
Abstract
Objective:
To investigate the effects of intramedullary nail removal after tibial fracture repair.
Methods:
Sixty patients at our hospital were enrolled in a prospective study and divided into moderate/severe knee pain (visual analog scale (VAS) ≥ 4) and mild/no knee pain (VAS < 4) groups after interlocking intramedullary nailing. Variables studied included the distance from the tip of the nail to the tibial plateau and the front of the tibia on a normalized lateral X-ray, the VAS score of knee and ankle pain, the range of motion of the knee and ankle, and Johner–Wruhs criteria before, 6 weeks after operation, and at the last follow-up.
Results:
Fifty-seven patients were followed for a mean of 8.4 (2–17) months. In patients with moderate or severe knee pain intramedullary nail removal led to significant pain reductions (p < 0.05). A significantly shorter distance from the tip of the nail to the tibial plateau (<10 mm) and the anterior border of tibia (<6 mm) was found in the 24 patients with moderate or severe knee pain. Knee pain VAS scores significantly lowered 6 weeks postoperatively and at the last follow-up, compared to before the operation (p < 0.05). However, no significant changes occurred with respect to ankle pain VAS scores, range of motion, and Johner–Wruhs criteria (p > 0.05).
Conclusion:
For patients complaining knee pain after interlocking intramedullary nailing of tibial fractures, especially with a short distance from the tip of the nail tail to the tibial plateau (<10 mm) and the anterior border of the tibia (<6 mm) removal of the intramedullary nails relieved the pain significantly.
Introduction
Interlocking intramedullary nails have become the treatment of choice for tibial fractures, because their use is associated with minimal trauma, reliable fixation, and they also act as a stress shield. After the fracture heals, patients are generally advised to remove the implant due to the risk of breakage as a result of material fatigue and because they may cause symptoms such as anterior knee pain and articular dyskinesia. Some patients also want the implant to be removed for cultural reasons. Karladani et al. 1 followed 71 patients treated with intramedullary nails, and found that anterior knee pain was relieved in 39 patients after removal of the nails, but it became worse in 18 patients, indicating that the operation was not always harmless. Whalley et al. 2 reported some complications such as removal failure and postoperative infection and/or refracture, suggesting that there is still some controversy regarding the necessity of, and indications for, nail removal. Therefore, we designed a prospective study to explore the indications for and complications of intramedullary nail removal after tibial fracture repair using interlocking intramedullary nails.
Patients and methods
Patients
Sixty patients who had received interlocking intramedullary nailing at our hospital between June 2011 and December 2012 were enrolled in our study. Inclusion criteria included tibial or tibiofibular fracture treated with interlocking intramedullary nails. Exclusion criteria were (1) ipsilateral femur, tibial plateau, or ankle fracture; (2) limited range of lower limb motion or paraplegia; (3) knee ligament injury or presence of osteoarthritis; (4) experiencing trauma following nail removal.
The study was approved by the ethical committee of the Zhongda hospital southeast university and all participants provided written informed consent.
Surgical method
All patients underwent surgery for intramedullary nail removal by the same group of surgeons. They were placed in the supine position and received epidural or spinal anesthesia. After exsanguination, the two distal interlocking pins and one proximal pin were first removed using the original incision. Then, after exposing the tibial slope, the last proximal pin was taken out by attaching the puller to the end of the intramedullary nail and removing the intramedullary nail using a sliding hammer. Drainage was routinely placed, and it was removed 1 day postoperatively. The incision was closed, and pressure dressing was placed on the incision with an elastic bandage. Patients were instructed to do flexion-extension exercises in bed and partial weight-bearing exercises 3 days after the operation.
Variables measured
Radiographic parameters: To normalize the lateral X-ray, radiographs were scaled up using NEUSOFT PACS/RIS software, and the following variables were measured: (a) The distance from the tip of the nail to the tibial plateau; (b) The distance from the tip of the nail to the anterior border of the tibia (the measured value was recorded as the actual numerical value, and a negative value was recorded if the tip of the nail protruded outside the bone). In order to guarantee the accuracy of the data, measurements were made by two independent researchers, and the average value was recorded.
