
Abstract
Objective
This study aimed to characterize the ultrasound (US) imaging features of breast tuberculosis (BTB) to clarify the process of disease progression and provide valuable clinical information.
Methods
We retrospectively reviewed 45 patients with pathologically or GeneXpert-confirmed BTB from January 2010 to December 2017. We assessed the US features of target lesions including size, shape, orientation, margin, echogenicity, calcification, posterior acoustic features, and blood-flow signal.
Results
The patients were classified with nodular (55.5%, 25/45), abscess (15.6%, 7/45), or sinus (28.9%, 13/45) type according to their US features. Forty lesions (88.9%, 40/45) extended in a parallel orientation and five extended in a non-parallel orientation. Calcifications were found in eight cases, including six macrocalcifications and two microcalcifications. Enlarged axillary lymph nodes were observed in three cases (6.7%, 3/45). In addition, 44 of the 45 cases (97.8%, 44/45) exhibited hypovascularity or avascularity according to color Doppler flow imaging (CDFI).
Conclusion
BTB lesions can be classified as nodular, abscess, or sinus type according to their US imaging features. Poor blood supply detected by CDFI might be a common US feature of BTB. Characterization of its US features may facilitate the clinical diagnosis of BTB.
Introduction
Breast tuberculosis (BTB) was first reported by Cooper in 1829. Breast tissue appears to be resistant to tuberculosis (TB) infection because of its unfavorable environment for the survival and proliferation of tuberculosis bacteria.1,2 The incidence of BTB is thus low, ranging from 0.1% to 0.52%. 3 However, the incidence has been gradually increasing as a result of increasing numbers of multidrug-resistant tuberculosis bacteria, increasing numbers of patients with immunocompromised disorders such as acquired immunodeficiency syndrome, especially in developing countries, and increasing immigration from regions where TB is prevalent.3–8 BTB is a rare form of extrapulmonary TB, accounting for approximately 0.1% of all breast diseases and 3% to 4.5% of surgically-treated breast disorders in developing countries. 9 The clinical manifestations of BTB are complex and unspecific, making it difficult to differentiate from other breast disorders such as breast cancer and breast sclerosing adenosis.1,10 Ultrasound (US) imaging is crucial for identifying breast lesions, and characterizing the US imaging features of BTB lesions may thus facilitate its diagnosis. However, few studies to date have reported on the use of US to characterize BTB lesions. In the present study, we retrospectively characterized the US imaging features of 45 patients with BTB to further our understanding of the disease progression and to provide valuable information for its clinical diagnosis. To the best of our knowledge, this is the largest study of US applied in patients with BTB to date.
Patients and methods
Patients
We retrospectively reviewed patients diagnosed with BTB who underwent US examinations from January 2010 to December 2017 at Zhejiang Integrated Traditional and Western Medicine Hospital, China. This study was approved by the institutional review board of Zhejiang Integrated Traditional and Western Medicine Hospital, China and all patients provided written informed consent.
Ultrasound examination
Patients were examined using a Philips IU22® Ultrasound instrument (Philips, Amsterdam, The Netherlands) with a L12-5 probe (corresponding frequency 5.0–12.0 MHz) or an Acuson Sequoia 512 instrument (Siemens Medical Solutions, Mountain View, CA, USA) with a 15L8W probe (corresponding frequency 8.0–15.0 MHz). The pulse repetition frequency was 750 Hz, filter M, and gain 250. Sonography-guided core-needle biopsy and fine-needle aspiration cytology were performed using a BARD® MAGNUM® instrument with 18G and 20G core needles, respectively (Bard Peripheral Vascular, Inc., Tempe, AZ, USA). To fully expose the bilateral breasts during US examination, patients were kept in a supine or lateral position with their hands placed symmetrically beside a pillow. Enclosed breast masses, nipple discharge, or skin sinus tracts were identified by the naked eye. All patients underwent routine US examination of bilateral breasts and axillary lymph nodes at least twice, in a radial pattern. We performed biopsy via an 18G biopsy needle for nodular BTB lesions, and aspiration for GeneXpert examination (Cepheid, Sunnyvale, CA) via a 20G needle prior to biopsy for lesions with cystic components. The findings of the US examinations were retrospectively reviewed by two radiologists with at least 5 years of experience. The US features of the lesions, including position, shape, margin, orientation, echogenicity pattern, posterior acoustic features, calcification, and vascularity, were analyzed and recorded.
