles were significantly lower in the RCT group compared to the control group: mean A1 angle of 49.7° and 54.61°, respectively (p = 0.011); mean A2 angle of 76.45° and 93.6°, respectively (p < 0.001); and mean A3 angle of 132.33° and 144.34°, respectively (p < 0.001).
Conclusions:
Decreased coracoid body–glenoid surface, coracoid tip–glenoid surface, and coracoid body–coracoid tip angles are associated with RCT. Decreased angles may reduce subacromial space by projecting the coracoacromial ligament more vertically.
Introduction
Since Neer stated in 1972 that impingement on the tendinous portion of the rotator cuff by the coracoacromial ligament and the anterior third of the acromion was responsible for the development of the chronic impingement syndrome, 1 many studies have arisen to support the extrinsic origin of rotator cuff tears (RCTs). Bigliani et al. identified three different types of acromion and the correlation of acromial morphology with RCT development in cadavers. 2 Likewise, anterior slope of the acromion, lateral acromion angle, glenoid version, scapular kinematics, and acromial coverage index have all been implicated as extrinsic contributors to RCT development. 3 –11
The coracoid morphology has also been implicated in coracoid impingement mainly resulting in anterior shoulder pain aggravated by forward flexion and internal rotation. 12 The coracohumeral distance is reduced and the subscapularis is commonly involved between the coracoid process and the lesser tuberosity. 12 –21 However, little attention has been paid to the fact that coracoid process morphology can affect the inclination of the coracoacromial ligament and subsequently the subacromial space in the same way that acromial slope does.
The purpose of this study was to evaluate the influence of the coracoid body–glenoid surface, coracoid tip–glenoid surface, and coracoid body–coracoid tip angles (coracoid inclination angles) on RCTs.
Patients and methods
Fifty consecutive patients with RCT (28 patients with open rotator cuff repair because of superior to posterior cuff tears and 22 patients with reverse prosthesis implantation because of massive cuff tears without glenoid erosion) were compared to 50 consecutive patients without RCT (25 patients with proximal humeral fracture and 25 patients with shoulder instability both subgroups treated surgically). In the RCT group, patients with rotator cuff arthropathy or glenohumeral arthritic changes were excluded. Patients with glenoid fracture or bony Bankart lesions were also excluded as were patients with any fracture affecting scapula. Cuff status was evaluated preoperatively with the aid of magnetic resonance imaging and computed tomography (CT) in the RCT group. In the control group, the status of the rotator cuff was determined by CT scans in the fracture subgroup and by CT scan and magnetic resonance imaging in the instability subgroup. In all patients, the rotator cuff status was finally assessed by direct intraoperative visualization. None of the patients included in the RCT group evidenced subscapularis involvement of the cuff tear. There were 64 females and 36 males with a mean age of 66 years. There were no significant between-group differences for age (p = 0.182) and sex (p = 0.821).