Pain scores: Visual analog scale (VAS) was used to assess pain in the knee and ankle before the operation, 6 weeks after the operation, and at the last follow-up.
Range of motion: The range of motion of the knee and ankle was measured before the operation, 6 weeks after the operation, and at the last follow-up.
Functional scores: Johner–Wruhs criteria were used to assess the therapeutic effect for patients compared to before the operation, at 6 weeks after operation and at the last follow-up.
Statistical analysis
All statistical analyses were performed with SPSS for Windows (Version 16.0., SPSS Inc., Chicago, Illinois, USA). Measurement data are expressed as mean ± SEM. Data obtained before and after the operation were compared and analyzed using Student’s t-test. Enumeration data (expressed as a percentage) were compared and analyzed using the χ 2 test. p < 0.05 was considered as statistically significant.
Results
A total of 60 patients were enrolled in the study: 34 males and 26 females; mean age 30.2 (24–59) years. There were 39 cases of tibial fracture and 21 cases of both tibial and fibular fracture. The fractures were caused by traffic injury (51), crush injury (5), and sports injury (4). There were 23 cases of open fracture, according to Gustilo typing: I (15) and II (8) and based on AO (Müller Arbeitsgemeinschaft für Osteosynthesefragen) typing there were 43-A2 (6), 43-B1 (5), 43-B2 (9), 43-B3 (28), 43-C2 (80), and 43-C3 (4) cases. Associated injuries included subarachnoid hemorrhage (2), nasal fracture (1), contusion of the kidney (1), and upper limb avulsion fractures (2). All of the associated injuries were treated conservatively. The mean interval between admission to hospital and surgery was 5.6 (1–8) days. Forty-eight fractures were treated by the transtendinous approach (TTA) and 12 by the paratendinous (PTA). The diameter of the nail averaged 9.7 (8–10) mm. The mean healing time was 4.3 (2–5) months, and no nonunion occurred. The nail was removed an average of 19.5 (12–30) months postoperatively (Table 1).
Patient characteristics.

TTA: transtendinous approach; PTA: paratendinous.
Fifty-seven patient were followed up for a mean of 8.4 (2–17) months. All wounds healed, and no postoperative infection or fractures occurred after interlocking intramedullary nail removal. Twenty-four of 57 patients reported moderate to severe knee pain (VAS ≥ 4). In this group of patients, the distances from the tip of the nail to the tibial plateau and the anterior border of the tibia were 8.2 ± 5.9 mm and −3.2 ± 3.5 mm, respectively. The same distances were 11.5 ± 5.3 mm and 5.5 ± 4.2 mm, respectively, in the other 33 patients, who reported mild or no knee pain (VAS < 4). The distances from the tip of the nail to the tibial plateau and the anterior border of the tibia were significantly shorter (<10 mm and <6 mm, respectively) on the normalized lateral X-ray in the 24 patients with moderate or severe knee pain (VAS ≥ 4) when compared with the 33 patients with mild or no knee pain (VAS < 4; p < 0.05, Table 2).
Correlation between knee pain and the distance from tip of the nail to the tibial plateau and the anterior border of the tibia.
