
Abstract
Diplopodia, being a rare congenital disorder, is infrequently discussed in published texts. Most reported cases have accounted the involvement of duplicated preaxial digits with other associated organ system and physical deformities. Here, we present an unusual case of isolated diplopodia involving postaxial toes in a child with no other organ and physical abnormalities. Radiological studies revealed a set of 10-digit-duplicated foot over the lateral aspect of the native foot, complete with phalanges and its corresponding metatarsals as well as tarsals, supplied by an anomalous posterior branch of the popliteal artery. Definitive surgery was performed just before the child was learning to walk.
Introduction
Diplopodia or duplicated foot is an extremely rare disorder in which the extra digits consist of phalanges, in addition to well-formed accessory tarsal bones and corresponding metatarsals. This condition must be differentiated from polydactyly by the absence of accessory tarsal bone(s). 1 To date, literature on postaxial-type diplopodia is scarce, as most available authors have reported preaxial diplopodia type.
Case report
A 5-week-old baby girl born full term with uncomplicated antenatal history of nonconsanguineous parents presented to Sarawak General Hospital, Borneo, for duplicated right foot with 10 toes. Routine prenatal ultrasound did not detect the anomaly. There was no history of diplopodia in the family and no maternal teratogen exposure.
Clinical presentation
General examination revealed no gross dysmorphic facies. Physical and mental developmental milestones were corresponding with her age. Detailed examination showed lower extremities of equal length. The aforesaid 10-digit duplicated right foot was emanating from the inferolateral aspect of the native little toe, as depicted in Figure 1. The main right foot has perfect five toes. Devoid of the great toe, the duplicated right foot was in an inverted position. The left lower limb is clinically normal in appearance. The movement of the native right lower limb was normal at all joints. There was lesser active motion elicited from the duplicated foot. Distal pulses were normal on the native right foot. Further examination did not reveal other physical abnormalities.

The plantar and dorsal surface of the duplicated right foot. Ten toes can be seen (1, 2, 3, 4, 5, A, B, C, D and E). Native toes are labeled from 1 to 5 and accessory toes are represented by alphabets A to E. The big toe was absent at the duplicated foot.
At age of 11 months, the child was learning to stand. Weight-bearing area of the affected limb was on the lateral border of the inverted duplicated foot.
The main problem faced by the child was abnormal posture when standing due to the position of the duplicated foot, grotesque appearance resembling a fan and inability to don footwear. The aim of surgery was to provide child with plantigrade foot, to bestow the privilege of wearing shoes and to improve cosmesis, thus avoiding possible future psychological difficulties.
Radiological findings
On plain radiograph shown in Figure 2, taken at the age of 9 months, there were 10 fully developed digits, each with its own metatarsal. The accessory foot great toe appeared to be absent as evidenced by the smaller sized individual phalanges and three phalangeal digits that did not match the features of the great toe. Three ossified cuboids were present at the duplicated foot. The most peculiar element of this accessory foot X-ray was the absence of talus and the presence of a structure that appeared to be a less developed extra calcaneum adjacent to the larger duplicated calcaneum. The larger duplicated calcaneum was exactly a mirror image of the native calcaneum.
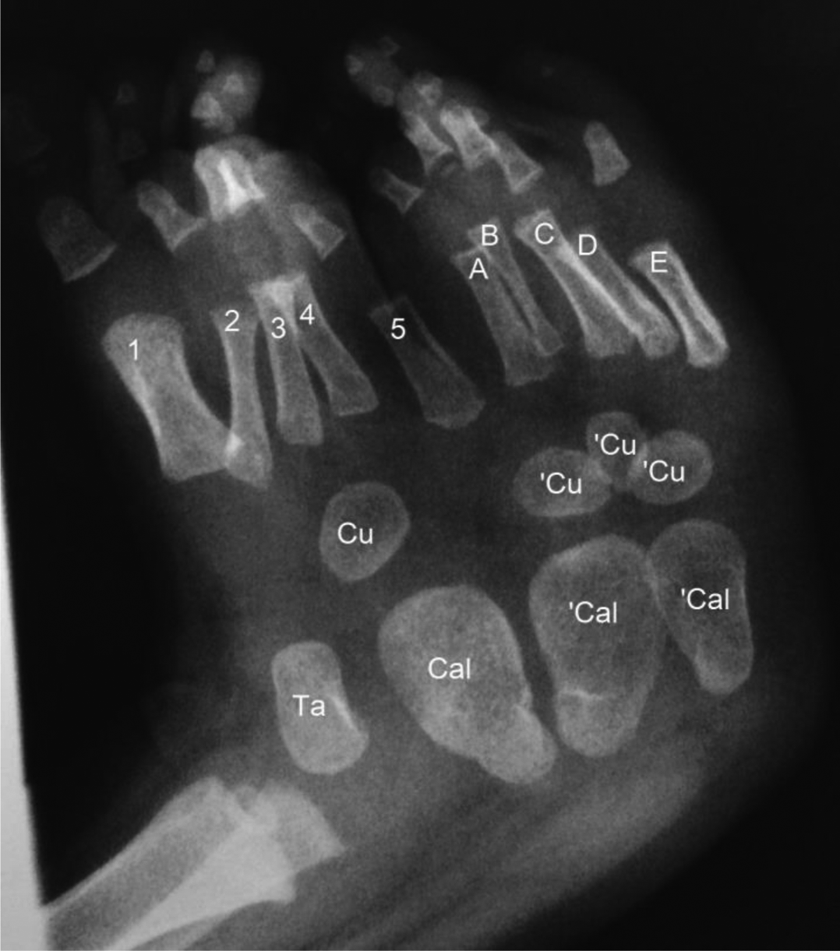
Plain radiographs of the right foot taken when the child was 9-months old. Native foot metatarsals are numbered from 1 to 5 and duplicated metatarsals are labelled A, B, C, D and E. A set of calcaneum (Cal), Talus (Ta) and cuboid (Cu) were present in the native foot. The duplicated foot has double sets of calcaneums (‘Cal) and triplication of cuboids (Cu).
A computed tomography (CT) angiography was done to evaluate the anatomy of the affected limb and vascular anatomy prior to surgical amputation of the accessory right foot. The radiographic study in Figure 3 revealed a near complete mirror image duplication of the right foot with the duplicated foot having its own talus and calcaneum. Both lower limbs displayed single tibia and fibula of the same size and length. The right popliteal artery was larger than the contralateral side. It was abnormal in its course and bifurcated into two main branches at the popliteal fossa. The anterior branch bifurcated at the popliteal fossa into right anterior and posterior tibial arteries and peroneal artery. The anomalous posterior branch gave rise to two tributaries at 3 cm proximal to the native calcaneum, namely the anteromedial branch and the posterolateral branch. The anteromedial branch supplied the dorsum and the sole of the duplicated foot. The posterolateral branch, which was located posterior to the posterior tibialis artery, supplied the plantar area of the last three digits of the normal foot. Another small branch arose from the posterior aspect of the muscle at the ankle level.