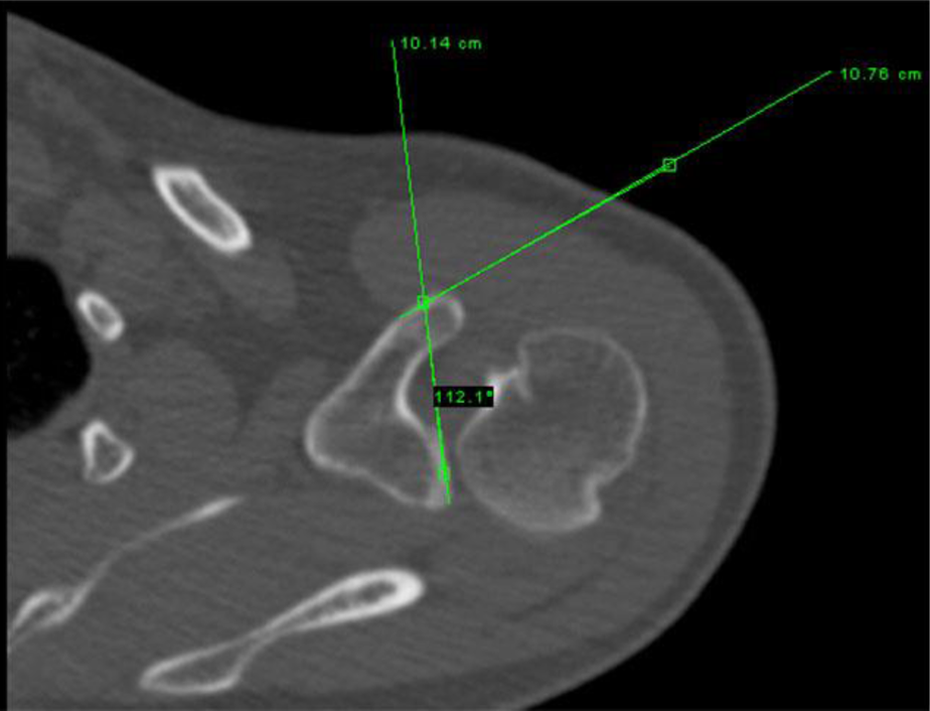
Three different angles were measured on CT scans. All angles were measured in the axial plane using the slices that better demonstrated the complete coracoid process and glenoid surface. The first angle (A1) was the angle created by a line running through the anterior cortex of the coracoid body and a line running from the posterior to the anterior aspect of the glenoid surface (Figure 1). The second angle (A2) was the angle created by a line running through the anterior cortex of the coracoid tip and a line running from the posterior to the anterior aspect of the glenoid surface (Figure 2). The third angle (A3) was the angle created by a line running through the coracoid body and a line running through the coracoid tip (Figure 3). The coracohumeral distance was also measured on the CT scan with the arm in adduction in all patients included in the RCT group and in the patients with instability of the control group, as described by Gerber et al. 16 In the RCT group, patients with rotator cuff arthropathy were excluded to avoid the influence in coracohumeral distance, and also all the patients included had an intact subscapularis and rotator cuff was limited to supraspinatus and infraspinatus. All measurements were performed by two experienced orthopedic surgeons who were blinded to the patient’s group. All measurements were done using the iPACS v5 software (General Electric Company®, Fairfield, Connecticut, USA).

A1 angle created by the angle formed between the coracoid body and glenoid surface.
A2 angle created by the angle formed between the coracoid tip and the glenoid surface.

A3 angle created by the angle formed between the coracoid body and the coracoid tip.
Statistical analysis
Descriptive statistics were used to summarize the values of all angles. An unpaired t-test was used to compare the angles between groups. A Pearson’s correlation coefficient was used to assess the influence of age and sex in angle values. A Cohen’s κ coefficient test was used to assess the interobserver reproducibility and concordance for all measured angles. All statistical analyses were conducted using the SPSS v22 (SPSS Inc., Chicago, Illinois, USA). The alpha level was set at 0.05.
Results
The between-group comparison for the coracoglenoid angle is shown in Table 1. Of notice, the RCT group demonstrated significant lower values of all angles compared to the control group. There was no significant correlation between any of the angles and age (for A1, p = 0.246; for A2, p = 0.635; and for A3, p = 0.799) or between the angles and sex (for A1, p = 0.950; for A2, p = 0.319; and for A3, p = 0.055). The mean coracohumeral distance was 0.8 cm in the RCT group and 0.83 in the control group (p > 0.05). For all angles, the κ test showed excellent reproducibility (for A1, 0.982; for A2, 0.988; and for A3, 0.962) and concordance (for A1, 0.912; for A2, 0.951; and for A3, 0.903).
Values of A1, A2 and A3 angles in the control group and the RTC (rotator cuff tear) group expressed in degrees.
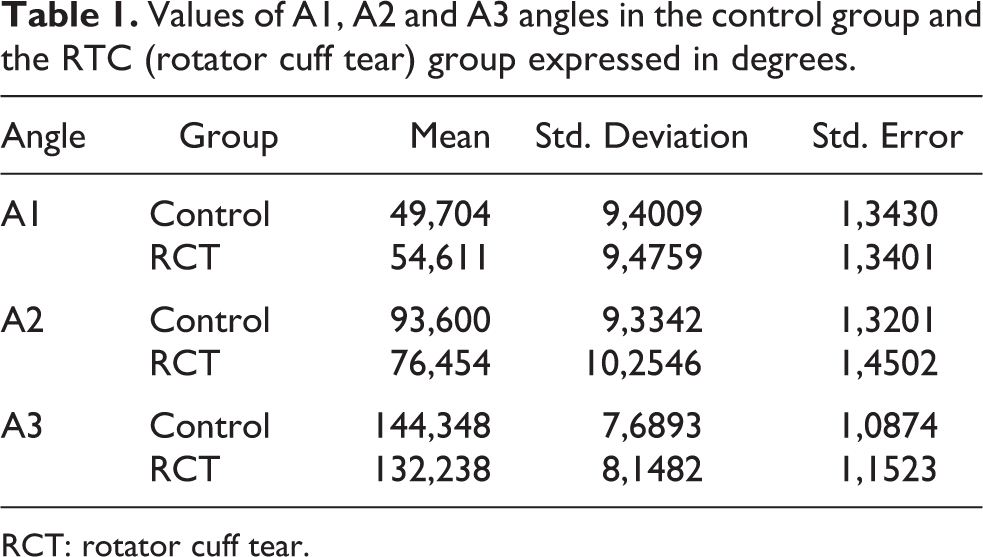
RCT: rotator cuff tear.
