
Abstract
Purpose:
To determine the perceptions of surgeons at both consultant and resident level to the difficulties of performing knee arthroscopy and to determine their willingness to adopt robotic technology.
Methods:
A questionnaire was designed to discern the attitude of orthopaedic consultants and residents to the technical challenges of performing knee arthroscopy and the possible role of robotically enhanced surgery. The questionnaire included 31 questions across five key domains.
Results:
Iatrogenic damage to articular cartilage was thought to occur in at least 1 in 10 cases by 50% of respondents with 15% believing that it occurred in every case. One hundred or more procedures were thought to be necessary to overcome the learning curve by 40% of respondents and 77.5% believed that 50 procedures or above were necessary. Ninety-nine per cent of respondents agreed that higher technical skills would decrease unintended damage. Despite such difficulties with the procedure and no prior experience with robotic surgery, 47% of respondents see a role for semiautonomous arthroscopic systems in the future.
Conclusions:
Surgeons believe that knee arthroscopy is a difficult procedure with a long learning curve and a high incidence of iatrogenic cartilage damage. Many find it ergonomically challenging and have frustration with current tools and technology.
Clinical Relevance:
This is the first study that highlights surgeons’ difficulties performing knee arthroscopy despite the commonly held attitudes that it is a straightforward procedure. Systems that are able to decrease these problems should improve patients’ outcomes and decrease the risk of harm.
Introduction
Robotically assisted minimally invasive surgery (RAS) is an emerging field both in orthopaedics and other surgical specialties. RAS has demonstrated advantages over the traditional open surgery like reducing pain, recovery time and producing less scarring. 1 The future adoption of robotic surgery (assisted/autonomous) will, in part, be determined by how comfortable surgeons and patients are with such technologies. Furthermore, the need for new technologies can only be identified by understanding technical challenges that a procedure currently presents to a surgeon and how these may be mitigated for better clinical/patient outcomes. To date, there have been no publications or literature examining a surgeon’s difficulties in using the current arthroscopy system and the willingness to adopt robotic technology in their clinical practice for better patient outcomes.
Knee arthroscopy is a common and well-established minimally invasive surgical procedure for diagnosis and treatment that entered mainstream orthopaedic surgery in the early 1970s. 1 There are currently more than 4 million knee arthroscopies performed worldwide annually, at a cost of US$15 billion, according to the American Orthopaedic Society for Sports Medicine. In Australia, 71,087 hospital admissions were recorded for knee arthroscopies in 2010–2011 with 81% of these being performed in private hospitals. 2 Even though knee arthroscopies are widely utilized, its efficacy has been questioned, 3 –6 and there are a broad range of known complications. 7 The reasons behind these problems are multifactorial and can be grouped into operator inexperience, rigid anatomy, poor intra-articular vision and lack of a tissue demarcation between diseased and healthy tissue. 8
With regard to operator inexperience, previously, researchers have devised the Global Assessment Score as a validated measure of an individual’s performance in arthroscopy simulation. 9,10 Although literature shows that one of the main issues during arthroscopy in the learning phase is damage to the cartilage, no publications cite this as a measure of competency. 9,10 The natural history of iatrogenic cartilage lesions is unknown. To evaluate the efficacy of knee arthroscopies, research to date has mainly focused on patient handling, after care, and patient outcomes 8 giving little importance to a surgeon’s perspective of the surgical approach using current tools and instruments.
The aim of this study was to determine the perceptions of surgeons at both consultant and resident (Australian Orthopaedic Association Certified Training Registrar) level to the difficulties of performing knee arthroscopy and to determine their willingness to adopt robotic technology. We selected knee arthroscopy, as it is an operation that is widely performed and is performed by a diverse group of surgeons including those in training. Currently, there are no robotically assisted technologies being utilized in knee arthroscopy, and the surgery is performed entirely manually.
Methods
A questionnaire was designed to discern the perceptions of orthopaedic consultants and residents towards the difficulties associated with performing knee arthroscopy, as well as their attitudes towards the possible role of robotically enhanced surgery in this context. Given that the questionnaire set out to record actual surgeon experiences and personal perceptions, a high degree of external validity was sought. As there has been little research in the area of surgeon perceptions previously, questions needed to be developed for this study. The questionnaire was therefore developed following appropriate question design principles, in direct consultation with knee arthroscopy surgeons. It was then informally piloted among another group of knee arthroscopy surgeons. Questions were found to accurately and consistently measure the required constructs, and internal reliabilities were above acceptable levels for all scale questions.