Blood supply examination
The blood supply and blood distribution of the lesions were evaluated using color Doppler flow imaging (CDFI). According to the Adler flow categorization, 11 the blood flow of the mass was classified into four categories: 0, avascular; I, one or two pixels containing blood flow; II, one main vessel in the area and/or several small vessels; and III, ≥4 vessels or diffuse reticular flow. In addition, alterations of axillary lymph nodes were also evaluated by US imaging.
Data analysis
All data were presented as mean ± standard deviation.
Results
We retrospectively reviewed the breast lesions in 45 female patients diagnosed with BTB. The patients’ demographic and clinical data are summarized in Table 1. Of these 45 patients, 17 were diagnosed pathologically, eight by GeneXpert examination, and the other 20 by both pathology and GeneXpert examination. Twenty-six of the 45 cases had palpable masses, 13 had breast skin thickening and ulceration, two had breast pain, and five had fatigue, low fever, and night sweats. Twenty-three patients also had pulmonary TB and two had pelvic TB. In addition, 10 had a history of pulmonary TB, three had a history of lymphatic TB, two had a history of BTB, and the other five had no history of either TB or TB involving other organs.
Demographic and clinical data of patients with breast tuberculosis (n = 45).
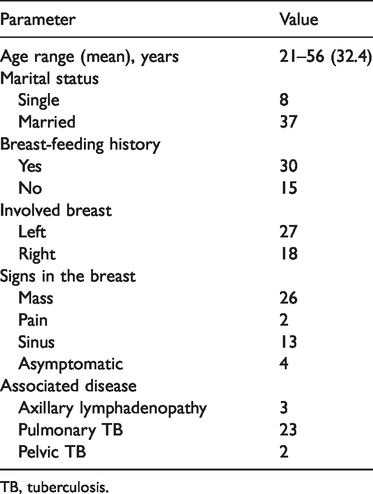
TB, tuberculosis.
All 45 cases had unilateral BTB lesions (Table 1). The locations and extents of the lesions are given in Table 2. The maximal diameters of the BTB masses ranged from 0.5 to 3.8 cm (mean 1.5 ± 0.7 cm). Three patients (6.7%, 3/45) had enlarged multiple ipsilateral axillary lymph nodes with a maximum short-axis diameter >0.6 cm. These involved lymph nodes were further proven to be lymphatic TB nodes via biopsy.
Ultrasound features of breast tuberculosis masses (n = 45).

The 45 BTB lesions were classified into one of three types based on their US imaging features. Type I, nodular type (Figures 1–5): 25 cases (55.5%, 25/45) with internal heterogeneous hypoechogenicity (11/25) or complex echogenicity (14/25), including 18 oval, two round, and five irregular lesions; 16 of the 25 cases (64.0%, 16/25) had a disease course of ≤6 months and nine (36.0%, 9/25) had a disease course >6 months. Type II, abscess type (Figure 6): 7 cases (15.6%, 7/45) with thick-wall cysts with oval shapes and posterior acoustic enhancement, including two (28.6%, 2/7) with internal punctate hyperechogenicity that were movable under probe pressure; five of the seven cases (71.4%, 5/7) had a disease course of ≤6 months and two (28.6%, 2/7) had a disease course >6 months. Type III, sinus type (Figures 7,8): 13 cases (28.9%, 13/45) with internal heterogeneous echogenicity, including 11 extending in a parallel pattern and two in a non-parallel pattern, all irregular with a cord-like hypoecho extending to the surface of the breast skin; three (23.1%, 3/13) cases had a disease course of ≤6 months and 10 (76.9%, 10/13) had a disease course >6 months. In addition, eight of the 45 cases (17.8%, 8/45) exhibited calcifications, including six macrocalcifications and two microcalcifications. In one case, the calcification increased from 0.4 to 0.8 cm after 3 months.