Discussion
The principal finding of this study was that patients with RCT had significant lower coracoid body–glenoid surface, coracoid tip–glenoid surface, and coracoid body–coracoid tip angles compared with a control group without RCT. Coracoid morphology may play a significant role in RCTs besides the already known coracoid impingement syndrome since all the patients included in the study showed a normal coracohumeral distance. The degenerative origin of the RCT can be aggravated by changes in the morphology of the coracoid.
The pathogenesis of RCT is still unclear. While Neer advocated for an extrinsic origin of the chronic impingement syndrome, 1 Codman and Akerson defended the intrinsic origin of the rotator cuff degeneration. 22 Many studies support that morphological changes of the subacromial arch have an influence on RCT development such as the type of the acromion, the anterior slope of the acromion, the acromial coverage index, the glenoid version, and the scapular kinematics. 3 –11 It is likely that the degenerative origin of RCT can be aggravated by the presence of different morphological changes in the coracoacromial arch.
Gerber et al. described the role of the coracoid process in the chronic impingement syndrome in a series of patients referring pain in the front of the shoulder aggravated during forward flexion and medial rotation in which the distance between the humeral head and the coracoid tip was significantly decreased. 12 Other authors have corroborated this finding and have reported good outcomes after coracohumeral decompression. 12,13,15,18 Coracoid impingement syndrome represents an uncommon entity that is commonly caused by trauma or iatrogenic injury. 12 –21
Although the role of the subcoracoid space in the impingement syndrome is widely recognized, the role of the coracoid process in the impingement syndrome has been centered into the reduced distance of the coracohumeral interval as the cause of anterior shoulder pain. However, this assumption misses the fact that the orientation of the coracoacromial ligament and subsequentially the subacromial space depends on the morphology of the coracoid process.
Cadaveric dissections have shown the anatomic variants of the coracoacromial ligament with different patterns of coracoid attachments demonstrating that coracoacromial ligaments with more than one bundle and larger coracoid insertion present stronger correlation with cuff degeneration. 23,24 Even though nonpathologic contact of the coracoacromial arch can be present in normal shoulders, 25 significant geometric changes have been found specially in the lateral band of the coracoacromial ligament in specimens with RCT. 26 Factors reducing subacromial space such as lateral acromion angle and acromial slope have also been implicated in rotator cuff disease because of an effect on the direction of the coracoacromial ligament, which can increase the pressure on cuff tendons. 3,4
The present study shows how the coracoglenoid angle can have an influence on RCT besides the coracoid impingement syndrome. Coracoacromial ligament direction can be influenced by the acromion morphology and in the same manner by the coracoid morphology. A diminished coracoid–glenoid surface angle may imply that the coracoacromial ligament direction is projected more vertically from its origin in the undersurface of the acromion toward the coracoid. A more vertical ligament would reduce the subacromial space and potentially increase the contact of the lateral band of the coracoacromial ligament to the rotator cuff even though this hypothesis needs to be confirmed by further anatomical studies. Patients included in this study presented a normal coracohumeral distance meaning that coracoid impingement syndrome was not the reason for cuff symptoms.
This study has some limitations. First, the patients’ cervical and thoracic spine morphology or position during the CT scan may have influenced the position of the scapula and potentially modified the coracohumeral distance. However, if the scapula is displaced anteriorly while lying in the CT table, the humerus should move in accordance with the scapula due to passive stabilizers. While it might be argued that this limitation would have been an issue in the instability subgroup, the absence of significant difference for this parameter between the control group (including only instability patients for this parameter) and the RCT indicates that this has not been a significant limitation. Second, the coracoacromial ligament has not been directly measured. However, it is reasonable to assume a certain orientation of the ligament if the attachment site is evaluated. Third, not all the factors potentially related to RCT have been evaluated in the present study. Therefore, the influence of these factors on our results cannot be completely discarded.
Many morphological changes of the subacromial arch can favor the progression of the degenerative changes of the rotator cuff but little attention has been paid to the coracoid morphology as being part of the subacromial arch despite the fact that the coracoacromial ligament orientation depends on the coracoid morphology. Better understanding of all the factors implicated in RCTs may help to improve the management of this condition.
Conclusions
Patients with RCT present a reduced coracoid body–glenoid surface, coracoid tip–glenoid surface, and coracoid body–coracoid tip angles compared to control patients without RCT. A reduced angle may reduce the subacromial space by projecting the coracoacromial ligament more vertically, favoring RCT development.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.