
Abstract
Purpose:
The second dorsal metacarpal (SDMC) perforator flap has been widely used for the soft tissue reconstruction of the hand. However, it is difficult to identify the depth and branches of the perforators of the second dorsal metacarpal artery (SDMA) using only handheld acoustic Doppler flowmetry (HADF), which is the most common method. The purpose of this study was to compare the results of examination by color Doppler ultrasonography (CDU) with those of HADF and to evaluate the efficacy of CDU for detection of the perforators to be used in the design of the SDMC flap.
Methods:
Twenty-two healthy volunteers (42 hands) were examined using both CDU and HADF. All locations identified as the perforators of the SDMA by the two examinations were mapped respectively.
Results:
The total perforator arteries detected with CDU in all hands were 111 branches, 49 branches of which could not be identified with HADF. The average number of perforators of the SDMA per hand found with CDU was 2.8 branches, while that for HADF was only 1.8 branches. The detection rates of the cutaneous perforators of the SDMA by CDU were 100% in the proximal one-third of the second metacarpal and 95% in the distal one-fourth of the second metacarpal.
Conclusion:
This study demonstrated the superiority of CDU compared with HADF for detection of the perforators of the SDMA. The CDU examination could easily identify the locations of the cutaneous perforators and help in the useful assessment of vascularity for the SDMC flap.
Keywords
Introduction
The second dorsal metacarpal (SDMC) perforator flap has been widely used to repair defects of the dorsum of the hand or the fingers since the first reports of Quaba and Davison in 1990. 1 –5 Many authors have reported that the SDMC perforator flap is an extremely useful and reliable surgical reconstructive method because of its advantages of matched color, thickness and texture. 1,2,4,5 Precise identification and evaluation of the course of the cutaneous perforators are essential components of a successful perforator flap transfer, in order to reduce complications and operating times and to provide an overall better result. 6 –9
Currently, handheld acoustic Doppler flowmetry (HADF) represents the traditional and most common method of identifying the perforators of the second dorsal metacarpal artery (SDMA). 10 –12 However, it is difficult to evaluate up to the depth, path, branching and orientation of the perforators by HADF. 8,10 –14 Additionally, some authors have reported that a disadvantage of HADF has often been poor concordance between the perforator positions detected by HADF and the locations of the perforators identified clinically. 8,13,14
Recently, color Doppler ultrasonography (CDU) has been widely and successfully used for the planning and design of the various perforator flaps. 6 –9 Many authors have reported that CDU is a useful non-invasive, reliable, easy and highly sensitive technique for evaluation of the perforator flaps harvested for reconstructive surgery. 6 –9
Despite the efficacy of the CDU examination in the detection of the perforator arteries for the planning of perforator flaps, there has been little research detailing the specific location of the perforators for the SDMC flap using CDU.
The purpose of this study was to compare the results of examinations by CDU with those of HADF, to evaluate the efficacy of CDU for detection of the perforators to be used in the design of the SDMC flap and to clarify the locations of the perforators of the SDMA.
We considered that CDU examination might easily identify the locations, numbers and courses of the cutaneous perforators, and this CDU information would provide a better knowledge and understanding of the distribution of the perforators of the SDMA to help in the planning and design of SDMC flaps.
Materials and methods
Twenty-two healthy volunteers (44 hands; 22 men, age range 24–56 with a mean age of 37.3 years without any histories of traumatic injuries) were examined using both HADF and CDU to map points where the cutaneous perforators of the SDMA were located. After signed consent was obtained from all participants in this study, we carried out those examinations for both wrists.
During the examination, the participants were sitting with the forearm in about 90° pronation, the elbow in about 45° flexion and the shoulder in about 30° abduction position. All examinations were performed by a single orthopedic surgeon (MN).
Handheld acoustic Doppler flowmetry
A flowscope model 820 apparatus (Hadeco Co. Ltd, Kawasaki, Japan) was used. The transducer was placed on the dorsal side of the hand between the second and third metacarpals, and moved from the level of the metacarpal head to its base, to identify the perforators of the SDMA. The locations of the loudest signals, where the perforators were thought to penetrate the fascia of the interosseous muscle, were marked on the skin.