The sample was identified via The Australian Orthopaedic surgical training programme, which runs over 5 years. Only surgeons in active practice and performing knee arthroscopy were included. There were no patients involved in the study, and no patient information was requested from any surgeon undertaking the survey. All respondents were de-identified. The questionnaire included 31 questions across 5 key domains: surgeon experience and basic demographics; surgeon perceptions of learning curve, technical difficulties and iatrogenic damage; surgeon experiences with and attitudes towards posture, ergonomics and equipment; visualization of the surgery; future robotic innovation.
Data was obtained from 93 respondents, 45 trainees (48.4%) and 48 consultant orthopaedic surgeons (51.6%). Given that the sample represented a very specific group representing a relatively small percentage of the general population, the sample size is appropriate for this study. Responses were scored using a five-point Likert scale. Statistical analysis was performed using a χ2 test for comparison of frequencies between groups, with the level of significance set to 5%. Multiple testing was adjusted for using Bonferroni’s correction.
Results
Domain 1: Surgeon experience and demographics
Responders were distributed across all years of training. Consultant surgeons had been in practice a mean of 7.1 years (SD 7.3, range 0.5–25 years). Thirty one (64.6%) consultants versus two (4.4%) trainees had performed more than 50 procedures per year, with this difference being statistically significant (p < 0.001). Just under 77.8% (35) trainees performed less than 31 procedures per year (Figure 1).

Number of surgeries performed per year by respondents: Bar graph showing number of surgeries performed per year by consultants and residents.
Domain 2: Learning curve, technical difficulties and iatrogenic damage
Iatrogenic damage to articular cartilage was thought to occur in at least 1 in 10 cases by 49.5% (46) of respondents with 7.5% (7) believing that it occurred in every case. There were no statistical differences between resident and consultant responses (Figure 2).
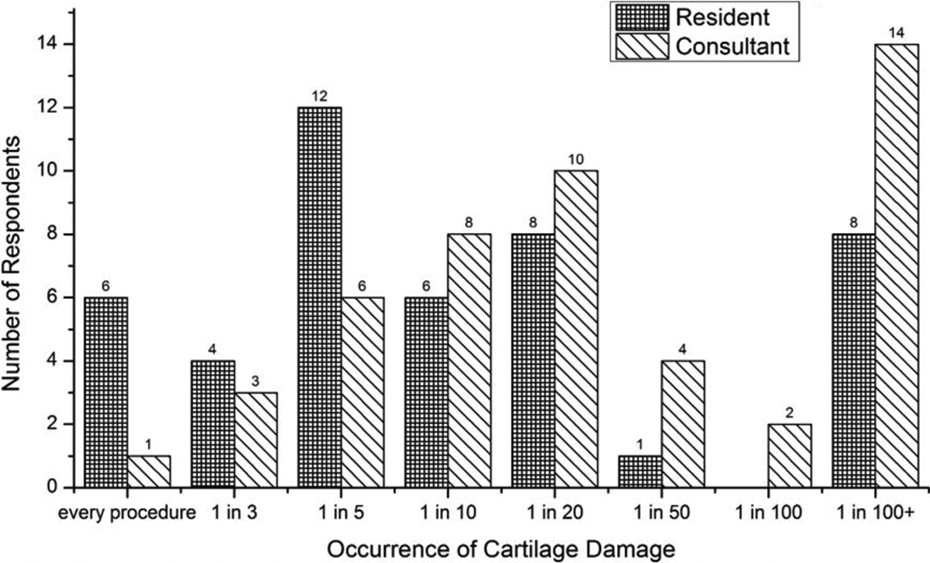
Occurrence of cartilage damage in procedures estimated by respondents: Bar graph showing the occurrence of cartilage damage in procedures estimated by consultants and residents.
When asked about the relationship between a surgeon’s level of arthroscopy skill and unintended cartilage damage, 98.9% of respondents agreed that higher technical skills would decrease unintended damage, whereas only one resident respondent said that there is no link between skill and damage caused during knee arthroscopies (Figure 3).
