
Abstract
Purpose:
It seems to be important to recognize bone health condition using a simple method in Japanese super-aged society. The aim of our study was to investigate whether grip and key pinch strength were associated with bone quality.
Methods:
Medical examinations were conducted of 337 adult residents (123 men, 214 women; average age of 64.7 years) of a mountain village. Bilateral grip and key pinch strength were measured. The sound of speed (SOS) of calcaneus was assessed using an ultrasound bone densitometer. Study participants were divided into non-osteoporotic and osteoporotic groups according to the relevant WHO classification to evaluate statistical significance by age-adjusted analysis. Stepwise linear regression was used to identify the predictor of SOS using the following factors as explanatory variables: age, height, weight BMI, grip and key pinch power strength in bilateral side. A P value of < .05 was regarded as statistically significant.
Results:
In age-adjusted analysis, significant associations were found between osteoporosis and BMI (OR 0.87, 95%CI 0.80–0.95), gender (OR 3.21, 95%CI 1.83–5.62), grip strength (right side:, OR 0.95, 95%CI 0.92–0.98; left side: OR 0.95, 95% CI 0.92–0.98) and key pinch strength (right side: OR 0.76, 95%CI 0.65–0.88; left side: OR 0.79, 95%CI 0.68–0.91). In stepwise linear regression, age and left key pinch strength were predictors of calcaneal SOS (age β coefficient = −0.46, P = .00; left key pinch strength β coefficient = 0.17, P = .0049).
Conclusions:
Key pinch strength assessment might be useful to predict calcaneal SOS in general population.
Introduction
Worldwide, the share of population of people 60 years of age or older increased from 9.2% in 1990 to 11.7% in 2013. It is expected to reach 21.1% by 2050: over two billion people. 1 Osteoporosis, which constitutes a major public health problem, is an age-related disease. Presuming a constant age-specific rate of fragility fracture related to osteoporosis in men and women, the incidence of hip fracture is estimated as reach 6.3 million in 2050. 2 Japan represents an unprecedented aging society. 3 According to population-based epidemiologic studies, an estimated 15 million people have osteoporosis in Japan, but only 20% of them are under treatment. 4 The most recent incidence rates of hip fracture in Japan were 5.1 in 10,000 men and 18.1 in 10,000 women in 2007. The number of patients is approximately 130 thousand, which is 2.8-fold higher than in the initial survey taken in1987. 2,4,5 It is important to elucidate bone health to prevent osteoporosis in the general population. Dual-emission X-ray absorptiometry is the gold standard for bone mineral density (BMD) assessment and diagnosis of osteoporosis. 6 However, this method is associated with high costs and few facilities. 7 Quantitative ultrasound (QUS) of the calcaneus, which is inexpensive and free of radiation emissions, rapidly provides a risk assessment of fragility fracture caused by osteoporosis. 6 –11 An earlier study demonstrated that both QUS and BMD evaluations were related strongly and equally with risk factors for osteoporosis. 12 Furthermore, QUS devices are compact and portable, requiring only about 10 s to measure the speed of sound (SOS) of calcaneus. In fact, QUS is suitable to assess bone health in field work. Grip strength is an important parameter related to functional integrity of the hand. Grip strength measurement is a simple and inexpensive method to assess forearm and hand function. Several reports have described the relation between BMD and osteoporosis and grip strength. 13 –18 Recognizing bone health using a simple method such as grip strength assessment is important. Few reports in the relevant literature have described an association between grip and key pinch strength and osteoporosis and the QUS of calcaneus. For residents of a mountain village in Japan, this study aimed to investigate the relation between the SOS of calcaneus and grip and key pinch power strength.
Materials and methods
Local medical examinations intended for early detection of cancer and for prevention of lifestyle-related diseases were conducted for residents of a mountain village in Japan, where agroforestry and tourism are the main industries. For this study, 337 people (123 men and 214 women; average 64.7 years of age, range 28–90; Table 1) were selected randomly. Height was measured using a digital height meter (A&D Co. Ltd, Tokyo, Japan). Body mass index (BMI) was calculated as weight in kilograms divided by height in meters squared. After they had been informed of the study protocol and had been told that their data would be published, all participants gave their consent to participate in this study. This study was approved by the regional ethics board.