CT angiogram of both lower limbs. Note the anomalous artery at the duplicated right foot. CT: computed tomography.
Preoperative planning
Surgical planning was done upon receiving the results of the CT angiogram. The child underwent surgery around the time when the child was able to pull herself to stand.
Intraoperative findings
A tourniquet was applied at the right midthigh section to minimize intraoperative haemorrhage. The undermining of skin edges was avoided to minimize devascularization. Therefore, careful incision was made to preserve as much plantar skin and subcutaneous tissue as possible. The anteromedial artery of the anomalous posterior branch supplying the duplicated foot was identified and ligated. Subperiosteal dissection of the metatarsals and tarsals immediately adjoining the native foot structures was done to create full thickness tissue flap. The smaller duplicated calcaneum was excised completely. The main duplicated calcaneum was not totally excised as it was too close to the native calcaneum. This was also to minimize the disruption of the blood supply to the heel pad, and thus to reduce the risk of heel pad necrosis. Furthermore, it is also aimed at maintaining the volume of the heel for weight-bearing. The periosteum surrounding the duplicated calcaneum was preserved to maintain the periosteal plexus for the viability of the heel flap.
The subcutaneous tissues and skin were closed with absorbable sutures. Immediate post-wound closure photograph is shown in Figure 4. The wound was dressed with a sterile bandage. The foot was in a slight inverted position. A below knee cast was applied as a measure to correct the malpositioned foot.

Postoperative excision of accessory right foot.
The excised accessory right foot was examined post-wound closure. On gross inspection, the two rays contiguous to the native fifth toe displayed perfect metatarsals, as shown in Figure 5. We did not proceed to dissect the specimen, as the child’s parents did not consent to it.

The plantar surface of the excised duplicated right foot. The duplicated metatarsal immediately adjacent to the native fifth metatarsal was in perfect shape.
Postoperative progress
On postoperative day 14, the cast was removed and wound has healed. The foot was in a plantigrade position.
A plain radiograph in Figure 6 obtained at 2 months postoperatively, when the child was 17-months old, showed residual accessory calcaneum. Ossification of the medial cuneiform has taken place. The deliberate partial resection of the duplicated calcaneum resulting in the presence of remnants of the extra calcaneum shown in Figure 6 has contributed to the broad right heel, as shown in Figure 7.

The plain radiograph of the right foot taken postoperatively at the age of 17 months showed ossified LC and remnant of accessory calcaneum (‘Cal). LC: lateral cuneiform.

