
Abstract
Purpose:
The purpose of this study was to investigate the relationship between the superior capsule tear patterns and synovitis with subacromial pathologies, such as bursal-sided rotator cuff tear and subacromial impingement syndrome.
Methods:
Fifty patients who underwent arthroscopic treatment for isolated bursal-sided tear were included in the study. Fifty more patients who underwent arthroscopic treatment for isolated Superior Labrum Anterior Posterior (SLAP) 2 lesion without pathology in the rotator cuff were included in the control group. Firstly, superior capsule tear and common synovitis on the rotator cable were assessed during glenohumeral joint examination. Coracoacromial Ligament (CAL) degeneration grading was performed according to the Royal Berkshire Hospital classification. Bursal-sided partial tear grading was done using Ellman classification. Whether or not there was a relationship between synovitis, classic capsule tear, plus reverse flap capsule tear, and partial bursal-sided tear existence.
Results:
There were 21 patients with reverse flap capsule tear in the study group and 3 patients in the control group. In addition, there were 13 patients with synovitis in the study group and 4 in the control group. Compared to the control group, there was also a significant positive correlation in the presence of both synovitis and reverse flap capsule tear with the presence of bursal-sided tear in the study group (p = 0.000). There was, however, no significant difference between the presence of classical capsule tear and the presence of bursal-sided tear (p = 0.485).
Conclusion:
This study shows that the presence of reverse flap capsule tear and synovitis was associated with partial bursal-sided tears. Therefore, if the reverse flap capsule tear or synovitis is detected in the superior capsule, the rotator cuff should be evaluated in more detail during subacromial bursoscopy in order not to miss a bursal-sided partial cuff tear.
Keywords
Introduction
Partial rotator cuff tears are more common causes of shoulder pain and dysfunction compared to full-thickness tears. 1 Although the rate of progression in the tear dimensions is lower than full-thickness tears, the fact that it is more painful makes it clinically important. 2 The clinical approach depends on the age of the patient, the presence of a history of trauma, the severity of the symptoms, and the accompanying pathologies. 2 –4 There are three types of partial rotator cuff tears: articular, intratendinous, and bursal-sided tears with different etiologies. 5,6 Arthroscopic repair is preferred for symptomatic partial rotator cuff tears that do not respond to conservative treatment for 3–6 months. 3
Histological studies have shown that the rotator cuff is composed of five layers. 7 These layers are coracohumeral ligament (superficial), supraspinatus and infraspinatus tendons, transverse band (deep coracohumeral ligament), and capsule, respectively, from the bursal side to the articular side. Cadaveric dissections have also shown that 4–5 mm length of the rotator cuff footprint at the greater tuberosity is capsular insertion (Figure 1). 8

Cadaver dissection study investigating the capsular insertion side on tuberculum majus (unpublished data). (a) Capsule and humeral head. (b) The capsule is dissected. (c) and (d) Capsule adhesion site.
Capsular tears on the articular side of the rotator cuff are easily evaluated during arthroscopic glenohumeral examination. These tears, which we usually call “classic capsular tears,” are close to the base of the rotator cable (Figure 2). However, we have observed that some tears are different from classic capsular tears whose base of the capsular tear is close to the footprint, which we have defined as “reverse flap capsular tear” (Figure 2). In practice, we have noticed that this capsular tear pattern may be related to the bursal-sided partial rotator cuff tear. As far as we know, glenohumeral joint predictors for a bursal-sided partial rotator cuff tears have not been investigated previously in the literature.