Grip and key pinch strength data for age-groups.a
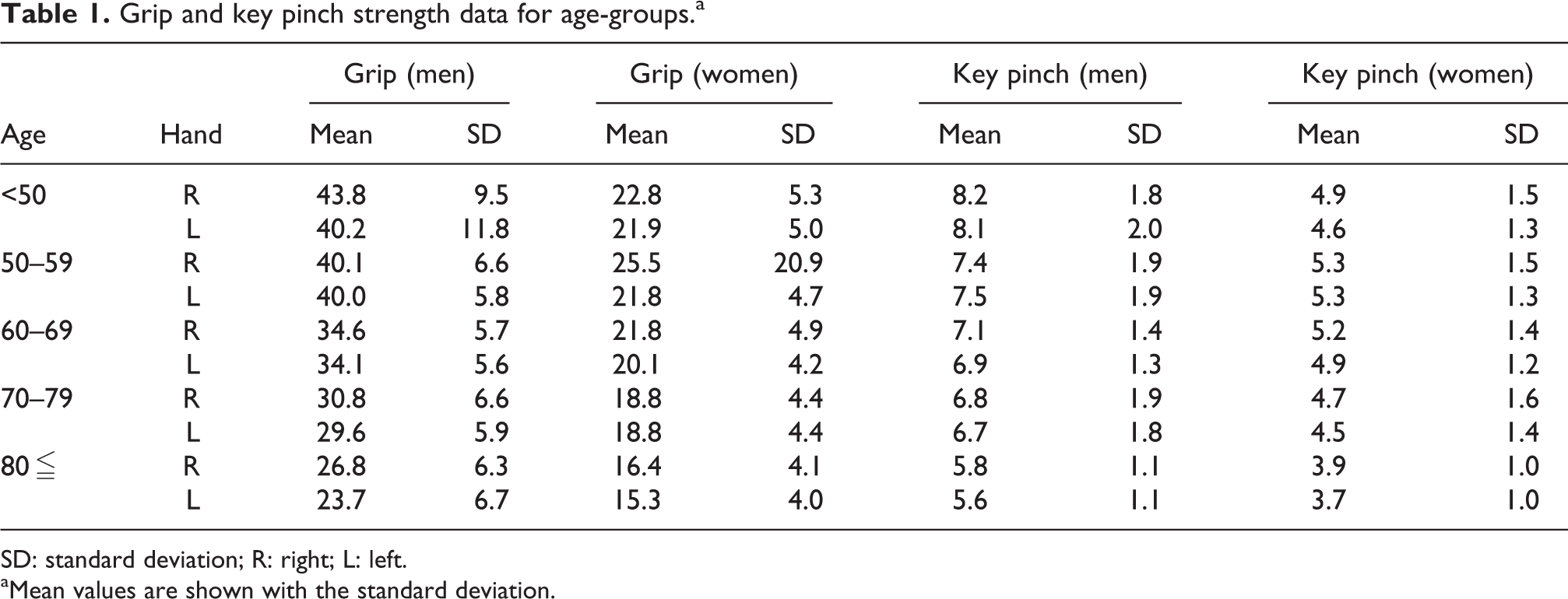
SD: standard deviation; R: right; L: left.
aMean values are shown with the standard deviation.
A digital dynamometer (Takei Scientific Instruments Co., Tokyo, Japan) was used to measure grip strength and a pinch gauge (MG-4320NC pinch gauge; B & L, Santa Ana, California, United States) to measure key pinch of both sides. Grip testing was conducted using the standardized position recommended by the American Society of Hand Therapists. Participants were seated with the shoulder in adduction and neutral rotation, elbow flexed at 90°, forearm in neutral position, and wrist between 0° and 30° of extension and 0° and 15° of ulnar deviation. Pinch testing was performed with the shoulder, elbow, forearm, and wrist in neutral position. We conducted key pinch tests. Key pinch is the thumb pad to the lateral aspect of middle phalanx of index finger. For each grip and pinch test, two measurements were performed in the bilateral side. All tests were administered by a single orthopedic surgeon. The exclusion criteria of this study were (1) participants who had prior operation in bilateral upper extremity, (2) participants who had pain of bilateral upper extremity, and (3) participants who took medications that affect bone metabolism as bisphosphonates and glucocorticoids.
