
Abstract
Purpose:
Pelvic vascular injury is a serious complication associated with acetabular component setting with screw fixation in cementless total hip arthroplasty (THA). In this study, we investigated the safety zone for acetabular component setting with screw fixation in cementless THA as a means to prevent pelvic vascular injury.
Methods:
Thirty left hip joints of Japanese cadavers (11 males and 19 females) were analyzed. We used a hemispherical measuring cup with 52 guide holes designed to allow vertical insertion of a Kirschner wire. After the measuring cup was placed on the acetabulum, the Kirschner wire was inserted from each guide hole to examine the anatomical relationship between the acetabulum and the pelvic vessels. We calculated the frequency of pelvic vessel punctures and measured the distance from the acetabular surface to the pelvic vessels at each guide hole.
Results:
Our findings revealed that pelvic vessels do not exist in certain parts of the posterior area of the acetabulum. Furthermore, in this area, intrapelvic vessels are either lacking or located at a distance ≥31 mm from the surface of the acetabulum.
Conclusion:
The posterior area of the acetabulum, excluding its central portion, appeared to be the safety zone for acetabular screw fixation in Japanese cadavers.
Introduction
Pelvic vascular injury associated with acetabular screw fixation is one of the serious complications of cementless total hip arthroplasty (THA). 1 –3 In the event of pelvic vascular injury, treatment for achieving hemostasis may be delayed because the injury is not accompanied by hemorrhage that is visible in the surgical field and massive hemorrhage, which may lead to death, occurs in the retroperitoneal space. 2,3 As most pelvic vessels are located in the pelvic cavity, it is not possible to confirm their location intraoperatively during cementless THA. Therefore, to prevent pelvic vascular injury and to perform cementless THA safely, it is necessary to estimate the course and location of the pelvic vessels posterior to the acetabulum during surgery and to place the acetabular screws in the so-called safety area. 1,4
Previous studies conducted in Western countries on the course of the pelvic vessels and the distance from the acetabular surface to the pelvic vessels have indicated that the posterior area of the acetabulum is the safety zone for screw fixation. 5 However, to date, no studies have been conducted to determine the safety zone for screw fixation in the Asian population. The thickness of the pelvic bone and the distance to the pelvic vessels may differ in the Asian population compared to Caucasian population, because of their relatively small body size, particularly the short height. Therefore, application of these findings from overseas reports to the Asian population without any adjustment may involve the risk of pelvic vascular injury.
The aims of this study were to perform an anatomical examination of the course of the pelvic vessels as viewed from the acetabular surface and to identify the safety zone for acetabular implant screw fixation in cementless THA in the Asian population.
Materials and methods
Thirty left hip joints from Japanese cadavers (11 males and 19 females) were analyzed in the present study. The most common age-group was the ninth decade of life (mean age, 84.5 years; range, 58–98 years); the mean height was 154 cm (range, 137–170 cm); and the mean weight was 36.8 kg (range, 23–63 kg). Cadavers with a history of surgery for hip osteoarthritis or intrapelvic viscera were excluded from this study, as surgery could have changed the relationship between the acetabulum and the pelvic vessels remarkably.