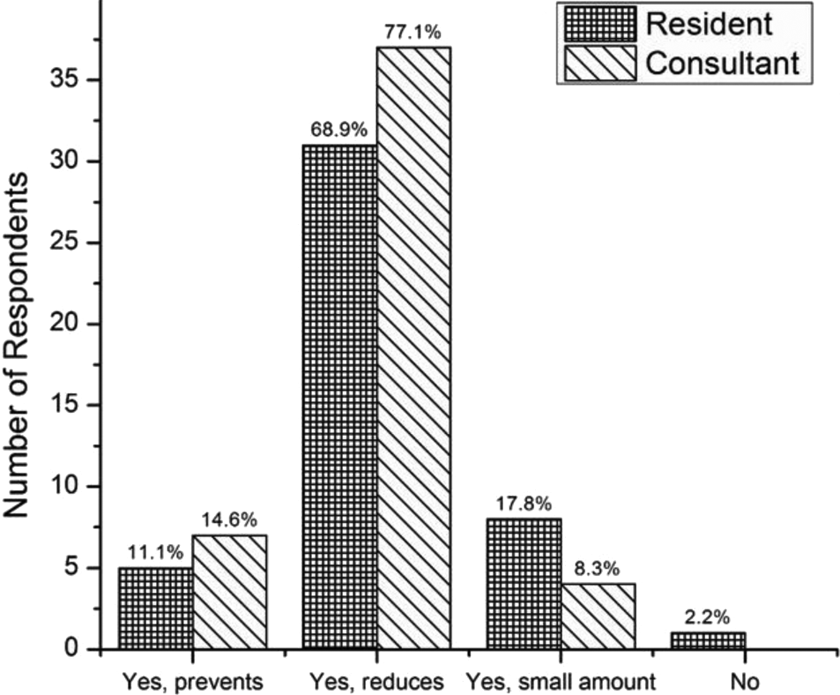
Link between skill and unintended damage: Bar graph showing the responses by consultants and residents to the question: ‘Does a high level of arthroscopic skill limit iatrogenic cartilage damage?’
One hundred or more procedures were thought to be necessary to overcome the learning curve by 39.8% of respondents (4.4% thought 500 procedures was the minimum). 77.4% believed that 50 procedures or above were necessary. There were no significant differences between resident and consultant responses (Figure 4)

Number of knee arthroscopies required to overcome the curve estimated by respondents: Bar graph showing the estimated number of knee arthroscopies required to overcome the learning curve by residents and consultants.
Domain 3: Posture, ergonomics and equipment
59.1% (55) p = 0.697 of respondents found knee arthroscopy to be ergonomically challenging with 22.6% reporting that they have experienced physical pain after performing a knee arthroscopy; half of these surgeons reported pain in their lower back and 30% reported shoulder pain. Frustration with the arthroscopic equipment was experienced by 73.1% (68) p = 0.310 of surgeons over their previous 10 cases. There were no significant differences in resident or consultants responses (p = 0.310).
Domain 4: Visualization
All but one surgeon reported that some sections of the knee are difficult to visualize, while 76.3% of surgeons report that the posterior portion of the knee was difficult to visualize using the current arthroscopy systems. There were 80.0% (36) of residents and 31.3% (15) of consultants who had trouble visualizing part of the knee in their last 10 cases, which was statistically significant (p < 0.001).
When questioned about specific technologies or equipment that might aid visibility, 47.3% (44) p = 0.529 of surgeons reported a larger screen is beneficial, 58.1% (54) p = 0.468 reported benefit from zoom functions and 40.9% (38) p = 0.981 reported multiple screens made it easier to visualize the knee. 40.9% (38) p = 0.565 reported that real-time generation of a three-dimensional model of the joint, using computer-reconstructed images from the arthroscope and displayed on a separate screen would be beneficial. No significant differences were observed between resident and consultant responses, indicating general agreement about which aids are beneficial.
Domain 5: Future robotic innovation
32.3% (30) p = 0.064 of surgeons reported that they were nervous about the introduction of semiautonomous arthroscopic systems, while 18.3% (17) p = 0.794 of surgeons felt that the technology would shorten the learning curve for the procedure. 76.3% (71) p = 0.712 would use such a system if it improved efficiency and 86% (80) p = 1.000 if it decreased the rate of iatrogenic damage to cartilage. 58.1% (54) p = 0.636 of surgeons reported they would use semiautonomous arthroscopy if it increased their working life. Only 10.8% (10) p = 0.515 of surgeons believed that they would be able to treat more patients if they had access to the technology. 19.4% (18) p = 0.616 of surgeons would use the technology if it permitted them to perform multiple operations simultaneously. Overall, 47.3% (44) p = 0.740 of respondents see a role for a semiautonomous arthroscopic system in the future.