Color Doppler ultrasonography
An ultrasound scanner (Mylab Five, Hitachi Medical Corporation, Tokyo, Japan) equipped with an LA332 3.5/12 MHz Hi-Definition linear array transducer (LA332) was used. The probe was placed on the dorsal side of the hand between the second and third metacarpals, and moved perpendicularly to the surface skin of the dorsal hand from the level of the metacarpal head to its base, to identify the perforators of the SDMA by both longitudinal and transverse ultrasonographic imaging. The locations and the numbers of the perforators penetrating the interosseous muscle fascia were marked on the skin.
Additionally, the distance (X) between the head of the second metacarpal and the points marked for both the HADF and the CDU locations was measured. In order to correct for individual differences, the ratio (x) of distance (X) to the second metacarpal length (A) was measured and defined as the location ratio of the perforator. These bony landmarks, which are the head and the base of the second metacarpal, were easy to identify by palpation and the CDU in all hands. Moreover, these locations mapped with the CDU were compared with those of the HADF.
We also confirmed the existence of the cutaneous perforators and the intramuscular perforators with the CDU, which we could not do with the HADF.
Results
Handheld acoustic Doppler flowmetry examination
Perforators of the SDMA were located in all 22 healthy volunteers. The numbers of the perforators mapped with HADF were one branch in 10 hands, two in 33 hands and three in 1 hand. The average number of the perforators mapped with HADF was 1.8 branches per hand. The total number of the perforators was 79 branches in 44 hands. Of those, 68 perforators (86.1%) were also identified at the same locations as perforators identified with the CDU. The corrected locations of the perforators detected with HADF were as shown in Figure 1. Moreover, as to the other 11 points mapped with HADF, no perforator was identified by the CDU. As to all those 11 points, the CDU could detect the cutaneous perforator precisely distally or proximally or the bifurcation of the perforator from the SDMA.
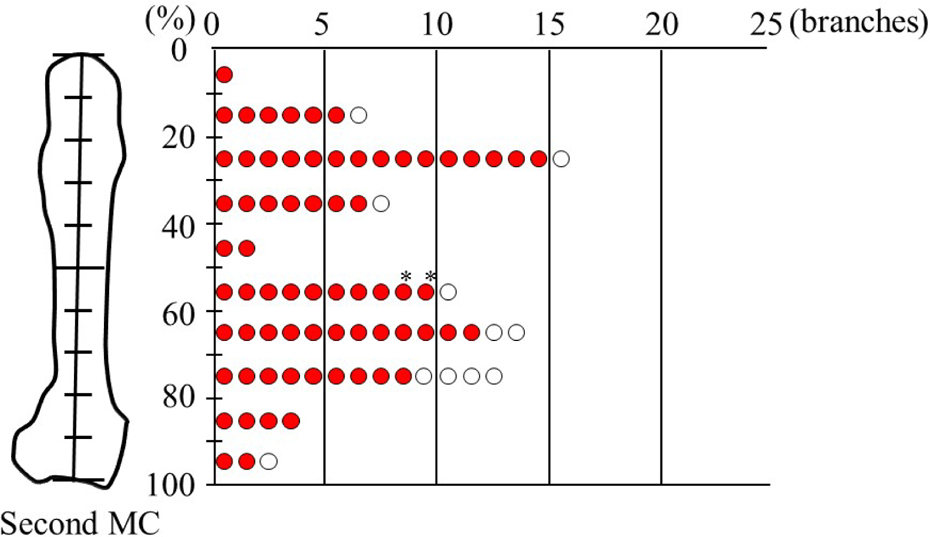
Location of the perforators detected using HADF. Red circle: perforators that were also identified by CDU; white circle: perforators that were not identified by CDU; *Intramuscular perforators that were identified by CDU. HADF: handheld acoustic Doppler flowmetry; CDU: color Doppler ultrasonography.