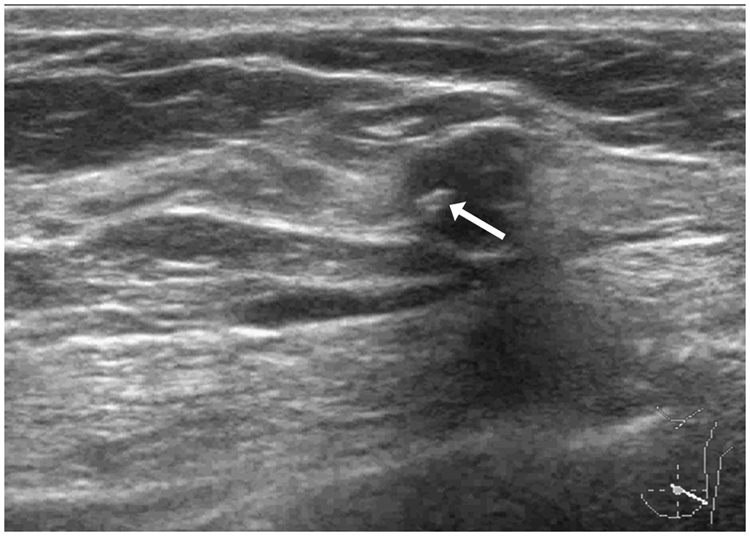
Sonographic appearance of a 43-year-old woman with nodular breast tuberculosis. (a) Ultrasound demonstrated a well-defined oval nodule, with internal anechoic area (arrow) and posterior acoustic enhancement. (b) Color Doppler flow imaging demonstrated two pixels containing blood flow in the margin of the nodule (arrows), with blood flow classified as category I based on the Adler categorization.

Sonographic appearance of a 28-year-old woman with nodular breast tuberculosis. (a) Ultrasound imaging of the right breast demonstrated an ill-defined irregular ‘starfish’-like nodule in the upper inner quadrant, with a large internal anechoic region and posterior acoustic enhancement (arrow). (b) Color Doppler flow imaging demonstrated one pixel containing blood flow in the margin of the lesion (arrow), with blood flow classified as category I based on the Adler categorization.

Sonographic appearance of a 32-year-old woman with nodular breast tuberculosis. Ultrasound imaging of the left breast demonstrated a hypoechoic nodule extending in a parallel orientation in the upper inner quadrant, with a circumscribed margin and internal heterogeneous echo. A punctate hyperechoic microcalcification was detected inside the nodule (arrow).
Sonographic appearance of a 36-year-old woman with nodular breast tuberculosis. Ultrasound imaging of the left breast demonstrated a round ill-defined hypoechoic nodule extending in a non-parallel orientation in the lower outer quadrant. A hyperechoic macrocalcification was detected inside the nodule (arrow), with 1-mm diameter and posterior acoustic shadowing.

Sonographic appearance of a 44-year-old woman with nodular breast tuberculosis. Ultrasound imaging of the right breast demonstrated an irregular hypoechoic nodule extending in a non-parallel orientation in the lower outer quadrant, with an angular margin (arrows).

Sonographic appearance of a 28-year-old woman with abscess breast tuberculosis. Ultrasound imaging of the right breast demonstrated an ill-defined oval nodule, with posterior acoustic enhancement and disseminated internal punctate hyperecho (arrow), which move with probe pressure.