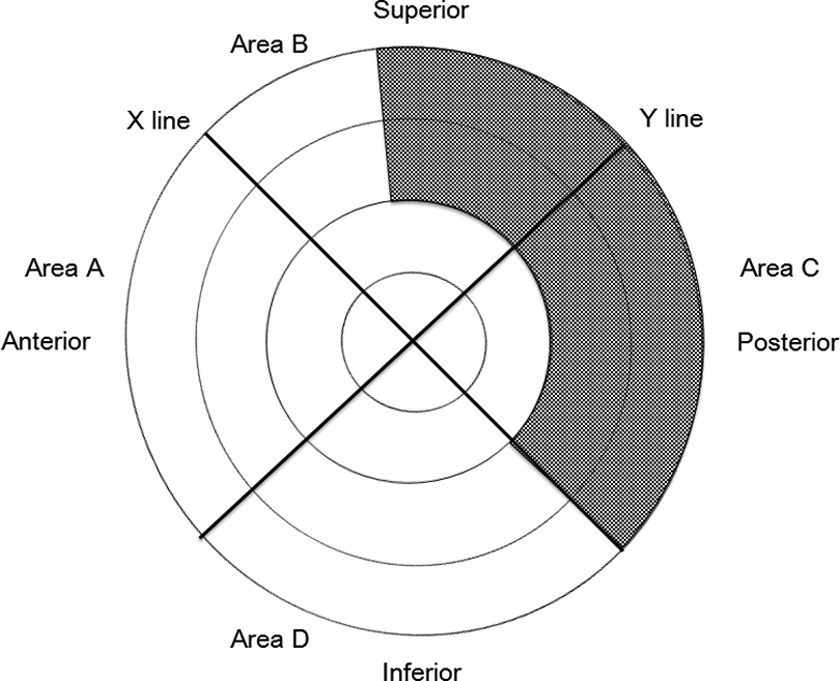
After dislocation of the left femoral head, the acetabular cartilage was removed. A hemispherical measuring cup corresponding to the acetabular diameter was then placed on the acetabulum (Figure 1). For placement of the measuring cup, the lateral opening angle was set at 45°, and the anterior opening angle was matched with the anteversion angle of the acetabulum of the pelvis. The measuring cup was designed to have 52 guide holes for inserting a Kirschner wire vertically into the cup surface (Figure 1). After the measuring cup was placed on the acetabulum, the Kirschner wire was inserted from each guide hole to examine the anatomical positional relationship between the acetabulum and the pelvic vessels. Among the pelvic vessels, the external iliac artery, obturator artery, superior gluteal artery, inferior gluteal artery, and external iliac vein were examined. The obturator, superior gluteal, and inferior gluteal veins were excluded from the examination because their locations are difficult to confirm in a cadaver. The acetabulum was divided into four quadrants by a line parallel to the Roser–Nelaton line and crossing the center of the acetabulum (X-line) and a line vertical to the X-line and crossing the center (Y-line). The anterior quadrant of the acetabulum was designated as area A, the superior quadrant as area B, the posterior quadrant as area C, and the inferior quadrant as area D (Figure 1). First, we calculated the frequency of the pelvic vessel puncture occurrence and prepared a distribution map of this frequency as viewed from the acetabular surface when the Kirschner wire was inserted into each guide hole of the measuring cup. Next, the distribution of the pelvic vessels, as viewed from the acetabular surface, was examined for each specimen, and a distribution map of the pelvic vessels was prepared. Parts of the posterior acetabular area with even one pelvic vessel and in only one of the target pelvises were considered as parts with pelvic vessels. Finally, the distance from the acetabular surface to a pelvic vessel was measured at each guide hole in each target pelvis, and a distribution map of the minimal distance at each guide hole was prepared.
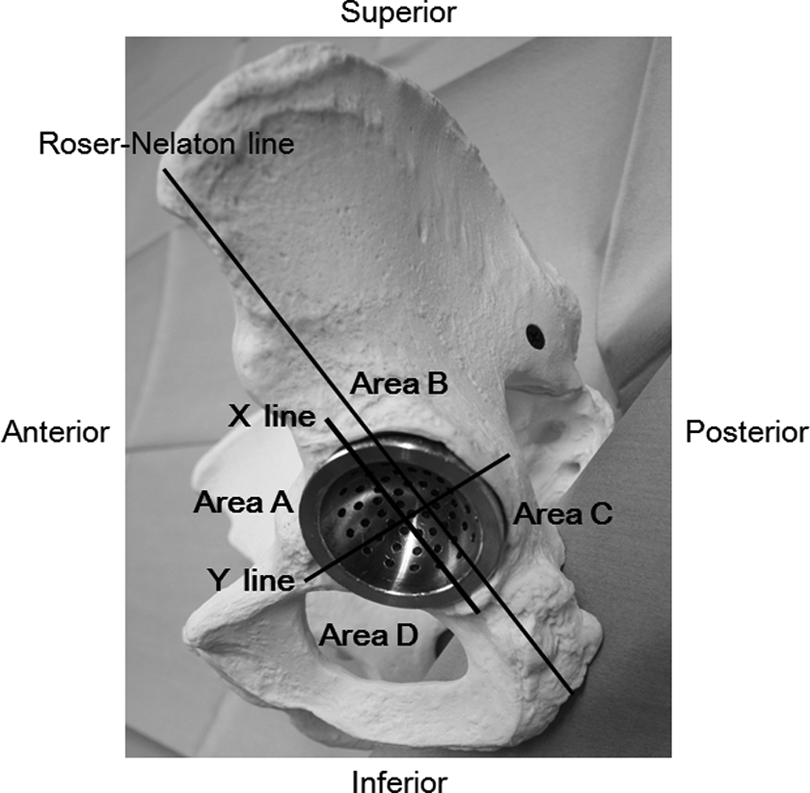
Acetabular measuring cup and acetabular areas. The acetabular measuring cup has 52 guide holes for inserting a Kirschner wire. X-line: A line parallel to the Roser–Nelaton line and crossing the center of the acetabulum. Y-line: A line vertical to the X-line and crossing the center of the acetabulum. The anterior quadrant of the acetabulum was designated as area A, the superior quadrant as area B, the posterior quadrant as area C, and the inferior quadrant as area D.
