
Abstract
Purpose:
The purpose of this study was to report the long-term results of total hip arthroplasty (THA) for the treatment of ankylosed hip.
Methods:
Twenty-nine consecutive THAs were performed in 26 patients. The mean age of the patients at the time of the operation was 43.3 years (range, 19–69 years). We used cementless fixation in all hips and the mean duration of follow-up was 10.1 years (range, 4.5–20 years). Radiological evaluation of components, osteolysis, radiolucent lines and loosening were assessed. The Harris Hip Score (HHS), range of motion (ROM), limb-length discrepancy and walking capacity with or without any support were used preoperatively and at final follow-up for clinical evaluation. Survivorship analysis was conducted using the Kaplan–Meier method using second revision for any reason as the endpoint.
Results:
The mean HHS was 85.6 (range, 55–98) points and mean ROM was 110.5° for flexion. The mean limb-length discrepancy improved from 4.1 cm to 1.1 cm. Positive Trendelenburg sign was recorded in 31% of the patients and 24% of patients needed any support for walking postoperatively. We observed surgical complications related to abductor arm in 25% of the patients. Radiolucency on the acetabular side was seen on one or more zones in 15 patients (16 hips). One aseptic acetabular component loosening was observed. On the femoral side, 11 patients demonstrated non-progressive radiolucent lines and osteolysis around the stem was seen in four hips but there was no aseptic stem loosening. The Kaplan–Meier survival rate considering revision for any reason as the endpoint was 81.5%, for aseptic loosening 91.3%, for a worst-case scenario of 66.4% at 10 years.
Conclusion:
Cementless fixation showed good to excellent results at 10 years. Preoperative and postoperative abductor status of the patient is critical for patient satisfaction.
Introduction
Etiology of the ankylosis of the hip can be spontaneous or surgical. Spontaneously fused hips are usually sequela to several developmental or rheumatological diseases including developmental dysplasia of the hip, ankylosing spondylitis, systemic lupus erythematosus and juvenile rheumatoid arthritis or might be as well as post-traumatic (arthritis following acetabular or proximal femoral fractures) and sequela of septic arthritis. Whereas surgical fusion or arthrodesis was once considered as an alternative treatment to total hip arthroplasty (THA) to provide long-term pain relief and stabilization for end-stage arthrosis of the hip for selected patients who are younger (<40 years) and active patients. 1,2 However, painful degenerative changes in their lower back, ipsilateral knee and contralateral hip and gait pattern of the patient were the main reasons of conversion of hip fusion to THA. The conversion to THA is a challenging problem and associated with high complication rates. 3 –5
Most of the previous studies revealed 10-year survivorship rates between 74% and 96% for cemented implants in ankylosed hips. 6 –8 Even though the use of cementless stems showed an increase in all countries, 9 –11 Aderinto et al. 12 reported conversion to THA as an effective procedure with a high risk of major complications and lower functional results. Flecher et al. 13 used 3D-printed, individually designed cementless stems for patients to address the particular anatomical difficulties of the ankylosed hip with excellent functional results. Conversion of the hip fusion is controversial and became a rarely performed surgery because of the high complications rates and lower functional results.
Mid- to long-term results of cementless THA technique for hip fusion patients are limited in the literature, 12,13 long-term follow-up studies being mostly available for cemented techniques. The purpose of this retrospective study is to report the long-term clinical and radiological outcome of cementless THA in patients with ankylosed hips.
Materials and methods
This is a retrospective analysis of 26 patients (29 hips) who underwent conversion from ankylosed hip to THA from 1993 to 2010 at a single institution, by a single senior surgeon. There were 10 male and 16 female patients. The ankylosis had been postsurgical in 18 hips and spontaneous in 11 patients. The average duration of follow-up was 10.1 years (range, 4.5–20 years). The average patient age at the time of conversion surgery was 43.3 years (range, 19–69 years). The duration of ankylosis prior to THA was 20.2 years (range, 4.2–55). The initial diagnosis and demographics of the patients are presented in Table 1.
Demographics of patients.

M: male; F: female; DDH: developmental dysplasia of the hip; JRA: juvenile rheumatoid arthritis; IK: ipsilateral knee; CK: contralateral knee; IH: ipsilateral hip; CH: contralateral hip; LB: low back; H: hip; HHS: Harris Hip Score; HO: heterotopic ossification; SLE: systemic lupus erythematosus.
