
Abstract
Purpose:
Athletes often receive conservative treatment for injured anterior cruciate ligaments (ACLs) so that they can continue to play to the end of their season. The purpose of this study was to examine the conscious performance and arthroscopic findings of athletes who received conservative therapy for ACL injuries.
Methods:
Forty-two patients with ACL injuries underwent conservative treatment. After the season ended, ACL reconstruction was performed. We examined the following parameters: (1) time required for return to competition after injury, (2) conscious performance after return to competition, (3) whether the injured knee gave way during conservative therapy or after return to competition, and (4) cause of performance deterioration if applicable. To determine conscious performance, patients were asked to rate their performance after therapy relative to their performance before injury.
Results:
Thirty-eight of the 42 patients (90.5%) returned to competition after conservative treatment. The mean time to return was 13.8 ± 7.6 weeks, and the mean conscious performance score was 58.4 ± 16.5%. Thirty-eight patients (90.5%) experienced their knee giving way, of whom 36 (94.9%) stated that fear of their knee giving way hampered their performance. At the time of ACL reconstruction, 9 patients had chondral injuries and 22 patients had meniscus injuries.
Conclusion:
Most athletes with damaged ACLs returned to the field within the same season after conservative treatment. However, conscious performance was only about 60%. It is possible that knees giving way caused secondary meniscus and joint cartilage damage. Therefore, conservative treatment of individuals with ACL injuries should be considered carefully.
Introduction
The anterior cruciate ligament (ACL) is important for knee stability, proprioception, and protection of internal knee structures. ACL rupture, a common knee-related injury, interferes with sports activities, especially in young athletes, and often results in pain, loss of function, and the knee giving way. ACL injuries do not heal spontaneously because of poor vascularization of the ruptured ligament and an unfavorable intra-articular environment. 1,2 Patients with a ruptured ACL have a high risk of secondary meniscal or cartilage injury, and chronic knee instability often causes early osteoarthritis. 3 –6 Reconstruction of ruptured ACLs has positive results and is the accepted procedure for most young, active patients.
Returning to competition within the same season after ACL reconstruction is difficult owing to long recovery times. Therefore, when athletes injure their ACL during the competitive season, but want to continue to play to the end of the season, they often opt for conservative therapy. 7 –9 Particularly, as for the athlete of the student, their senior year often becomes the last chance of the participation opportunity. How soon after therapy players can return to competition is unclear, as is their level of strength and risk of secondary meniscal or cartilage injury after return. The purpose of this study was to examine the conscious performance of young athletes to whom we provided conservative therapy for ACL injuries. Arthroscopic findings obtained during ACL reconstruction after the competition season were also reviewed.
Methods
This study was approved by the ethics committee of the Graduate School of Medical Science Kanazawa University. It consisted of 42 patients with ACL rupture from 2004 through 2011 (Table 1). The diagnosis of an ACL injury was reached based on a history of knee injury and the results of the Lachman and pivot shift tests. All patients underwent magnetic resonance imaging (MRI) to confirm the diagnosis of an ACL tear. All patients were injured during the competitive season; they strongly desired to continue to play to the end of the season and thus preferred conservative treatment. All patients were informed of the disadvantages of continuing competition after receiving conservative therapy. The inclusion criteria were a unilateral complete ACL tear and no previous knee ligament surgery, and the exclusion criterion was a multiple ligament injuries or meniscus tears with locking symptoms.
Patient demographics.

SD: standard deviation.
The study group contained 16 men and 26 women with a mean age of 17.1 ± 2.8 years (14–25 years). Thirteen of the 42 patients were basketball players, 10 were handball players, 4 were volleyball players, and 15 played other sports. All patients were students and competition level athletes (Table 1).
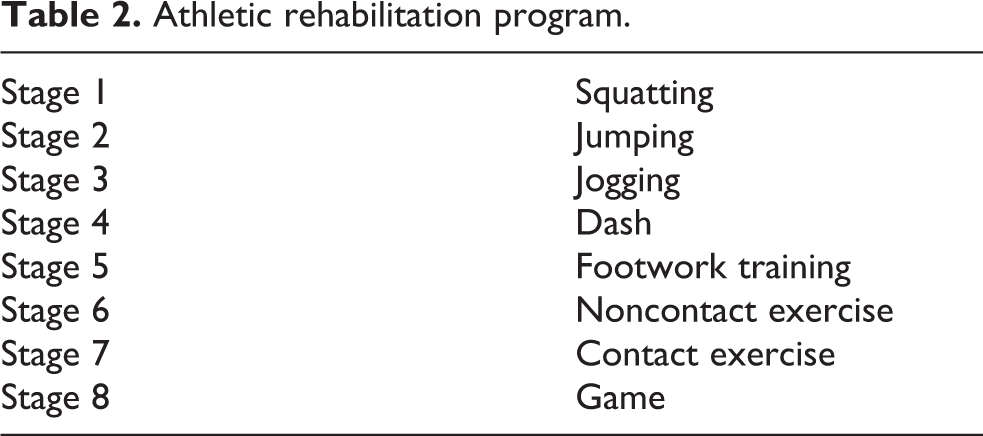
All patients underwent conservative treatment (athletic rehabilitation) with the aim of returning to competition within the same season. Rehabilitation consisted of eight steps to gradually build strength (Table 2). All patients wore an elastic ACL brace. Patients were allowed to return to competition when subjective and objective symptoms were absent, the rehabilitation program was completed, and the flexion and extension strength of the injured knee was 90% of that of the uninjured knee.