Measurement of calcaneus SOS
The SOS of calcaneus bone of right side was measured using an ultrasound bone densitometer (Furuno Electric Co. Ltd, Nishinomiya, Japan). The size and weight of this device allow it to be carried to any location for measurements. This device has a unique sensor to compensate for the participant’s heel temperature. This function provides accurate SOS measurements. Participants place their right feet on the foot plate, which can be adjusted to accommodate any foot size. Ultrasound waves are conveyed from one transducer through the calcaneus and the other transducer. The T-score was calculated from the manufacture-specific SOS reference population database. This machine was calibrated with its physical phantom. All measurements were taken by the same orthopedic surgeon.
Statistical analyses
Descriptive statistics were performed for all direct measurements. Spearman’s rank correlation coefficient was calculated to elucidate the relation between SOS and age, height, weight, BMI, left and right grip, and key pinch strength. Univariate and age-adjusted analysis were used to evaluate statistical significance for participants with osteoporosis and without osteoporosis. Osteoporosis was defined as a T-score below −2.5 × standard deviation (SD), according to the definition of World Health Organization (WHO). 6 Stepwise regression analysis was used to evaluate factors that might affect calcaneal SOS such as age, weight, height, BMI, right and left grip, and key pinch strength. Statistical analyses were conducted with SPSS 21.0 software for Windows. A p value of <0.05 was regarded as statistically significant.
Results
In both groups (men and women), the grip strength decreased with age (Table 1). In men, key pinch strength decreased as age increased, but in women, taking the ages below 50 years as baseline, bilateral key pinch strength showed the most drastic increase during the ages of 50–60 years (Table 1). The calcaneal SOS decreased as age increased in both men and women (Table 2). In men, age was inversely correlated with calcaneus SOS. Weight, height, BMI, bilateral grip strength, and key pinch strength were positively correlated with calcaneus SOS. In women, age was inversely correlated with calcaneus SOS. Weight, height, bilateral grip strength, and key pinch strength were positively correlated with calcaneus SOS. In all participants, age was inversely correlated with calcaneus SOS. Weight, height, BMI, bilateral grip strength, and key pinch strength were positively correlated with calcaneus SOS (Table 3).
Calcaneal SOS for age-groups.a
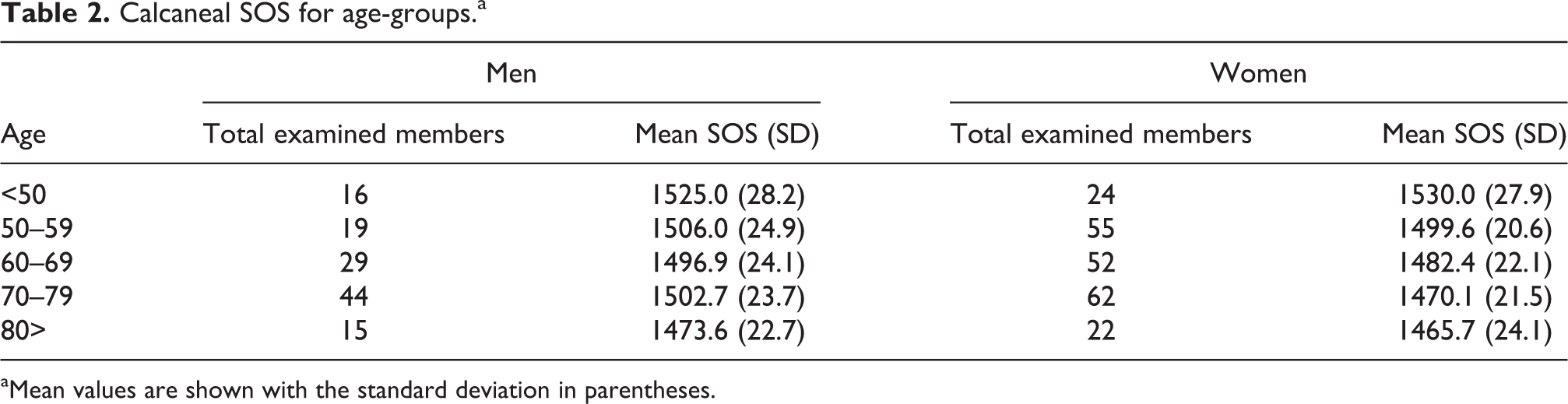
aMean values are shown with the standard deviation in parentheses.