The indication for conversion was ipsilateral and/or bilateral knee pain in 23% of the patients, whereas 34% had contralateral hip pain, 23% had lower back pain and 20% complained about limited daily motion and limping due to leg-length discrepancy. The involved limb was usually shorter than the contralateral limb. The mean limb-length discrepancy was 4.1 cm (range, 0–8 cm). All patients had palpable abductor muscles contraction preoperatively. According to Dorr index, 11 hips showed type A and 18 type B.
All the surgical procedures are performed under the general and spinal epidural combined anaesthesia. The direct lateral Hardinge approach with anterior capsulotomy and repair 1/3 anterior fibre of gluteus medius using intraosseous sutures was used in all hips in lateral decubitus position. Ankylosed hips have no rotational movements thus can cause challenges for the exposure of the acetabulum. First, we cut the femoral neck at the level of subcapital region and then make a second cut after releasing the capsule around femoral neck at the level of basocervical region. After the second cut, bone block was removed from femoral neck to achieve enough space for acetabulum exposure and rotation of the femoral neck. We used remnant fat tissue of acetabular fossa and if present remnant cartilage tissues as anatomical landmarks to determine the amount medialization during reaming. Femur was prepared with a standard technique for the spontaneously fused hips, guided intramedullary reaming under fluoroscopy was used to avoid malalignment and/or false route of femoral stem in surgical arthrodesis patients if patient had intramedullary fixation.
Cementless stems were used in all of the hips; porous coated tapered conical stems (Synergy®; Smith and Nephew, Memphis, TN, USA) were used in 18 (56%) hips. Other 11 stem types were as following: anatomic type (Zimmer®; anatomic hip system) (n = 3), tapered (Anthology® and Image®, Polar stem®; Smith and Nephew, USA) (n = 5), PFC (n = 2), fully coated distal fixation type stem (Echelon®; Smith and Nephew, USA) (n = 1). On the acetabular side; hemispherical porous coated cementless cup (Reflection Interfit®; Smith and Nephew, USA) was used in 22 hips (75%). Other eight cementless cup types were as follows: Harris Galante II (n = 4), Birmingham (n = 2) and R3 (n = 1). Furthermore, different bearing surfaces were used; ceramic on ceramic (Biolox® and Biolox Forte®, Biolox Delta®; CeramTec, Plochingen, Germany) were used in 14 hips whereas metal on polyethylene (PE) were used in nine hips, zirconia on PE in four hips and metal on metal in two hips.
Abductor arm problems were observed in eight (25%) hips: distal gluteus medius muscle avulsion occurred in five hips and repaired postoperatively with Ethibond; one proximal gluteus medius tear was fixed postoperatively with Dacron; posterior trochanteric avulsion fracture occurred in two hips and treated postoperatively with cerclage wire. During the repair, we maintained the 30°–40° abduction of limb. After repair, these patients used two crutches for 6–8 weeks. Active abduction movement during physical therapy was restricted for 6 weeks to secure repair or reconstruction of the abductors. Also, we used abduction device for the patients who had trochanteric avulsion fracture for 6 weeks.
Clinical and radiological evaluation was performed preoperatively and postoperatively at every 3 months thereafter until 1 year and every 3 years thereafter. Harris Hip Score (HHS) was used to measure pain and function. Increase in HHS more than 20 points with a radiographically stable implant and no further surgical reconstruction was set as a successful result. Any reoperations and/or complications were recorded prospectively. The immediate postoperative radiograph was selected as the baseline for the assessment of subsidence, bone ingrowth, radiolucency, osteolysis and loosening. Loosening was determined according to Gruen et al. 14 Osseointegration of the stems was graded as stable bony ingrowth, stable fibrous and loose. 15 Femoral stems were also assessed for subsidence of more than 2 mm and for changes in alignment (valgus or varus) of more than 2°. 16 The Brooker classification was used to assess heterotrophic ossification. 17
Statistical analysis
Statistical analysis was performed using MedCalc statistical software version 17.9 (MedCalc Software bvba, Ostend, Belgium; https://www.medcalc.org; 2017). Measures were reported as means, ranges, medians, minimums and maximums. We used the Mann–Whitney U test for comparing HHS values. Survival of components was calculated according to Kaplan–Meier survivorship analysis and failure defined as femoral component and THA revision for any reason, respectively. A worst-case scenario for Kaplan–Meier was postulated on the basis of the assumption that for patients who are pending revision for any reason.