Color Doppler ultrasonography examination
The numbers of the perforators mapped with the CDU were one branch in 2 hands, two in 17 hands, three in 16 hands, four in 8 hands and five in 1 hand. The average number of the perforators mapped with the CDU was 2.8 branches per hand. The total number of the perforators was 121 branches in 44 hands. The corrected locations of the perforators detected with the CDU were as shown in Figure 2. Of them, 44 perforators (36.4%) could not be identified by HADF. In addition, there were 114 cutaneous perforators (94.2%) that penetrated the fascia. The remaining seven perforator arteries were intramuscular perforators (5.8%) that did not penetrate the fascia on the CDU examination. Of seven perforators, two were mistakenly identified as cutaneous perforators from the HADF.
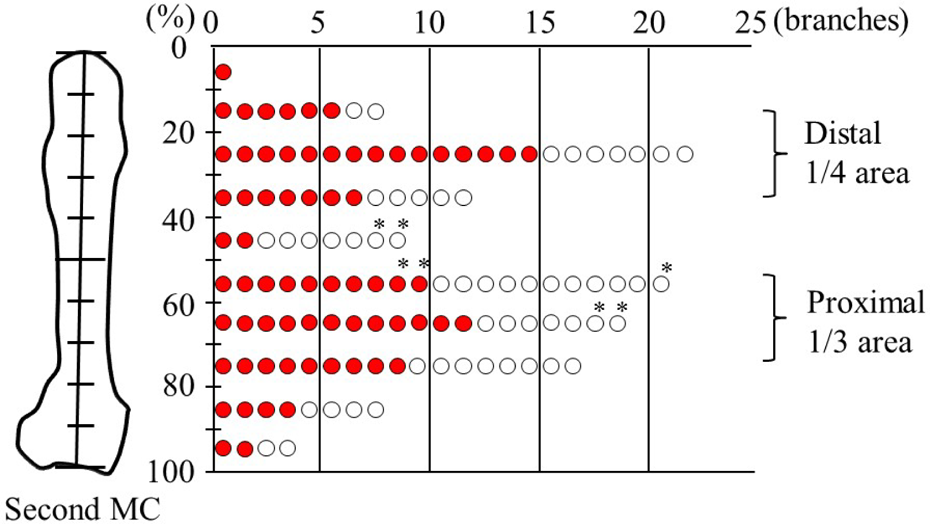
Location of the perforators identified using CDU. Red circle: perforators that could be also detected by HADF; White circle: perforators that could not be detected by HADF; *Intramuscular perforators that were identified by CDU. CDU: color Doppler ultrasonography; HADF: handheld acoustic Doppler flowmetry.
The CDU could identify the locations, numbers and the courses of the perforator branches and whether they were cutaneous or intramuscular perforators.
In all hands, one or more of the cutaneous perforators of the SDMA by the CDU was detected in the proximal one-third of the second metacarpal. Moreover, 38 of 40 hands (95%), one or more of the cutaneous perforators of the SDMA by the CDU were detected in the distal one-fourth of the second metacarpal level. That is to say, more than one perforator was able to be identified at the proximal one-third and/or distal one-fourth of the second metacarpal in all hands by the CDU examination.
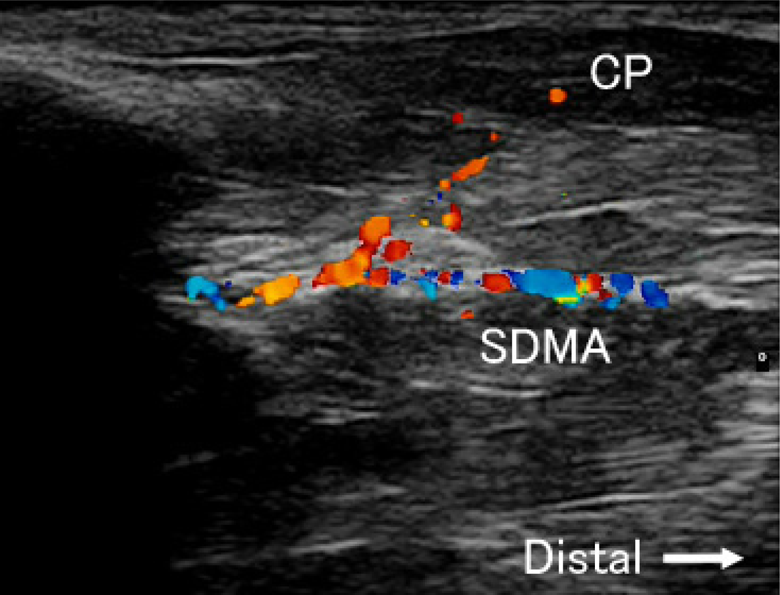
The typical cutaneous perforator identified by the CDU at the distal of the metacarpal on the longitudinal and the transverse imaging were as shown in Figures 3 and 4. The typical cutaneous perforator identified by the CDU at the proximal of the metacarpal on the longitudinal imaging was as shown in Figure 5.