Athletic rehabilitation program.
In each patient, we determined the following: (1) the time required for return to competition after injury, (2) conscious performance after return, (3) whether or not the injured knee gave out during conservative treatment or after return to competition (example of a subjective symptom), and (4) the cause of performance deterioration if applicable. To determine conscious performance, patients were asked to rate (as a percentage) their performance after therapy relative to their performance before injury.
All patients received ACL reconstruction surgery after the competitive season. Arthroscopy was performed during reconstruction. The presence of meniscus tears and chondral injuries was determined retrospectively via examination of the arthroscopic videos and surgical records. In the videos, a meniscus tear was defined as the entrance of a probe into a tear. We defined chondral injury as International Cartilage Research Society grade 1 or higher.
Results
Thirty-eight of the 42 patients (90.5%) returned to competition after conservative treatment. The mean time to return was 13.8 ± 7.6 weeks (Figure 1), and the mean conscious performance percentage was 58.4 ± 16.5% (Figure 2). Thirty-eight patients (90.5%) experienced their knee giving way, of whom 36 (94.9%) stated that fear of their knee giving way hampered their performance.
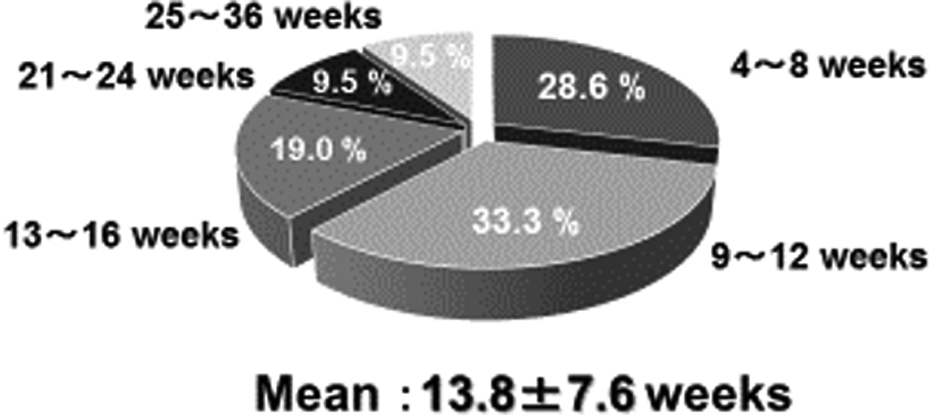
The mean time to return.

The mean conscious performance.
At the time of ACL reconstruction (mean, 5.1 months after injury), 9 of the 42 patients (21.4%) had a chondral injury (medial condyle, 7; both condyles, 2) and 22 (52.4%) had a meniscus injury (medial meniscus, 2; lateral meniscus, 13; both menisci, 7).
Discussion
Because long-term ACL injury increases the risk of secondary meniscus injury and cartilage damage, 3 –6 ACL reconstruction surgery is recommended for young athletes. 7 –9 However, some athletes with ACL injuries forego surgery so that they can finish out the season. Some investigators reported excellent results for conservative treatment. 10,11 For example, in a follow-up study of elite handball players 7.1 years after ACL damage, Myklebust et al. 12 found that 82% of players who received conservative treatment had returned to their preinjury game level. They suggested that players highly satisfied with conservative treatment continued to select this treatment. Degree of satisfaction may, however, reflect the sport; for example, satisfaction was low for sports requiring contact and pivot motion.
In our study, 90.5% (38/42) of the patients receiving conservative treatment were able to resume playing their sport 13.8 weeks (4–36 weeks) after injury. However, conscious performance was only 58.4%, and only two patients (4.8%) gave a rating of 100%. Unlike surgery, conservative treatment of ACL injury may not cure instability as manifested by a knee giving way. 6,13,14 In our study, 38 of 42 patients (90.5%) experienced this phenomenon, and 36 of the 38 mentioned fear of giving way as the cause of a fall. The persistence of instability is one of the reasons why athletes decide to undergo surgery after the season has ended. On the other hand, a small number of players with ACL injuries fully regain their preinjury performance levels without surgical intervention; however, a method for recognizing these players (termed “ALC-deficit copers”) at the time of injury has not been established. 15 We plan to investigate this issue, because we believe it is important to design strategies that accommodate athletes who wish to return to the field as quickly as possible.