Results
Clinical and functional results
The average follow-up was 10.1 years (range, 4.5–20 years). Preoperative average HHS score improved from 52.5 (range, 42–73) to 85.6 (range, 55–98) postoperatively. Excellent and good outcomes achieved in 25 hips (78%). Trendelenburg sign was positive in nine hips (31%). Mean limb-length discrepancy improved from 4.1 cm (range, 0–8 cm) to 1.1 cm (range, 0.8–2.5 cm). The mean range of flexion (extension) was 110.5° (range, 80°–140°), range of abduction (adduction) was 40.1° (range, 10°–60°) and range of internal (external) rotation was 55° (range, 40°–70°). Of the patients, seven (24%) needed one hand support to get up the chair. Wheelchair mobilization was required in one patient. Twenty patients were able to walk with a normal gait, whereas five needed a cane to walk.
Post-operative radiographic analysis
Radiolucency on the acetabular side was seen on one or more zones in 15 patients (16 hips). The most common zone was zone III (n = 10) according to DeLee–Charnley classification. 18,19 Four patients showed radiolucency in all zones and four patients in zones II and III. Six heterotopic ossifications were observed (two grade 1, two grade 2 and two grade 3 according to Brooker (Figure 1(a) to (d)). On the femoral side, 11 patients demonstrated non-progressive radiolucent lines. Six patients had in zone 4 and the remaining five had around zones 3–5; according to Gruen classification, 14 Osteolysis was seen in four hips. (Figure 2(a) to (d))

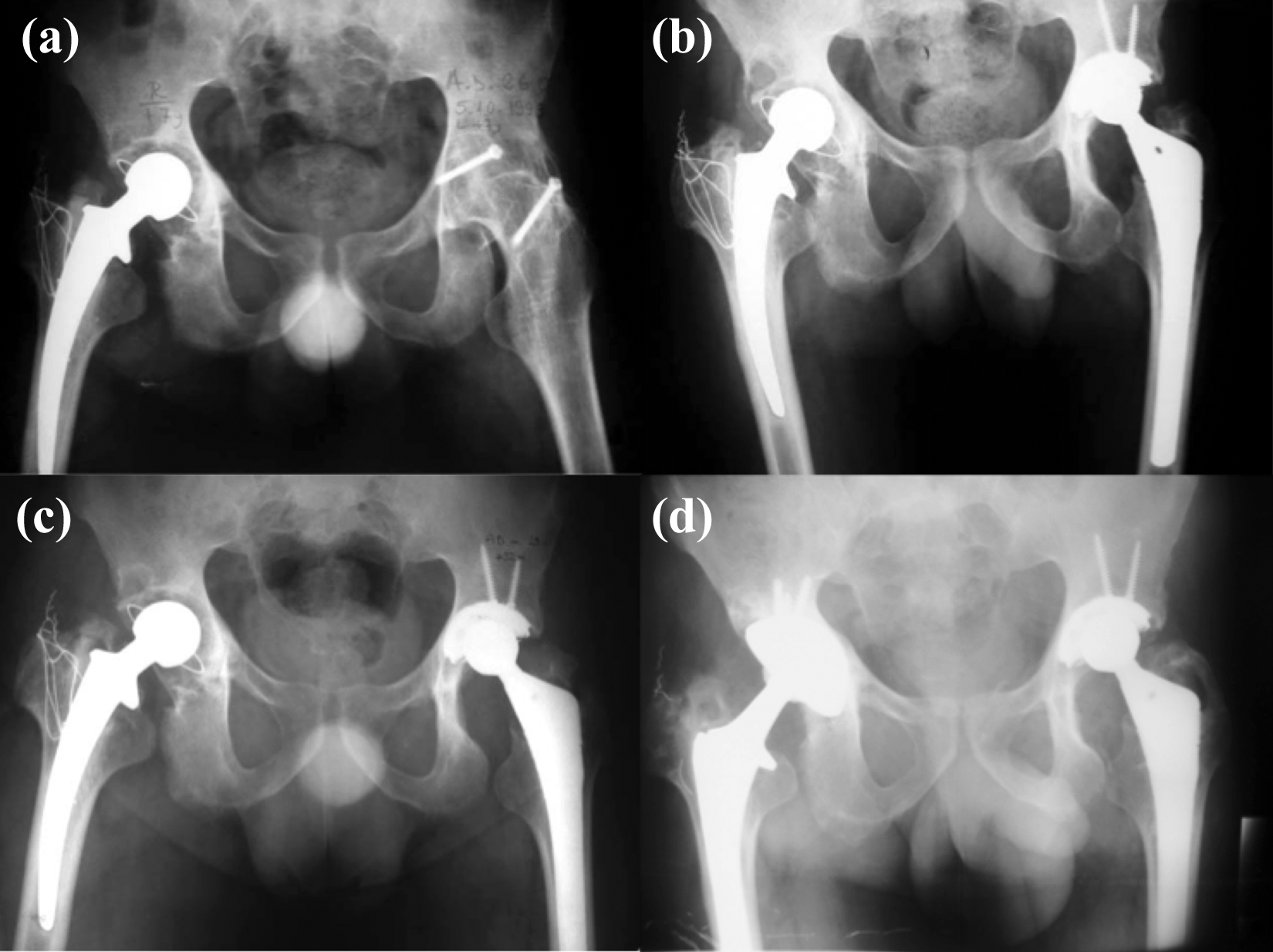
A 40-year-old male patient who had bilateral hip involvements due to ankylosing spondylitis (a) underwent simultaneous bilateral THA with direct lateral approach. (b) Brooker grade 2 heterotopic ossification was seen 3 years after index surgery (c) and non-progressive radiolucent lines were seen around acetabular cup at zones III and II in both side at 12-year follow-up views (d). THA: total hip arthroplasty.