CP of the SDMA at the distal of the metacarpal on the longitudinal CDU imaging. CDU: color Doppler ultrasonography; SDMA: second dorsal metacarpal artery; CP: cutaneous perforator.
CP of the SDMA at the distal of the metacarpal on the transverse CDU imaging. CDU: color Doppler ultrasonography; SDMA: second dorsal metacarpal artery; CP: cutaneous perforator; 2MC: second metacarpal; 3MC: third metacarpal.

CP and IMP of the SDMA at the proximal of the metacarpal on the longitudinal CDU imaging. CDU: color Doppler ultrasonography; SDMA: second dorsal metacarpal artery; CP: cutaneous perforator; IMP: intramuscular perforator; SDMA: second dorsal metacarpal artery.
Discussion
The SDMC perforator flap is highly useful and excellent to cover the skin defect in the dorsum of the hand, because elevating the flap can preserve the main artery of the SDMA. 1 –5 Conversely, this perforator flap has a disadvantage of the difficulty associated with finding appropriate perforators due to anatomical variation, and the small, thin cutaneous perforators of the SDMA. 1 –5
Presently, the most common method of mapping SDMC perforators has been the conventional HADF using a pencil-type Doppler probe. 10 –12 HADF is a non-invasive, simple and portable method, which makes it easy to perform in most hospitals. 8,13,14 However, this examination often misidentifies or misses arteries, particularly in evaluating small perforators, and perforators running obliquely from the muscle to the skin, making this technique unreliable. 8,13,14 Tsukino et al. reported that there is only a 40% concordance rate between preoperative perforators and those found intraoperatively by HADF. 8 Shaw et al. also described that HADF resulted in a large underestimate (30%) or overestimate (150%) of the location and number of the perforators. 15
Recently, for planning and designing of the various perforator flaps, the CDU has been the most commonly used method of preoperative perforator mapping, providing predictive information regarding the blood-flow characteristics of the cutaneous perforators. 6 –9 The CDU is non-invasive and effective for evaluating the location, number, depth and course of cutaneous perforators, although the disadvantage is that it requires the experienced examiner and the learning curve to be skilled at detecting the perforators. 6 –9 In addition, the high cost associated with the procedure limits its availability in some hospitals. 6 –9 Tsukino et al. reported that all the points identified with the CDU for the anterolateral thigh perforator coincided with the actual perforators and there were no misidentifications or missed arteries. Their concordance rate was 100%. 8 Dorfman et al. examined the value of CDU for reliability in identifying the perforators of the anterolateral thigh flap. They reported that all visualized perforators were identified in flap elevation (sensitivity, 100%) and all the flaps were successfully elevated including the identified perforators. 6 No unexpected operative plan change was needed. 6
The present study describes the usefulness of the preoperative CDU evaluation in the harvesting of the SDMC perforator flap and clarifies the location of the cutaneous perforators of the SDMA. Additionally, the examination by CDU was compared with that by HADF, in order to evaluate the efficacy of the CDU for detection of the perforators for the planning of the SDMC perforator flap. Consequently, the CDU identified approximately 1.5 times the number of cutaneous perforators detected by HADF. Sixty-eight perforators (86.1%) mapped with HADF agreed with the perforators identified by the CDU. There were 11 false-positive HADF results, attributable to perforator branching at skin level, and 44 (36.4%) false-negative results, including the perforators that were missed. This is because the perforators often run obliquely from the muscle to the skin. Besides, these perforators may be intramuscular, not the cutaneous ones, which are necessary for the SDMC flap. The HADF is unable to distinguish between these two courses, and thus often misidentifies or misses the cutaneous perforators. Tsukino et al. also compared the examination of the CDU with that of the HADF in patients receiving anterolateral thigh flap. 8 The HADF is similarly inferior to the CDU in preoperative perforator evaluation because it cannot provide accurate information on the subcutaneous tissue. 8 Cheng et al. examined two systematic reviews of clinical trials of the HADF and the CDU. 9 These two reviews found that the sensitivity and positive predictive value of the CDU is, respectively, 6% and 7% higher than the HADF. 9 This study also revealed the superiority of CDU to HADF for preoperative planning of the SDMA perforator flap elevation. Moreover, the CDU could provide detailed information on the location and the depth of the SDMA perforators as well as their course before raising the flap.