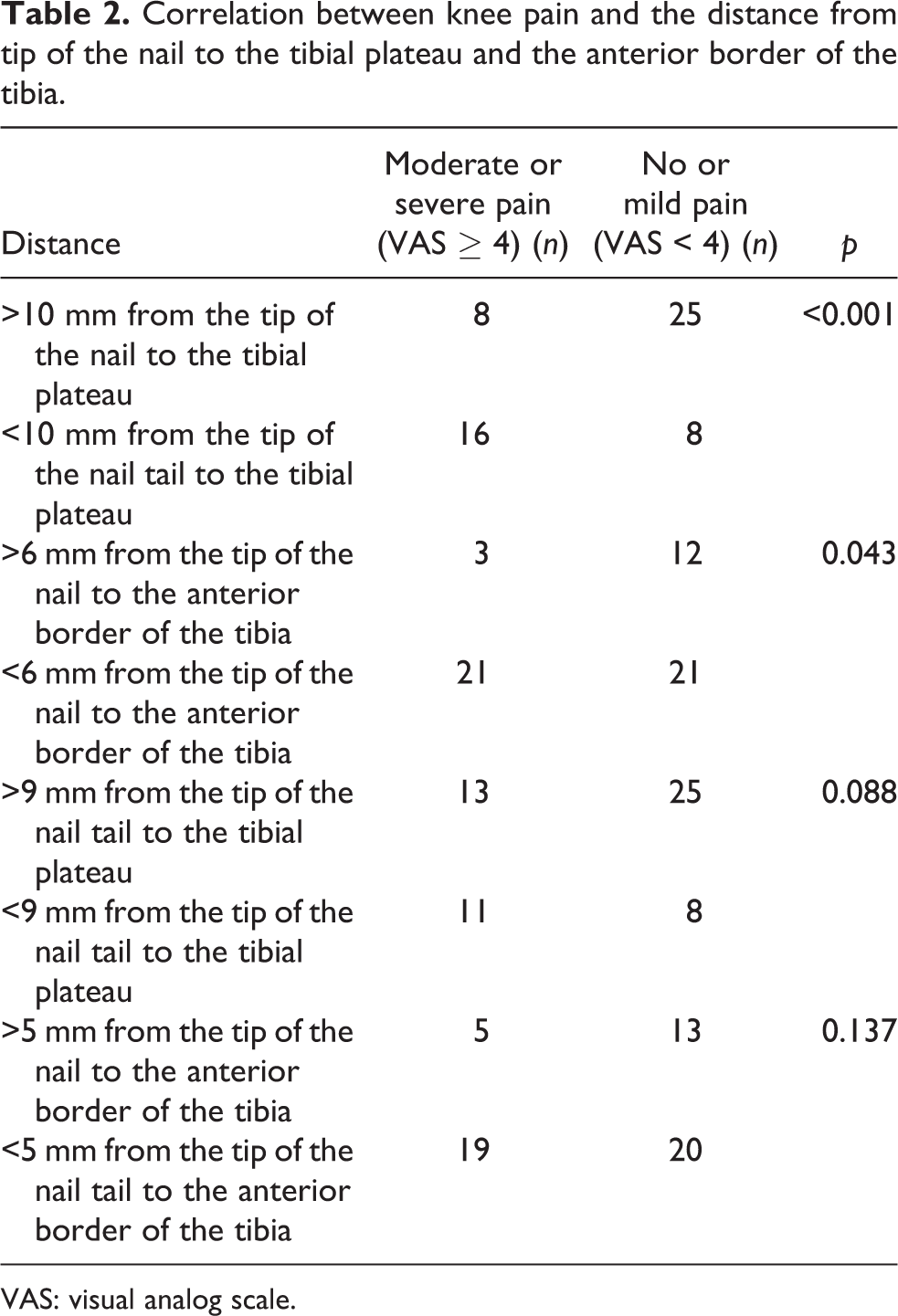
VAS: visual analog scale.
The VAS value for knee pain among the 57 patients decreased significantly from 3.4 ± 2.1 before the operation to 2.5 ± 1.4 6 weeks after the operation and 2.4 ± 1.3 at the last follow-up (p < 0.05, Table 3). In the subgroup of 24 patients with moderate to severe knee pain (VAS ≥ 4), the VAS value for knee pain also decreased significantly from 5.8 ± 0.9 before the operation to 4.3 ± 1.7 6 weeks after the operation and 3.6 ± 1.6 at the last follow-up (p < 0.05, Table 4). Intramedullary nail removal in the 24 patients with moderate to severe knee pain led to pain relief in 18 (75%), to pain increase in 0 (0%) and no change in 6 (25%) of the cases (p < 0.05, Table 5). No significant difference in ankle pain VAS score, knee and ankle range of motion, or Johner–Wruhs criteria was found at 6 weeks postoperatively when compared with that before the operation (p > 0.05, Table 6). Three of five patients with limited range of knee motion (<100i) showed improvement at the last follow-up, but without statistical significance. Five of 33 asymptomatic patients experienced knee pain after nail removal.
Range of motion and VAS pain scores for the knee and ankle before the operation, 6 weeks postoperatively, and at last follow-up.