Arthroscopic images of capsular tears from different patients. (a and b) Classical capsule tears. (c and d) Reverse flap capsule tears.
The purpose of this study was to investigate the relationship between the superior capsule tear patterns and synovitis with subacromial pathologies, such as bursal-sided rotator cuff tear and subacromial impingement syndrome. Our hypothesis was that the reverse flap capsule tear might be a sign for bursal-sided tears.
Patients and method
Clinical and digital video data from our institutional archive between January 2008 and July 2015 were retrospectively evaluated. If isolated bursal face partial tear was detected in the examination, it was included in the study. Although the data of patients were collected prospectively, the evaluation was made retrospectively. The presence of subscapularis or infraspinatus rupture, shoulder instability, Superior Labrum Anterior Posterior (SLAP) lesion, biceps rupture/instability, previous shoulder surgery, and adhesive shoulder capsulitis history was determined as exclusion criteria.
Fifty patients who underwent arthroscopic treatment for isolated bursal-sided tear were included in the study. Fifty more patients who underwent arthroscopic treatment for isolated SLAP 2 lesion without pathology in the rotator cuff were included in the control group. The reason for choosing patients with isolated SLAP lesion as a control group was to constitute a group with intact rotator cuff and to match the mean age in two groups since these two entities are suffered from in similar age groups. The patients’ operation dates were taken into consideration while selecting the patients to be included in the study. All of the patients had a history of failed conservative treatment (active surveillance, oral pain medication, steroid or tenoxicam injection, and physiotherapy) and persistent shoulder pain before the surgery at least 6 months.
Surgical technique
All of the arthroscopic surgeries were performed by the senior surgeon of this study. General anesthesia with or without an interscalene block or a single interscalene block was performed on the patients. The position during the procedure was standard lateral in which patients were allowed to rotate 30° posteriorly, thus placing the glenoid fossa parallel to the floor. The standard posterior portal was used for the initial examination of the shoulders. The procedures were performed with a 30-rigid arthroscope. Firstly, superior capsule tear and common synovitis on the rotator cable were assessed during glenohumeral joint examination. If the base of the tear was close to the rotator cable, it was recorded as classic capsule tear (Figure 2(a) and (b)). However, if the base of the tear was close to the rotator cuff footprint, it was recorded as reverse flap capsule tear (Figure 2(c) and (d)). The presence of synovitis was confirmed only if half of the rotator crescent surface was covered with hypertrophic synovitis tissue (Figure 3).

Arthroscopic images of superior capsule synovitis findings at the rotator cable from different patients.
Coracoacromial Ligament (CAL) degeneration grading was performed according to the Royal Berkshire Hospital classification. 9 Bursal-sided partial tear grading was done using Ellman classification. 10 Whether or not there was a relationship between synovitis, classic capsule tear, plus reverse flap capsule tear and partial bursal-sided tear existence, partial bursal tear grade, and CAL degeneration grade was investigated.
Statistical analysis
Statistical analysis of demographic data, findings on superior capsule, the degree of CAL degeneration, and the degree of bursal-sided partial tear were made by using SPSS/PC (version 18.0 for Windows; SPSS Inc, Chicago, Illinois, USA). All assessments were performed by two different researchers. The Pearson χ 2 test was used to analyze the relationship between the findings of superior capsule and the presence of bursal-sided partial tear and also to analyze the relationship between the findings of superior capsule and the degree of CAL degeneration and degree of bursal-sided partial tear. Since the groups were homogeneous and normally distributed, the study and control groups were compared in terms of mean age by t-test. Significance was set at 0.05 with 95% confidence intervals. The power analysis was performed for detecting an adequate patient number for groups. It is needed a simple size of 50 patients to be able to reject the null hypothesis with a type 1 error set at 0.05 and to show significant power greater than 80% for all the variables tested.
Results
A total of 3177 patients who underwent shoulder arthroscopy in our clinic were examined retrospectively. After the power analysis, 50 patients were included in the study group and 50 patients were included in the control group, according to the patient’s operation order.
The mean age of the patients at the time of surgery was 43.1 years (37–51). The average age of the patients was 44.6 ± 4.1 years with bursal-sided tears and 41.9 ± 4.4 years with SLAP 2 lesions. There was no significant difference between the study and control groups in terms of age, gender, and dominant side (Table 1).
Demographic characteristics of patients.