There are some detailed anatomical studies of SDMC perforator flaps. Quaba and Davison demonstrated that the perforators of the SDMA arose approximately 1 cm proximal to the metacarpal head. 4 Lai-Jin et al. described that two pivot points were 2.5 and 1.5 cm proximal to the edge of the second web space in 34 cadaveric specimens. 1 These reports described that the cutaneous perforators of the SDMA were almost all located at approximately 1–1.5 cm proximal to the metacarpophalangeal joint, namely at the distal one-fourth of the second metacarpal, similar to our findings. Although those authors have evaluated the location of the cluster or the pivot points of the SDMA perforators, they have not corrected for individual differences by the size of the metacarpal. In addition, they measured the perforator points using no bony landmark. 1,2 In the current study, all data evaluated were corrected for the length of the metacarpal. Consequently, more than one cutaneous perforator of the SDMA could always be found at the distal one-fourth of the second metacarpal in all hands with the CDU examination. To better understand the detailed location of the perforators, bony landmarks should be used to examine the distribution of the perforators of the SDMA. Identification of these perforator locations and pivot points can be helpful in the planning of the SDMC flap to repair lesions in the dorsal hand and to confirm that the perforator length will be sufficient to cover the defective area.
In addition, Omokawa et al. reported on their cadaveric study that the number of the cutaneous perforators of the SDMA at the proximal, central and distal thirds of the metacarpal averaged 1.6, 1.2 and 3.4, respectively. 3 They also described that the average diameter of the perforators was 0.12–0.16 mm in their cadaveric study. 3 These findings indicate that the distal perforators contribute most to the cutaneous vascularity of the SDMC flap. However, the numbers of the SDMA perforators found using the CDU in the current study were less than those described by Omokawa et al. 3 We consider that this is because the CDU equipped with the most widely used 12 MHz transducer was used in this study. Kimura et al. stated that it is difficult to visualize all the cutaneous perforators of the SDMA owing to the resolution limit with less than 30 MHz transducer of the ultrasound. 16 Tsukino et al. also reported that the CDU examination is the most reliable for the identification of perforators approximately 1 mm in diameter in planning flap surgery. 7
The present study had several limitations. First, we did not intraoperatively evaluate the true perforator points of the SDMC flap, in the current study. Consequently, it is impossible to investigate false-positive perforators. We plan to perform the intraoperative examination, and to compare between the preoperative and the intraoperative findings statistically. Second, a weakness of the current study was the reproducibility of the ultrasound examination. All examinations were performed by a single examiner. Therefore, we could not evaluate interobserver reliability. Ultrasound examination is known to be examiner dependent. This remains for future studies.
Conclusions
This study demonstrated the superiority and the usefulness of CDU compared with HADF for the detection of the perforators of the SDMA and the distribution characteristics of its cutaneous perforators. The CDU examination could easily identify the locations, numbers and the courses of the cutaneous perforators and help in the useful assessment of vascularity to confirm the existence and location of appropriate perforators for the design of the SDMC flap. Using this CDU examination, difficulties owing to the anatomical variation of the SDMA perforator are easily overcome, simplifying SDMC flap harvest. We recommend that the flap including these cutaneous perforators be designed using CDU for planning the SDMC flap.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.