Discussion
Robotics has emerged in many fields allowing tasks to be performed safely and reliably. Medicine has been a late adopter of such technology but this will rapidly change in the upcoming decades. Surgeons will need to learn new techniques and become comfortable with the use of such technology. One of the reasons postulated about the slow uptake of robotics in surgery is that surgeons do not believe that they need such technology to perform surgery safely. This is contradicted by the fact that all operations are known to have a learning curve and there are many published articles discussing this issue. 11 –13
We have shown that surgeons are generally comfortable with the introduction of robotic technology to the operating theatre. We also show that although knee arthroscopy is widely performed, it is an ergonomically challenging procedure with a long learning curve required to develop the skills to perform competently. This finding was recently quantified in a simulated model 14 with a predicted 170 cases required for a surgeon to reach baseline competency. This learning curve means that trainees are likely to require more time to perform each surgery and have an increased risk of complications arising from the procedure. While 99% of surgeons agree that higher skill levels are correlated with lower incidence of iatrogenic cartilage damage, our study shows that surgeons routinely underestimate the level of experience required to be truly competent, falling short of the 170 procedures recommended by Price et al.’s study. 14 Surgeons may therefore be underestimating the severity of the learning curve necessary to achieve positive patient/clinical outcomes. If every surgeon needs to perform 170 knee arthroscopies before becoming competent, then any technologies that can decrease this number will be of great value to patients. Moreover, this study suggests that most Australian trainees are not likely to have achieved consultant-level competency at the completion of their training.
In addition to improving patient outcomes, preventing occupational injury to surgeons may be an additional benefit of any robotic-assisted technology that reduces the ergonomic challenges that knee arthroscopy currently imposes. This is supported by our findings with 59% of surgeons reporting that knee arthroscopy is ergonomically challenging and 23% of surgeons reporting physical pain following arthroscopy procedures. Currently, the impact of knee arthroscopy on surgeon occupational injury is unknown. However, with patient obesity rates continuing to increase across both the western and developing world; the task of managing the operative limb will not get any easier over time if current manual operative methods are utilized, exposing surgeons to increasing occupational hazards.
Surgeons in this study accept that a high rate of iatrogenic (unintended) damage occurs during arthroscopy. In addition, iatrogenic damage seems more likely to occur with junior surgeons and trainees. Moreover, there is broad acceptance that technology can improve arthroscopic surgery. Robotic-assisted knee arthroscopy has many potential advantages in easing the physical burden for the skilled surgeon, improving ergonomics and delivering a more precise operation. This could decrease unintended iatrogenic trauma and improve visualization, thus increasing diagnostic yields and the execution of arthroscopic repairs. Current state-of-the-art technologies are largely experimental; however, some clinical applications are currently in use. 15 Progress has been made in autonomous surgical manoeuvres, optical coherence, tomography guidance, motion compensation and revolutionizing surgeries, such as robotic laparoscopic operations. 16 Currently, there are no robotically assisted technologies being utilized in knee arthroscopy, and the surgery is performed entirely manually. This presents an opportunity for the use of robotic technology because of the confined spaces within the knee joint and the complex manoeuvres of the leg that are required to access the joint and perform the surgery.
Although our results show that surgeons claim that they are willing to adopt new technologies if they improve outcomes, there will be many barriers to the uptake of these technologies. In profit-driven healthcare systems, throughput is important to both surgeons and hospitals, any technology that adds time to a procedure, even if only during its initial introduction, will meet resistance. An example of this is computer-assisted knee replacement. It has been demonstrated in the Australian National Joint Replacement Registry that in younger patients (<65), revision rates are lowered with the use of computer assistance. 17 Despite this, the technology has had a very low uptake in many countries including the United States and United Kingdom. 18,19 Arthroscopic robotic technologies will likely need to show not only safety benefits to patients and staff but also convey efficiency benefits over current techniques in order to justify their cost of introduction.
Although none of the surgeons in this study have experience in performing robot-assisted surgery, 47.3% of them see a role for robotic surgery in the future. The willingness to use robots in the operating theatre by surgeons will potentially rise given that benefits to patients and surgeons can already be seen from these new technologies over traditional paradigms. Education of surgeons on these emerging technologies will speed up the adoption of robot-assisted surgery. Refer Figure 5 for an infographic representation showing the perceptions of orthopaedic surgeons on arthroscopic surgery today and in the future.

Arthroscopic surgery today and in the future: Infographic representation showing the perceptions of orthopaedic surgeons on arthroscopic surgery today and in the future.
Limitations
This study was limited to only Australian orthopaedic surgeons whose views may not reflect that of surgeons globally. In addition, surgeons may not be aware of the rate of development of robotic technology and how it may affect their working careers over the midterm. In spite of these limitations, the study has highlighted that arthroscopy is a challenging procedure that can potentially be improved with the introduction of robotics.
Conclusion
Surgeons believe that knee arthroscopy is a difficult procedure with a long learning curve and a high incidence of iatrogenic cartilage damage. Many find it ergonomically challenging and have frustration with current tools and technology. Despite this, less than 50% of surgeons see a role for semiautonomous arthroscopic systems to aid surgery.
Footnotes
Acknowledgements
Ms Clare Villalba for an infographic representation of the research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Advance Queensland Scheme for the funding support.