F: female; M: male; yr: year; SD: standard deviation.
There were 21 patients with reverse flap capsule tear in the study group and 3 patients in the control group. In addition, there were 13 patients with synovitis in the study group and 4 in the control group. Compared to the control group, there was also a significant positive correlation in the presence of both synovitis and reverse flap capsule tear with the presence of bursal-sided tear in the study group (p = 0.00; Table 2). The sensitivity and specificity of the presence of reverse flap capsular tear as a sign of bursal-sided tears were 87.5 and 61.8%, respectively. There was also no significant difference between the presence of classical capsule tear and the presence of bursal-sided tear (p = 0.485; Table 2).
The relationship between articular-sided capsule findings and bursal-sided tears.

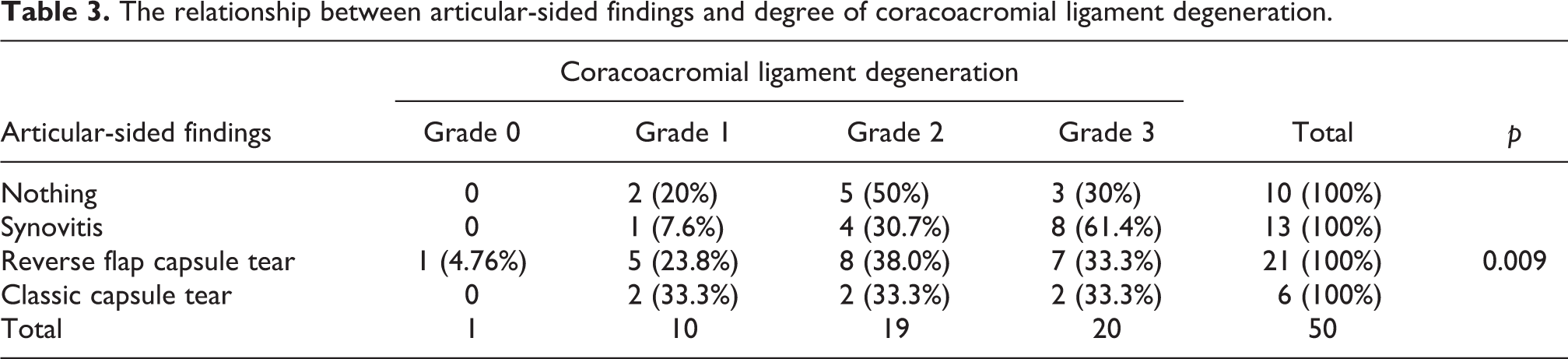
There was 1 patient with grade 0 (2%), 10 patients with grade 1 (20%), 19 patients with grade 2 (38%), and 20 patients with grade 3 (40%) CAL degeneration. There was no significant difference between articular-sided findings and degree of CAL degeneration (p = 0.09; Table 3).
The relationship between articular-sided findings and degree of coracoacromial ligament degeneration.
There were 20 patients with grade 2 (40%) and 30 patients with grade 3 (60%) bursal-sided partial tear according to the Ellman’s classification. Also, there was no significant difference between the articular-sided findings and the degree of bursal-sided tear (p = 0.881; Table 4).
The relationship between articular-sided findings and degree of bursal-sided tear.

Discussion
In histological studies, it has been shown that the rotator cuff consists of five layers and that these five layers are intertwined like the fingers of two hands union together. 7 –11 The fact that the layers are so intertwined with each other formed the idea that the changes in the capsule tissue on the articular side could give information about bursal-sided tears. In this study, we investigated superior capsular findings like the classic or reverse flap capsule tears and synovitis, which may exist in the articular side of the two groups of patients with bursal-sided tear and the control group.
The principle result of the study was that the frequency of synovitis and reverse flap capsule tear was found to be statistically higher in bursal-sided tear group than the control group. A hypothesis was thought to explain this capsular tear difference. The articular-sided tear starts from the footprint of the rotator cuff. The capsular flap separates from the footprint and creates the classic rotator cable-based capsular tear. On the contrary, bursal-sided tear starts from the rotator cuff (supraspinatus tendon) and progresses from the tendon to the rotator cable on the capsule. The torn tendon tissue accumulated at the level of the rotator cable creates pressure on the capsule. As a result of this pressure, reverse flap tear or diffuse synovitis occurs at the level of rotator cable (Figure 4). In addition, the presence and stage of CAL degeneration, which was found to accompany bursal-sided tears frequently, was also examined. There was no statistically significant relationship between the presence of capsular findings and both the grade of bursal-sided tear and the grade of CAL degeneration.