Plantar and medial aspect of the child’s foot at 2 months postoperative period.
Subsequently, the child, now a contented 27-month-old toddler, progressed to a normal gait, despite of the wider right heel than the left.
Discussion
Diplopodia was previously described in a very first publication of its kind by Karchinov, 1 as partial duplication of the foot with the accessory structures located on the tibial aspect. Diplopodia is less common than diplocheiria or duplication of the hand. 2 In addition to supernumerary digits, duplicated foot has well-formed accessory tarsals and metatarsals, which are separated from the structures of the normal foot. It must be differentiated from polydactyly where the additional structures consist of toes that may or may not have corresponding metatarsals but devoid of tarsal bone. 1,3
Another term, which is mirror foot, is a loosely used term to refer duplicated foot involving preaxial toes. 3 –5 At present, there is no consensus on the exact definition of mirror foot. 6 An existing literature described mirror foot as an extreme spectrum of preaxial polydactyly, where the duplicated anatomical elements involved are the tibial aspect foot skeletal structures, in combination with fibular hemimelia and absent great toe. 7 Mirror foot has to be distinguished from our case where the extra digits involved here were the rays of the fibular side (postaxial). While most publications reported diplopodia with duplicated structures on the medial or tibial aspect, 1,3,8 –11 a more recent publication by Hocaoglu et al. 12 has extended the traditional description of diplopodia to structural elements of the fibular side, which is similar to our case.
The duplicated postaxial rays in our case were in perfect form, in contrast to a literature, which also reported duplicated foot involving the lateral rays but has a Y-shaped metatarsal that connects the native foot to the extra foot. 12
Limb formation begins as limb buds from the ventrolateral body wall at the fourth week of embryonal development. 13 There is an extremely intricate interplay of various elements in the stages of limb development in which in any point disrupted may lead to a range of malformations such as absence, duplication of a structure or hypoplastic limb. Exposure to teratogens such as thalidomide during this period can cause deformities in extremity development. 13 However, in this case, there was no antenatal exposure to possible teratogens in our questioning of the patient’s mother about her pregnancy. Until now, no apparent factors can be attributed to cause diplopodia in human. 14
This is an unusual case of diplopodia as there were no associated physical or internal organ defects. Most existing literatures reported similar cases with other anomalies, such as defective tibia or fibula, 1,4,5,8,15 syndactyly or polydactyly, 8 imperforate anus 9,12,16,17 cardiac defects, 9,14 renal agenesis 4,12 and hypothyroidism. 10
In majority of the available case reports, the duplicated foot emerged from the native foot itself. Brower et al. 16 reported an extremely rare case of duplicated foot emanating from the posterolateral aspect of the calf instead of the native foot.
Table 1 depicts a list of existing publications on duplicated foot cases, summarizing the gender of the patients, number of extra bones, origin of the duplicated structures (pre- or postaxial duplication) and the other accompanying birth defects.
Collection of previous reports on duplicated foot.

Looking into the ossification timing of tarsal bones, the three tarsal bones that are ossified in utero are the calcaneum, talus and cuboid. Ossification centres for the lateral, intermediate and medial cuneiforms will only become visible on roentgenographs at 1–3 years of age, respectively. The navicular ossification centre appears on X-ray at 3 years of age. 19 Analysing the plain radiograph of the foot taken at the age of 9 months (Figure 2), as expected for that age, the native foot showed the ossified calcaneum, talus and cuboid. The accessory foot appeared to have two sets of calcaneums. Based on the knowledge on the appearance of ossification centres, the three smaller tarsal bones at the accessory foot showed in the plain X-ray at 9 months of age are most probably three extra cuboids. The presence of the lateral cuneiform in the postoperative plain radiograph taken when the child was 14-months old (Figure 6) corresponds to the expected ossification time.
Currently, there is no standard protocol on the treatment of diplopodia. Treatment should be considered case-by-case basis and tailored appropriately to suit individual needs and circumstances. The surgical intervention for this child took place in time for the patient to enjoy the privilege of a normal learning walking process and in accordance with the recommended timing in other similar reported cases. 1,12,18 The ultimate aim of the surgery is to provide the child with a normal or near normal functioning plantigrade foot. Timely surgical intervention will enable patient to adapt to the structural changes early, as the reconstructed bone will remodel over time. Furthermore, surgical intervention during prewalking phase will allow child to focus on gait retraining. The secondary aim is to reconstruct the foot to be more aesthetically acceptable to the general public. 12
Conclusion
In conclusion, we have reported an uncommon case of unilateral diplopodia involving the postaxial digits in a child with no other gross physical abnormalities and organ system disorders. Following surgical excision of the duplicated foot, the child was able to walk normally and avoid possible future psychological difficulties stemming from social stigma for her fanned foot deformity. Therefore, surgical intervention aimed at improving quality of life is essential before the child reaches preambulatory age.
Footnotes
Acknowledgment
We would like to extend our heartfelt gratitude to the parents of the child described for allowing us to share her details, to the Director General of Health, Ministry of Health Malaysia for giving us the permission to publish this case report and to the following individuals who have contributed in the management of this patient: Madam Ajek Entri, Miss Nurul Bahiyah and Madam Soh Mee Hua.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.