VAS: visual analog scale.
aCompared with preoperatively p < 0.05.
Knee pain VAS scores in patients with moderate or severe knee pain preoperatively, 6 weeks postoperatively, and at last follow-up.
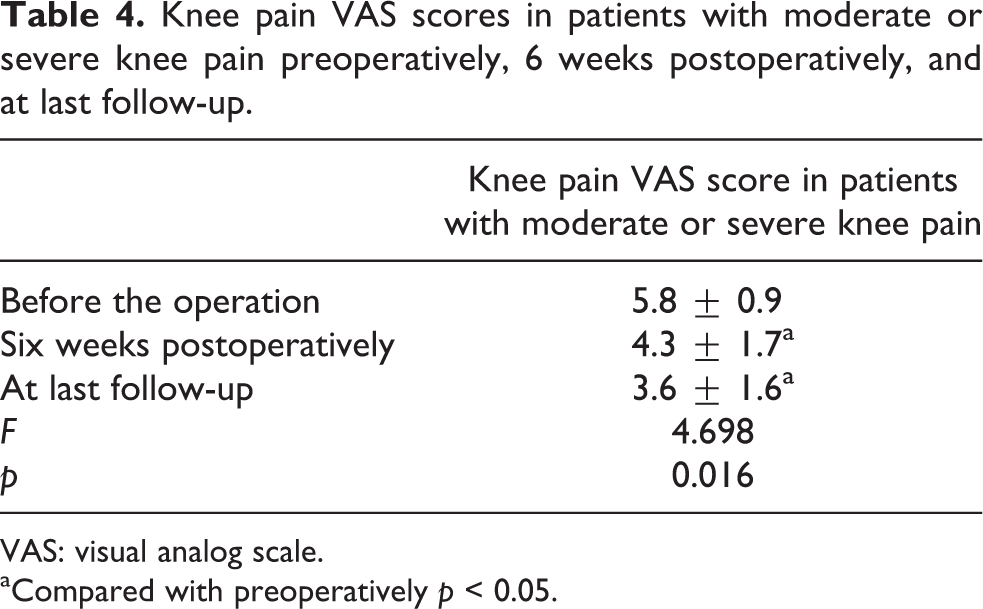
VAS: visual analog scale.
aCompared with preoperatively p < 0.05.
Changes of pain in patients with moderate or severe knee pain after intramedullary nail removal (n = 24).
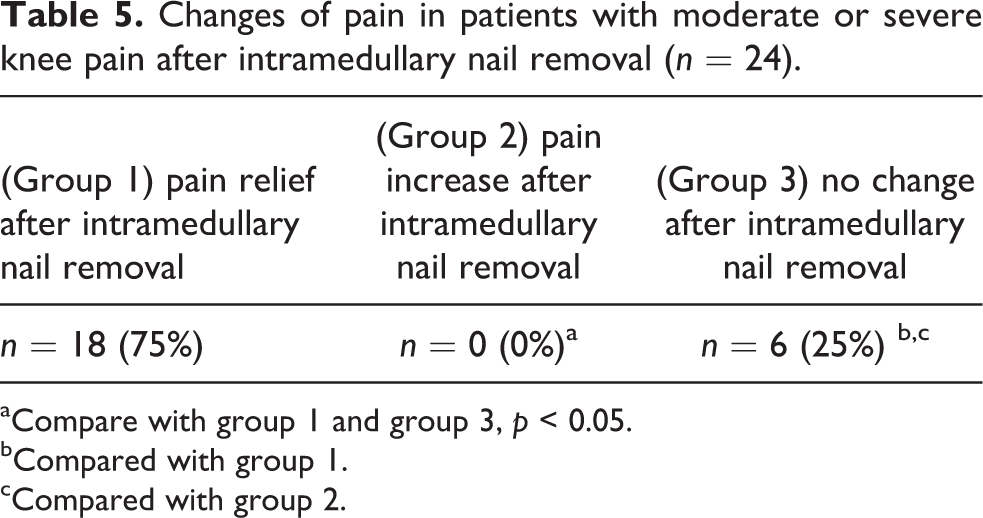
aCompare with group 1 and group 3, p < 0.05.
bCompared with group 1.
cCompared with group 2.