Radiographs showed the case of a 28-year-old male patient who had two operations in his left hip due to misdiagnosed of ankylosing spondylitis 5 years ago (a). Early postoperative view after THA (b), and 3-year follow-up radiography showed no heterotopic ossification (c). Polyethylene wear and osteolysis were seen after 18 years from index THA (d). THA: total hip arthroplasty.
Complications and survival
Two patients suffered from deep infection: one of them was treated 4 months postoperatively with debridement and liner–head exchange. The other patient needed femur and acetabulum revision at 1.5 years postoperatively. One patient had acetabular fracture during surgery and fixed with plate and screw osteosynthesis. There was an intraoperative distal femoral fracture in one hip, and this fracture was treated with a longer stem placement. One patient had sciatic nerve paralysis that required an operative release.
We had one acetabular loosening due to subsequent wear of zirconia PE bearing 11.5 years after index surgery and undergone revision. Two patients were pending for revision for acetabular liner exchange due to wear of zirconia on PE bearings. The Kaplan–Meier overall survival of components with any revision as the endpoint was 81.5 (95% confidence interval, 73.8–89%) (Figure 2) at 11.5 years (Figure 3), with a worst-case scenario 66.4% (95% confidence interval, 62.2–82.1%). The overall survival of components with aseptic loosening as the endpoint was 91.3% (95% confidence interval, 88.2–94.6%).

The graph shows the cumulative survival rate of total hip system, with any revision as the endpoint, was 81.5 (95% confidence interval, 73.8–89%).
Discussion
Conversion of hip ankylosis to THA has been a challenging procedure. This study confirmed other studies 4,6,12,20,21 which found out that conversion to THA is a satisfactory procedure with good result. However, reported complication rates were higher than normal THA and vary between 11% and 54%. 5,6,8,12,22 According to the current study, abductor muscle–related complication is still major problems in this patient group.