Sonographic appearance of a 30-year-old woman with sinus breast tuberculosis. Ultrasound imaging demonstrated a complex mass mainly composed of cystic components, with posterior acoustic enhancement extending to the breast skin and forming a sinus (arrow).

A 36-year-old woman with sinus breast tuberculosis. (a) Ultrasound imaging of the left breast demonstrated an irregular hypoechoic mass extending in a non-parallel orientation in the lower outer quadrant, presenting a ‘crater’-like sinus connecting the breast mass to the localized breast skin (arrows). (b) Color Doppler flow imaging demonstrated a few pixels containing blood flow in the margin of the mass (arrow), and the blood flow was classified as category I based on the Adler blood flow assessment. (c) The breast skin was thickened and ulcerated with light yellow pus discharging (arrow), as seen by the naked eye.
Blood flow was classified according to Adler category by CDFI (Table 2).
Discussion
BTB is classified as primary or secondary, depending on its origin. Primary BTB is extremely rare and results from direct infection via the breast ducts opening to the nipple or from breast skin abrasions. 12 Secondary BTB is much more common and has three main routes of spread: 1) direct spread by extension from surrounding TB lesions such as in the sternum, costa, pleural, and mediastinum; 2) retrograde lymphatic spread from TB lesions in the ipsilateral axillary, neck, chest, supraclavicular, and subclavian nodal regions; and 3) hematogenous spread from TB lesions such as mesenteric lymphatic TB via the blood circulation. The direct and retrograde lymphatic routes are the most common spread routes of secondary BTB.12,13 In the current study, five patients (11.1%, 5/45) showed no significant abnormalities in any organs except the breast and had no history of any other TB lesions, indicating probable primary BTB. The susceptibility to BTB has been reported to be dramatically increased in young, married, pregnant, and lactating women.2,14,15 Two of the current patients (2/45) were lactating, and lactation has been reported to increase the susceptibility to TB infection by 7% to 30%,6,14,15 possibly as a result of ectasia of the breast ducts and the increased number of vessels.
Previous studies demonstrated that 30% to 75% of cases of BTB were accompanied by involvement of the ipsilateral axillary lymph node.15,16 In this study, only three patients (6.7%, 3/45) developed enlarged axillary lymph nodes, which were proven to be axillary lymphatic TB by biopsy. However, whether concomitant lymphatic TB is a primary source or a secondary involvement remains controversial. 15 The low incidence of BTB concomitant with axillary lymphatic TB in the current study (6.7%, 3/45) was likely due to the relatively low sensitivity of US for detecting axillary lymphatic lesions or to a lack of structural alterations in the involved lymph nodes, despite remaining invasion of tuberculosis bacteria.
BTB lesions can be classified into nodular, disseminated, and abscess types. 16 In the present study, we classified the BTB lesions into nodular, sinus, or abscess type, according to their US features, accounting for 55.5%, 28.9%, and 15.6% of lesions, respectively. No disseminated-type lesions were observed in this study. The pathological hallmarks of BTB are tuberculous granuloma, caseous necrosis, and liquefaction necrosis, and the BTB types classified in the present study were thought to be related to their pathological alterations. Lesions pathologically identified with tuberculous granuloma, caseous necrosis, and little/no liquefied necrosis were generally classified as nodular type by US, and lesions with a mass of liquefied necrosis were generally classified as abscess type. Lesions in which the necrosis in the BTB lesion broke through the skin to form a sinus tract connecting the breast mass to the localized breast skin were generally classified as sinus type by US. Six months of anti-TB therapy combined with suction or drainage of the abscesses is recommended for abscess type BTB, while antibiotic treatment is also recommended for sinus type BTB, and mastectomy is required if the lesion extends to a large, painful, or ulcerated mass. 17 Classification of BTB lesions based on their US features would therefore help to identify disease progression and inform the treatment regimen.