Johner–Wruhs criteria before the operation, 6 weeks postoperatively, and at last follow-up.

aCompared with preoperatively.
These results indicate that knee pain may be mainly due to the short distance from the tip of the nail to the tibial plateau (<10 mm) and to the anterior border of the tibia (<6 mm), as shown on the normalized lateral X-ray and removal of the intramedullary nail alleviated the pain in these patients (Figure 1).
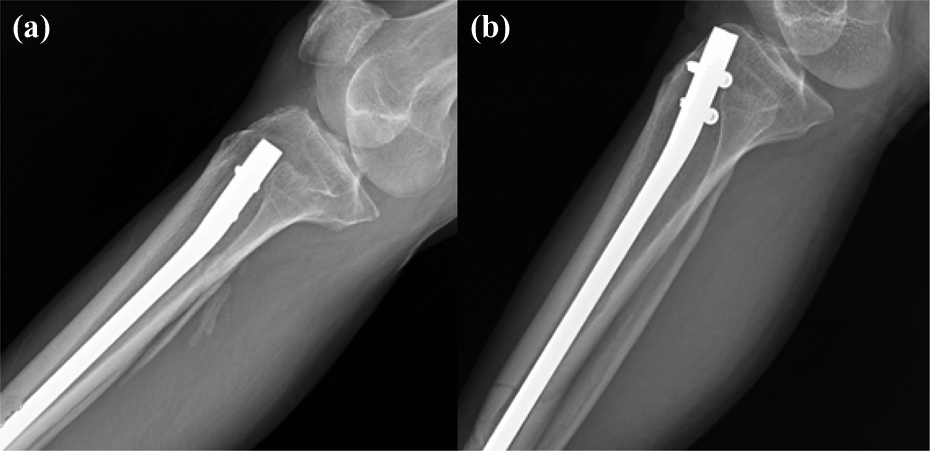
(a) A 37-year-old male patient with right tibiofibular fracture treated with interlocking intramedullary nail. The distance from the tip of the nail to the tibial plateau and the anterior border of the tibia was 4.33 and 10.59 mm, respectively. The knee pain VAS score was 2, and the range of knee motion was 135° before the operation. No significant changes occurred in these values at 6 weeks postoperatively. (b) A 52-year-old female patient with right tibiofibular fracture treated with interlocking intramedullary nail. The distance from the tip of the nail to the tibial plateau and the anterior border of the tibia was 6.9 and 3.7 mm, respectively. The knee pain VAS score was five points and the range of knee motion was 120° before the operation. The knee pain VAS score decreased to 2 at 6 weeks postoperatively, but the range of knee motion showed no improvement. VAS: visual analog scale.
Discussion
There is still some controversy as to whether or not the internal fixation should be removed after bone fracture repair. Busam et al. 3 suggested that the internal fixation should not be removed, because it is associated with a high rate of complications, such as infection, removal failure, and re-fracture. Kellan reviewed five case series studies and two retrospective cohort studies, and found that the internal fixation had been removed in about 30% of patients after surgery, of which about 50% was in the absence of clear indications. 4 However, they did not specify what they meant by “clear indications” for the removal of internal fixation. According to a report by Shen et al. 5 indications may include pain, infection, or patient preference. In our hospital, interlocking intramedullary nails were routinely removed after bone fracture repair, which makes it possible to investigate what kind of patients would benefit from this operation.
In our study, we found a significant reduction in knee pain VAS scores after removal of the intramedullary nail, which suggests that patients complaining of knee pain would benefit from removal of the intramedullary nail. However, no significant differences in ankle pain VAS scores, range of knee and ankle motion, and Johner–Wruhs criteria were found at 6 weeks postoperatively, when compared with those before the operation.
Further analysis has revealed that the incidence of knee pain was significantly greater in patients with a short distance from the tip of the nail to the tibial plateau (<10 mm) and anterior border of the tibia (<6 mm), indicating that the distance from the tip of the nail to the tibial plateau and the anterior border of the tibia played an important role in knee pain. Based on our experience, we posit that the knee pain may be due to the excessive length of the intramedullary nail used in the primary surgery. Specifically, the protruding tip of the nail can easily irritate the surrounding soft tissue, thereby resulting in knee pain.