Correlation between calcaneus SOS and grip, key pinch strength.
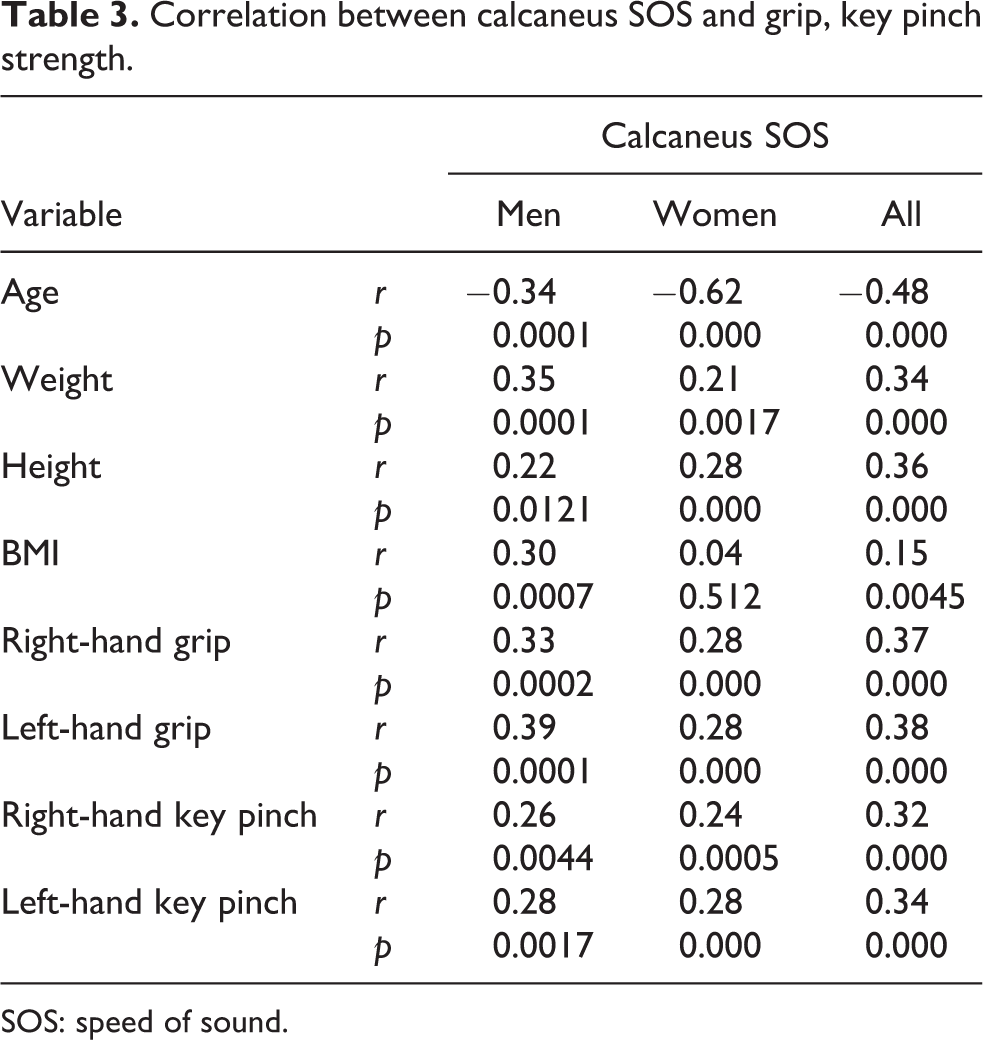
SOS: speed of sound.