The result of cementless stems in conversion ankylosed hip to THA with long-term follow-up is limited in number. Kim et al. 23 showed no significant difference between cemented and cementless THA after fusion takedown. Using only cementless stems, Rajaratnam et al. 20 concluded previously ankylosed hip showed good long-term results with one revision in 16 hips in 10 years. Flecher et al. 13 reported an excellent survival rate with custom-made cementless stems at 15 years. This study demonstrates cementless implants achieved good survivorship and stability, good clinical outcomes scores at an average of 10-year follow-up. The Kaplan–Meier overall survival rate, with aseptic loosening as the endpoint, was 91.3% at 10 years.
Another concern is the surgical approach for these complex cases. Every surgical approach has its own advantages and disadvantages. The main difference between anterior approach and other most widely used lateral and posterior approaches is the muscle-sparing technique. 24,25 Preoperative abductor muscle quality, strength and surgical complications affect the postoperative performance of abductor in these patients. Numerous studies reflected different results on negative Trendelenburg sign and limp-free gait for conversation of ankylosed hip to THA. 11,16,23 Celiktas et al. 21 used a posterior approach in 40 hips and 30% of the hip had a postoperative positive Trendelenburg sign. Flecher et al. 13 used anterolateral Watson–Jones approach in 23 hips and 13% of the hips had positive Trendelenburg sign. A cohort study by Fernandez et al. 22 showed 37% of the patients with positive Trendelenburg sign after conversion via various surgical approaches. In our study, we used direct lateral approach in all cases, nine hips (31%) showed positive Trendelenburg sign postoperatively.
Nerve injury is a potentially serious complication of conversion arthroplasties and mostly affects sciatic, femoral and peroneal nerves. 26 Tamaki et al. 27 used a direct anterior approach for THA conversion of fused hips. They reported no risk of muscle denervation because the direct anterior approach uses the true internervous plane. Celiktas et al. 21 also didn’t face any nerve palsy in 40 hips using posterior approach. Although one posterolateral approach study 23 reported two peroneal and two femoral nerve injuries in 87 hips, they used cementless implants in their surgeries. Using lateral approach, our series showed only one sciatic nerve paralysis (3%). Other reports that used lateral approach for conversion to THA showed nerve injury rates between 0% and 9%. 6,8,13,28 Dislocation is another major concern in these patients. Kim et al. 23 reported two dislocated hips out of 45 hips in the cementless group using posterolateral approach. Using cementless implants, Tamaki et al. 27 stated one anterior dislocation in nine hips. Similar to Flecher et al. 13 and Hamadouche et al. 8 our study showed no postoperative dislocation.
Heterotopic ossification (HO) has been reported to occur following hip arthroplasty but is asymptomatic in the majority of conversion group. 12 In our study, six patients (20%) had HO without functional restriction. Aderinto et al. 12 reported a 33% incidence in a series of conversion to THA patients by applying lateral approach. Joshi et al. 6 showed 13% occurrence rate after conversion to THA. Using the anterolateral approach, Flecher et al. 13 observed HO in 13% of their patients. Celiktas et al. 21 reported no HO in their series with posterior approach. There are no certain data for these patients on which surgical approach has a lower risk for HO, but routine prophylactic treatment such as non-steroidal anti-inflammatory drugs or radiotherapy may be considered for these complex cases. 29
There were a few limitations in this study. First of all, there were no control groups. Furthermore, we only evaluated patients’ limb-lenght discrepancy (LLD) clinically. Together with clinical assessment of LLD, a wise use of comprehensive imaging methods such as standing full-length anterior-posterior-computed radiograph or computed radiography teleoroentgenogram may optimize patient evaluation. 30 Another limitation is that, as an outcome measure, we only used HHS. Initially, surgical indications, pain and functional capacity, are the two dominating domains in HHS whereas deformity cannot be analysed as well. 31 In addition, even though HHS is effective in short-term (between preoperative and 6-months postoperative), it remains as a weak outcome score in long-term (after a 2-year follow-up). Also, bodily or referred pain couldn’t be evaluated accordingly using HHS. 32 Intraoperative palpation and observation was done to evaluate status of the gluteal muscles. This technique is the optimal choice but its subjectivity remains a problem. 23 Cementless femoral and acetabular components were not uniform and loosening and osteolysis was evaluated only in plane radiographies.
In conclusion, THA is an effective treatment method, which provides functional recovery and patient satisfaction in ankylosed hips. Preoperative and postoperative abductor status of the patient is still critical point for patient satisfaction.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.