(a) Bursal-sided tear starts form supraspinatus tendon. Tear progresses from the tendon to the rotator cable on the capsule and the tear tendon tissue accumulated at the level of the rotator cable creates pressure on the capsule. As a result of this pressure, reverse flap tear occurs at the level of rotator cable. (b) On the contrary, articular-sided tears primarily begin with the adhesion of the capsule on the footprint.
Capsule tears do not exceed 3–5 mm thickness from the articular-sided tears. They usually have degenerative appearance. However, as the capsular attachment involves half of the anterior part of the supraspinatus footprint, tears located in this area should be carefully examined to distinguish capsular tears from supraspinatus tendon tear. 12 In addition, there are no studies about the progression of these capsular tears. However, since the capsule tissue has blood flow, the general approach is to protect the integrity of the tissue by local debridement of the tear. 8,13 In this study, debridement was applied as treatment to classic capsule tears as they composed less than 50% of the tendon. As far as we know, this is the first study defining reverse flap capsule tear pattern and relating them with bursal-sided tears.
Another articular-sided sign that is associated with bursal-sided tears is the presence of synovitis in the rotator crescent. Supraspinatus tendinopathy usually exists in the subacromial region. 14 In the joint, tenosynovitis is mostly seen on the biceps tendon. 15,16 Synovitis around the rotator interval may be related to the tears where the biceps tendon was involved. Moreover, a biceps instability caused by a lesion of the biceps pulley may also influence rupture patterns of the articular side of the rotator cuff. Therefore, patients with biceps rupture or instability were excluded from the study. Although there were radiological studies about the presence and grading of diffuse synovitis in glenohumeral joint, we could not find any arthroscopic evaluation in the literature. 17 Our study has shown us that the presence of rotator cable synovitis is a good finding that can be related to tears that may exceed 50% thickness of the rotator cable (Figure 3). Debridement was performed in the same manner as in capsule tears.
The fact that there is a significant difference in terms of both the reverse flap capsule rupture and the presence of diffuse synovitis in comparison with the control group supports the idea that these findings constitute a sign in the glenohumeral joint examination for the presence of bursal-sided tears. Advanced coracoacromial ligament degeneration is also associated with bursal-sided tears. 6,18 Although all of these findings were associated with bursal-sided tears, there was no significant correlation between the presence of a reverse flap tear and the presence of synovitis with coracoacromial ligament degeneration.
In the control group, four patients had synovitis and three patients had reverse flap. However, one of these seven patients had grade 1, four of them had grade 2, and two of them had grade 3 coracoacromial ligament degeneration. This situation suggests that impingement syndrome may have started to develop in these patients, but the bursal-sided rupture has not developed yet. And, that these patients may develop a bursal-sided tear in the future.
This study has defined two different arthroscopic findings accompanying bursal-sided tears for the first time in literature. However, there are some limitations of this study. The clinical results were not evaluated and the study was designed retrospectively, although the data were collected prospectively. The number of patients in the groups is slightly lower. Besides these limitations, the distribution of patients in both groups were homogenous.
Conclusion
This study shows that the presence of reverse flap capsule tear and synovitis was associated with partial bursal-sided tears. Therefore, if the reverse flap capsule tear or synovitis is detected in the superior capsule during the glenohumeral joint examination, the rotator cuff should be evaluated in more detail during subacromial bursoscopy in order not to miss a bursal-sided partial cuff tear.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.