Results
Frequency of pelvic vessel punctures
The frequency of pelvic vessel punctures in the anterior aspect of area A was >50%, especially it was >75% in the central part of this aspect (Figure 2). The frequency of a part of area D exceeded 50%. Although the overall frequencies in areas B and C were low, parts with 0% frequency were small. Thus, in only few parts, no pelvic vessel will be damaged, and the possibility of vessel damage is high in the anterior acetabular area.

Frequency of pelvic vessel puncture occurrence. The frequency of pelvic vessel punctures was high in areas A and D, especially in the anterior portion of area A.
Distribution of the pelvic vessels as viewed from the acetabular surface
The external iliac artery and vein were found in the region from the anterior part of area B to almost the entire area A (Figure 3). The obturator artery was found in the entire area D, excluding the posterior area, and the central acetabular parts of areas A and B. The main trunk of the superior gluteal artery was present in the superior part of area B and the area at the border between areas B and C near the center of the acetabulum. The peripheral portion of the superior gluteal artery was found in the posterior part of areas B and C. The inferior gluteal artery was found in the area that was at the border between areas B and C and near the center of the acetabulum. However, the superior and inferior gluteal arteries existed far from the acetabular surface even around the center of the acetabulum, and the distance between the surface and the arteries was ≥31 mm. These facts revealed that there are no pelvic vessels in a small part of the superior aspect of area B and in a part of area C. The mean distance to the main pelvic vessels in each area is shown in Table 1.

Distribution of the pelvic vessels and distance from the acetabular surface to them. The external iliac artery and vein are distributed in the anterior acetabular area, and the obturator artery is distributed from the central to the inferior acetabular areas. The superior gluteal artery is distributed from the superior to posterior acetabular areas, and the inferior gluteal artery is distributed in the posterior part of the central acetabular area. The external iliac artery, the external iliac vein, and the obturator artery tend to be found close to the cartilaginous callus. Conversely, the superior gluteal artery is found relatively far from the subchondral bone. Areas where the pelvic vessels will not be punctured with the consideration of an error in the placement angle of the acetabular implant (asterisks). This was determined from the area without any pelvic vessels in the region posterior to the acetabulum, with the consideration of an error of 15°. Although vessels existed in a part of this region, this part was extremely small.
The mean distance to the main pelvic vessels in each area.a

aMean distance ± standard deviation (mm).
Minimum distance from the acetabular surface to the pelvic vessels
In areas A and D, where the external iliac artery, the external iliac vein, and the obturator artery exist, and the area near the center of the acetabulum in Area C, where the obturator artery exists, the minimal distance from the acetabular surface to the pelvic vessels was ≤20 mm at all points in the parts with the vessels (Figure 3). In area B and parts of area C where the superior and inferior gluteal arteries exist, the minimal distance to the pelvic vessels was 31 mm. Thus, the areas where the pelvic vessels are located far from the posterior acetabulum (even if they are found) are area B, excluding the central acetabular area, and the posterior part of area C.
Discussion
Pelvic vascular injury is one of the serious complications of THA. 6 These injuries are commonly caused during the insertion of acetabular screws, by the tip of the retractor as it is approaching the acetabulum and by the acetabular reamer. 4,7 –14 The incidence rate of these injuries ranges from 0.2% to 0.3%. 6 The risk of vascular injury is higher in the anterior and central areas of the acetabulum, especially during acetabular screw fixation in cementless THA. 5,12 In this study, the pelvic vessels were punctured in the anterior acetabular area at a frequency ≥76%, and this result revealed that screw fixation in the anterior acetabular area may be complicated by a high incidence of pelvic vascular injury.