The T-score was calculated from the manufacturer-specific SOS reference population database. Osteoporosis was defined as a T-score lower than −2.5 × SD according to the definition of WHO. 6 Participants were divided into groups according to their calcaneal SOS: osteoporosis (n = 118) and non-osteoporosis (n = 219). The respective mean (SD) of SOS values of participants with and without osteoporosis were 1461.4 (13.5) and 1508.8 (21.9). The average age (SD) of participants with osteoporosis was 66.7 years. The prevalence of osteoporosis increased with age. The prevalence of osteoporosis was significantly higher among women than among men in univariate and age-adjusted analysis. Regarding anthropometric variables, BMI was associated significantly with osteoporosis in both univariate analysis and age-adjusted analysis; however, weight and height were not related with osteoporosis. Both univariate and age-adjusted analysis showed that key pinch strength and bilateral grip strength are significantly related to osteoporosis (Table 4). Stepwise linear regression analysis was performed to evaluate factors that might affect calcaneal SOS such as age, weight, height, BMI, right and left grip, and key pinch strength. Age (β coefficient = −0.46, p = 0.00) and left-hand key pinch strength (β coefficient = 0.17, p = 0.0049) were selected as significant predictors of calcaneal SOS. They explained 35% of the variation in calcaneal SOS.
Variable data of study participants with and without osteoporosis.a

CI: confidence interval.
aMean values are shown with the standard deviation in parentheses. Odds ratios were calculated using univariate and age-adjusted analysis. A one-unit change in the explanatory variable increases the odds of having osteoporosis by a factor of the odds ratio.
Discussion
We used QUS of calcaneus to assess bone quality in medical examination in place of measuring lumbar and hip BMD as recommended by WHO for diagnosis of osteoporosis. Prior reports of the literature have described that QUS of calcaneus is useful to assess bone health. 19 –24 SOS of the calcaneus has shown significant positive correlation with BMD. 25,26 Takaishi et al. validated the relation between lumbar spine BMD measured using dual X-ray absorptiometry and SOS of calcaneus measured using ultrasound bone densitometry. 23 They reported a significant positive correlation between lumbar spine BMD and SOS of calcaneus (r = 0.62).
Previous studies have shown a significant relation between BMD and the risk of fragility fracture related with osteoporosis and grip strength. 13 –18,27 Dixon et al. examined the association between low grip strength BMD at the hip and spine and the medical history of vertebral fracture in middle-aged and elderly people, 1265 men and 1380 women, in a cross-sectional study. 27 Their data demonstrated that low grip strength is a significant marker of low hip and spine BMD. It is related with an increased risk of incident vertebral fracture. Furthermore, Cheung et al. assessed a prospective cohort with 882 men and 820 women to elucidate the risk of fragility fracture related with osteoporosis. They used a score for the standardized hand grip strength T-score (value-young reference mean/young reference standard deviation). Their multivariate analysis with adjustment of clinical risk factor including age, sex, BMI, history of fall, presence of diabetes, current smoking and drinking, physical activity and hand grip T-score, and femoral neck BMD T-score revealed 1.24-fold increased odds for fracture with decrease in hand grip T-score. 28 However, few reports describe the SOS of calcaneus and grip strength. Furthermore, we tried to investigate other easy muscle power assessment-related bone health, except for grip strength. In grip strength assessment, extrinsic muscles of the forearm consisted of flexor digitorum profundus and superficial muscles are apparently evaluated mainly without reflecting thumb muscle power. The thumb is the most important finger for hand function in daily life activities. Angust et al. evaluated the predictive power of cofactors related with normative grip and key pinch strength for a general population. 29 They reported five cofactors as highly accurate predictors of normative grip and key pinch strength: sex, age, body, height, categorized occupational demand on the hand, and body weight. In an earlier study, we investigated the associations between normative grip strength and key, palmar, and tip pinch strength in high school students. 30 Results showed that tip, palmar, and key pinch strength are significant predictors of grip strength on the dominant side. Grip strength reflecting the extrinsic muscle of forearm is closely related to pinch strength, reflecting the intrinsic muscles of the hand.