People with ACL damage have a high risk of secondary meniscus and cartilage injury, which can significantly increase the risk of osteoarthritis. 7 In the study of Mitsou and Vallianatos, 16 meniscal involvement was noted in 24.4% of patients receiving surgery immediately after ACL injury; no articular cartilage involvement was observed. In situations where surgery was delayed, 61.6% of patients had meniscus injuries and 20–67.5% had articular cartilage injuries. In our study, 52.4% of the patients had meniscus injuries and 21.4% had chondral injuries at the time of ACL reconstruction (mean, 5.1 months after injury) (Figure 3). These injuries, whose incidence is difficult to estimate, may have resulted from knees giving way in many of patients. Therefore, conservative therapy for ACL injuries, with the aim of returning the player to the playing field as soon as possible, is not necessarily recommended and should be carefully considered.
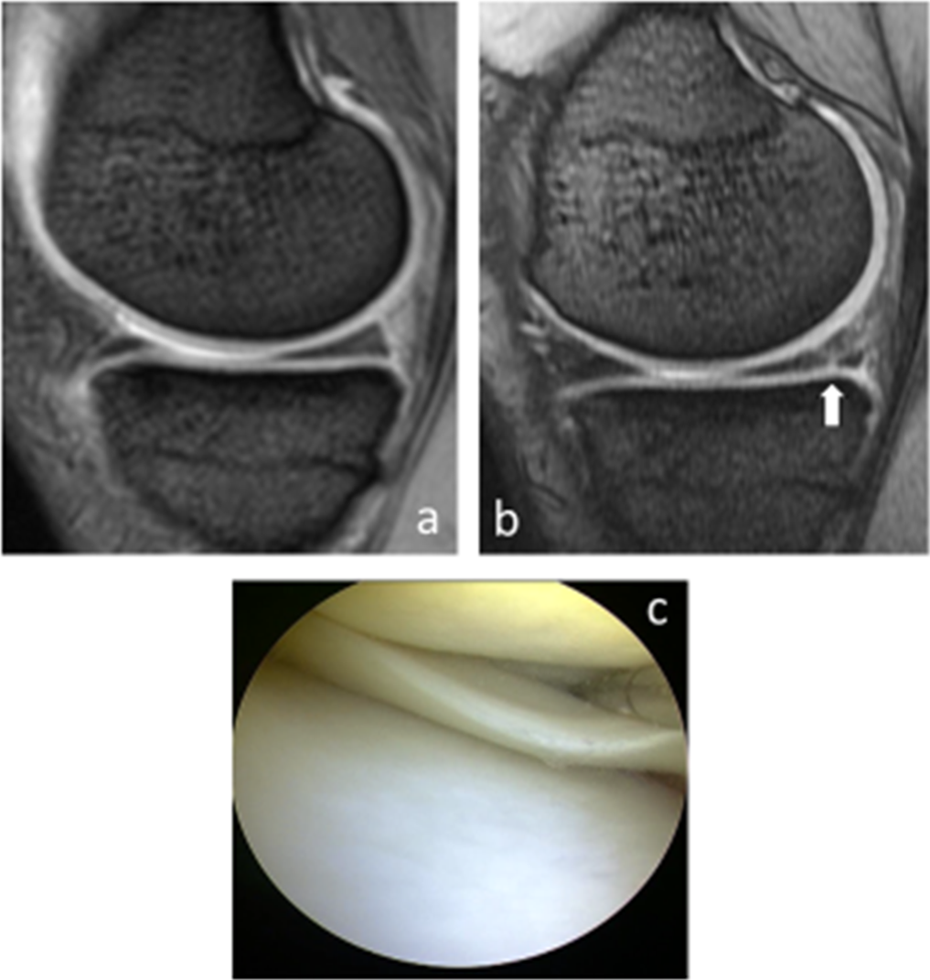
Results of a representative case. (a) T2-weighted magnetic resonance imaging of the right knee before conservative therapy did not show any obvious meniscus tears. (b) After the competition season, there was an obvious medial meniscus tear. (c) A longitudinal medial meniscus tear is detected via arthroscopy.
Our study had three limitations. First, many of the athletes included in the study participated in sports requiring contact and pivot motion (e.g. basketball and handball). In these sports, players need more stability in their knee joints, which may lower the overall conscious performance score. These sports also have a high risk of secondary meniscus and chondral injury. Second, it was unclear when the meniscus and cartilage injuries occurred (they were only examined at the time of surgery). It is difficult to determine the degree of meniscus and chondral injury at the time of injury using arthroscopy because of ethical issues. It is also difficult to compare magnetic resonance images because imaging is performed at different times after injury in each patient. Concurrent and secondary meniscus injuries are contained at the time of surgery. Third, our study was retrospective, and future prospective studies are needed.
Conclusion
Many athletes with injured ACLs returned to competition within the same season after conservative treatment. However, the mean conscious performance score was only about 60%. It is possible that knees giving way after treatment caused secondary meniscus and joint cartilage damage. Therefore, conservative treatment of athletes with ACL injuries should be carefully considered.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.