Sinus formation is a unique finding highly suspicious of BTB, with about 8% to 39% of BTB lesions associated with sinus formation.13,14,16,17 Of the current 45 BTB cases, 13 were classified as sinus type (28.9%, 13/45), accompanied by breast skin thickening and ulceration. The incidence of BTB with associated sinus formation is likely to be related to the disease course. In our study, 10 of the 13 patients with sinus type BTB (76.9%, 10/13) had a disease course longer than 6 months. A long-term disease course may result from low immunity, ultimately inducing the formation of a tuberculous abscess when liquefactive necrosis occurs. Tuberculous abscesses can gradually extend to the skin, causing skin ulceration and suppuration. Patients with plasma cell mastitis can also develop sinus formation. Lipid accumulation in the enlarged breast ducts in patients with plasma cell mastitis may trigger inflammation and further induce the formation of an abscess. About 20% of patients with plasma cell mastitis presented with sinus tracts.9,18,19 Both BTB and plasma cell mastitis can therefore present with internal hypoecho or heterogeneous echo in a ‘crater’ shape, making it difficult to differentiate between these two diseases using US, and a definite diagnosis requires US-guided fine-needle aspiration cytology or biopsy specimens.
Calcification is not common in BTB lesions. About 20% of BTB cases have been reported to develop calcifications, which is considered as a sign of a healed granuloma.18–22 However, BTB calcification has rarely been reported in US studies. 18 Calcification was detected in 8 of the 45 cases (17.8%, 8/45) in the current study, including six macrocalcifications and two microcalcifications. In addition, 74% of patients with breast ductal carcinoma and 55.8% with breast sclerosing adenosis developed calcifications, though these are usually associated with multiple punctate or clustered microcalcifications as detected by US.4,23 The present study showed a relatively low incidence of calcification (17.8%, 8/45), and most calcifications were >5 mm in diameter (75%, 6/8). One or two punctate microcalcifications were observed in two cases and no clustered calcifications were observed in any cases. Both these two cases had a disease course of <6 months and the diameter of the calcification increased after 3 months, and we therefore hypothesized that the microcalcification might have occurred in the early stage of BTB. Tuberculous granulomas will enlarge and calcium salts will be gradually deposited as the disease progresses, leading to the formation of macrocalcifications during the late stage of BTB. Further studies are needed to explore the correlation between the size of the calcification and the duration of the disease.
Previous imaging studies of BTB have mainly focused on gray images and few have used color images. In the current study, we used CDFI to detect and classify the blood supply conditions of the BTB lesions based on the Adler blood flow categorization. The blood flow was classified as category I in 36 cases, with a punctate color blood-flow signal in the margin and no blood-flow signal in the center. This was thought to be associated with the pathology of the BTB. Pathological alterations in the central BTB lesion are likely to involve caseous or liquefaction necrosis, resulting in avascularity at the center of the lesion. However, the margins of the lesion might retain residual normal tissue or form a tuberculous granuloma, thereby leading to vascularity of the marginal regions. The blood flow in eight cases (17.8%, 8/45) was classified as Adler category 0 and in one case (2.2%, 1/45) as Adler category II, possibly because of the large area of tuberculous granuloma with rich capillaries during sinus formation. Overall, the blood-flow signals in 44 cases (97.8%, 44/45) were classified as below category II, suggesting that hypovascularity might be a common US feature of BTB lesions.
The present study had several limitations. First, no information was obtained for cases of disseminated BTB, and further investigations of these are therefore needed. Second, we used CDFI to assess lesion blood flow rather than more advanced US techniques such as enhanced contrast US. Finally, we did not analyze other imaging data such as mammography or magnetic resonance imaging data because of the limited sample size.
In conclusion, BTB lesions can be classified as nodular, abscess, and sinus types based on their US features. BTB is characterized by hypovascularity and internal multi-macrocalcifications. US can provide good characterization of BTB, with great potential for contributing to its clinical diagnosis.