Key pinch strength, operated mainly by adductor pollicis muscle of the hand intrinsic muscle, was assessed to ascertain whether key pinch strength assessment is related with bone health condition or not. Results show that right and left grip strength values are positively correlated with right and left key pinch strength values. Bilateral grip and key pinch strength are positively correlated with calcaneal SOS in men and women. Furthermore, QUS assessment of calcaneus with age-adjusted analysis shows that bilateral grip and key pinch strength in participants with osteoporosis were significantly lower than those of participants without osteoporosis. Key pinch assessment might suggest related factors of bone health, as does hand grip power assessment.
Earlier reports have described predictors of calcaneal SOS. 20,22 Hien et al. assessed the prevalence and related factors of osteoporosis using a QUS device we used with older Vietnamese women. From multiple logistic regression analysis, they reported that variables related with low SOS of calcaneus were age, menopause, educational level, lifelong occupation, recreational weight-bearing exercise, number of birth, and height. 20 Chin et al. examined the influences of age, lifestyle factors and body anthropometry on the calcaneal SOS in Malaysian men using a QUS machine of the same type we used. In their study, age, height, physical activity, weight, and body fat percentage for participants were significant predictors for calcaneal SOS. 22 In our study, stepwise linear regression analysis was performed to evaluate factors that might affect calcaneal SOS such as age, weight, height, BMI, right and left grip, and key pinch strength. Age and left-hand key pinch strength were selected as significant predictors of calcaneal SOS. Different assessment variables might suggest different predictors of calcaneal SOS. However, few studies have assessed the relations among calcaneal SOS and grip and key pinch strength. Key pinch strength assessment might be useful to estimate bone health.
Our study had several limitations. The sample size was small, particularly with respect to participants younger than 40 years. The small sample size might affect the statistical power for evaluation of the relation between grip and key pinch strength and calcaneal SOS. We were unable to assess the association between the hand dominance and grip and key pinch strength and calcaneal SOS. It is apparently more valuable to understand the relation between hand dominance and grip and key pinch power and SOS to assess bone quality. We were unable to investigate anthropometric variables such as muscle mass, fat mass, fat free mass, and muscle strength except grip and key pinch strength and physical activity. Rikkonen et al. investigated the relation between muscle strength, lean tissue distribution, and overall body composition and osteoporosis in postmenopausal women. They reported that grip strength and leg extension strength were significantly associated with femoral neck osteoporosis in multiple logistic regression analysis. 18 Yung et al. reported that weight-bearing exercise such as soccer and dancing affected maximization of peak bone mass compared non-weight-bearing exercise such as swimming. 24 We were unable to assess the relation between calcaneal SOS and smoking and alcohol consumption and lifestyle. Sritara et al. reported that low-to-moderate alcohol consumption was related independently with higher BMD at lumbar, femoral neck, and total hip and that smoking was independently associated with lower BMD at the lumbar spine in men of Thailand. 31 Further studies should be performed to elucidate the QUS assessment and grip and pinch strength with multiple-related factors in the general population.
Conclusions
We evaluated the relation the calcaneal SOS and grip, key pinch strength, and anthropometric variables in a general population. For all participants, age was correlated inversely with calcaneus SOS. Weight, height, BMI, bilateral grip strength, and key pinch strength were positively correlated with calcaneus SOS. Dividing the participants into osteoporosis and non-osteoporosis groups determined by QUS, significant associations were found between osteoporosis and BMI, gender, and bilateral grip strength and key pinch strength in age-adjusted analysis. In stepwise logistic regression, age and left key pinch strength were found to be predictors of calcaneal SOS. Key pinch strength assessment might be useful to predict calcaneal SOS in a general population.
Footnotes
Acknowledgment
The authors thank the participants and the medical staff and public health nurses of the regional health center for their assistance and support in this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.