The most important requirements for establishment of the safety zone for acetabular screw fixation include the absence of pelvic vessels posterior to the acetabulum and a large distance from the acetabular surface to any potential vessels. In addition to these requirements, surgeons must consider several other factors and possibilities, including the arteriosclerotic status of the patient, any potential alterations in the vascular course due to variation, deformity of the acetabulum, and individual differences in pelvic morphology. Moreover, since the positions and procedures for implant placement vary for each patient and between each surgeon, acceptable ranges, as discussed below, should be considered when setting the safety zone for acetabular screw fixation.
The error in acetabular implant placement has been reported to be 4–15° in general and 2–7° under the concurrent use of a navigation system. 15 Thus, it is necessary to set a safety zone with the consideration of an error of approximately 15° at least, under the condition in which the acetabular implant is placed. The results of this study show that pelvic vessels do not exist in some parts of the posterior acetabular area. However, when a distribution map of the pelvic vessels is prepared with the consideration of an error of 15°, only small parts remain free of the vessels (Figure 3). Thus, if the safety zone for acetabular screw fixation is defined as the area posterior to the acetabulum where pelvic vessels do not exist, the safety zone would be almost nonexistent. However, if we focus on the area behind the acetabulum where pelvic vessels exist but are located at a large distance from the surface, the areas that satisfy this condition would be area B, excluding the central acetabular and anterior areas, and area C, excluding the central acetabular area. In cases of hip osteoarthritis, the distance from the acetabular surface to the pelvic vessels may be shortened because of disuse atrophy of the iliopsoas and internal obturator muscles. 1,6,14 Moreover, as there may be cases in which the distance to the pelvic vessels is even shorter owing to individual differences, it is necessary to set a safety zone with the consideration of acceptable ranges regarding the length of drills and screws to be used. The minimal distance to the pelvic vessels in the concerned area was 31 mm in the present study. Although no previous studies have reported the stability of screws used for acetabular cup fixation in THA, the use of screws measuring at least 15 mm in length is recommended in order to achieve stable acetabular cup fixation. In this study, the minimal distance to the pelvic vessels was 34 mm in the posterior acetabular area where the vessels existed but were far from the acetabular surface. Thus, acetabular screw fixation with screws and drills measuring 15–25 mm in area B, excluding the central acetabular area, and in the posterior part of area C can be considered safe (Figure 4).
Safety zone for screw fixation with screws measuring 25 mm or less, with the consideration of the error in the placement angle of the acetabular implant. The safety zone is determined from areas with the risk of puncturing the obturator and inferior gluteal arteries in the central area of the acetabulum, the external iliac artery and vein in the anterior area, and the obturator artery in the inferior area with the consideration of an error of approximately 15°.
In agreement with the results presented herein, previous studies investigating this topic in Western countries also concluded that the safety zone for screw fixation was located in areas B and C, excluding the central acetabular area. However, no studies have been conducted on the safety zone in the Asian population. According to these previous reports, the thickness of the pelvis in Caucasian subjects is 25–35 mm, which is significantly greater than the distance from the acetabular surface to the pelvic vessels determined in the present study. 2,3,12,14 This indicates that if the acetabular screw fixation was performed for the Asian population with drills and screws based on the length described in other populations, the pelvic vessels may be damaged. It appears that performing the procedure with shorter drills and screws based on the results of this study for the Asian population, whose body size is small, may prevent this risk. However, it should be noted that even the safety zone for the acetabular screw fixation identified in this study is associated with individual differences, tortuosity of vessels due to arteriosclerosis, and error in implant placement.
One of the limitations of this study is that the hip joints used in the present study were from Japanese cadavers without joint abnormalities. Since abnormalities of the hip joints may cause the abnormal anatomy of the pelvic vessels, additional anatomical study using the hip joints with articular disorder such as osteoarthritis or developmental dysplasia is needed in the future.
Conclusion
In this study, the safety zone for acetabular screw fixation in cementless THA was examined anatomically using 30 Japanese cadavers. The posterior acetabular area, excluding the central acetabular area, under the condition of using screws and drills measuring ≤25 mm, is the safety zone for the acetabular screw fixation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.