In addition, we found that the tip of the nail did not often enter the knee joint cavity, so the range of knee motion was generally not limited. For the 24 patients with knee pain VAS > 3, we compared the VAS value at 6 weeks postoperatively and at last follow-up with that before the operation, and as might be expected, the VAS value was significantly lower at both time points. In fact, similar results were reported by Bhattacharyya et al., 6 who found that the incidence of pain was significantly less when the distance from the tip of the nail to the tibial plateau and the anterior border of the tibia were both above 1.25 cm. They also pointed out that having the appropriate depth of the tip of the nail below the bone cortex would make it easier to remove the nail in the future.
Darabos et al. measured the distance from the tip of the nail to the tibial plateau and tibia tuberosity on lateral knee X-rays in 220 patients treated with intramedullary nails, and they suggested that the position of the tip of the nail and its negative influence on the innervation pattern of the area dorsal to the patellar tendon could be the key factor in knee pain. 7
Our findings not only show the relationship between the distance from the tip of the nail to the tibial plateau and the anterior border of tibia, but also provide specific parameters for intramedullary nail surgery, especially in patients with a short distance from the tip of the nail to the tibial plateau (<10 mm) and the anterior border of the tibia (<6 mm).
Postoperative knee pain is a common complication with interlocking intramedullary nails. For example, Leliveld and Verhofstad 8 reported an incidence of 38% (27/71) for knee joint chronic pain. In our study, 24 of 57 patients suffered from moderate to severe knee pain (VAS ≥ 4), and the VAS score decreased significantly at 6 weeks postoperatively and at the last follow-up. However, removal of the intramedullary nail did not relieve the knee pain in all of these patients, and some patients without preoperative pain developed knee pain postoperatively. Therefore, the distance from the tip of the nail to tibial plateau or the anterior border of the tibia was not the only factor contributing to knee pain.
Labronici et al. 9 performed CT scans on 30 patients treated with interlocking intramedullary nails who had complained of knee pain postoperatively, and the results showed that the proximal interlocking pin entered the tibiofibular joint in 20 of these patients, which may be the iatrogenic cause of knee pain. In addition, Hemigou and Cohen 10 have shown that postoperative knee pain correlated with damage to the internal structure of the knee joint, including the nerves and the fat pad under the patella. There was a slope between the tibial tubercle and the anterior border of the tibial plateau, with transverse ligaments connecting the anterior edge of the medial and lateral meniscus on this slope, and a so-called safety zone for inserting the intramedullary nail existed on this slope. The anterior border of the tibial plateau, the transverse ligament, and the anterior horn of the meniscus were easily damaged if the entry point of the nail was beyond the safety zone.
Alsousou et al. 11 have confirmed that adhesion in the patellar tendon structure could lead to postoperative knee pain. We think that this finding could explain the new knee pain experienced by some patients in our study after removal of the intramedullary nail. Furthermore, Väistö et al. conducted an ultrasound study of the patellar tendon after tibial nailing to compare the changes between patients with and without anterior knee pain, and the results of this study suggest that the two different approaches (TTA and PTA) did not make any difference in this regard. 12 Therefore, in order to reduce the incidence of knee pain postoperatively in patients treated with intramedullary nails, the so-called safety zone should be identified, and an intramedullary nail with the appropriate length should be selected. The selection should be confirmed by a “C” arm machine, making sure that the tip of the nail does not extend into the knee or tibiofibular joint. The use of drainage is also recommended to prevent postoperative adhesion of the patellar tendon structure.
Conclusion
Our results show that removal of the intramedullary nail resulted in significant pain relief in patients complaining of knee pain after interlocking intramedullary nailing of tibial fractures, especially in those with a short distance between the tip of the nail and the tibial plateau (<10 mm) or the anterior border of the tibia (<6 mm) on normalized lateral X-rays. Close proximity of the tip of the intramedullary nail to these anatomical structures may be considered to be an indication for intramedullary nail removal after tibial fracture repair using interlocking intramedullary nails.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.