
Abstract
Purpose:
To analyze pre- and postoperative spinopelvic parameters and sagittal profiles in lumbar degenerative kyphoscoliosis (LDK) patients who underwent surgery using iliac screw (IS) and the incidence and risk factor of radiological adjacent segment degeneration (ASD).
Methods:
A total of 32 patients, who had undergone surgical correction and lumbar/thoracolumbar fusion with pedicle screws and IS instrumentation for LDK with a minimum 2-year follow-up, were included. Ten cases with ASD (group 1) and 22 cases without ASD (group 2) were compared to see pre- and postoperative change in sagittal view of spine and adjacent segment. Parameters of both groups were analyzed before and after surgery with each parameters being tested on correlativity. All deformity types of patients were classified using Scoliosis Research Society (SRS)-Schwab classification. Risk factors of ASD were evaluated using variables of SRS-Schwab classification.
Results:
Group 1, rather than group 2, showed significant increment in pelvic incidence (PI). Curve types, classified using SRS-Schwab classification, were all corrected using IS; and after correction, coronal curve type was N curve and PI minus lumbar lordosis (LL) and pelvic tilt showed tendency to decrease. Cases with preoperative sagittal vertical axis (SVA) more than 10 cm and with postoperative PI minus LL more than 20° were at higher risk of developing ASD.
Conclusion:
For those with high PI, it might be a risk to cause ASD. Maintaining normal thoracic and lumbar angle, correction of SVA less than 4 cm, and PI minus LL below 20° are proper ways to avoid ASD after surgery.
Introduction
Lumbar degenerative kyphoscoliosis (LDK) is characterized by the abnormal sagittal curvatures in which a kyphosis or a marked loss of lordosis is seen in the lumbar spine. 1,2 And LDK patients show a substantial decrease in the sacral inclination and marked weakness of the lumbar extensors. 2,3 The sacral slope (SS) and lumbar lordosis (LL) of patients with LDK are significantly lower than those of normal population. 4 –6 Because pelvic incidence (PI), the sum of SS and pelvic tilt (PT), is a fixed value, the mean PT is usually greater in LDK. Loss of the pelvic compensation resulting from the degeneration of pelvic and lumbar extensor muscles may result in the marked anterior PT. 7,8 LDK surgery usually needs long fusion. These long fusions are often associated with complications such as pseudarthrosis, sagittal deformity, and instrumentation failure. 9 –12 In several studies, sagittal imbalance has been shown to play a key role in the prognosis of LDK patients. 4,13 –16
ISs used in long instrumentation for deformity treatment are subject to large forces. Advantages of IS are relatively easy and rapid to insert, reduced intraoperative blood loss and operative time, equivalent to the Galveston rod technique for pelvic fixation, minimal rod bending, and a low-profile construct. However, there is no available critical consensus concerning incidence and risk factors of adjacent segment degeneration (ASD) as well as influence on sagittal profile and benefit of ISs in treatment of LDK.
The purpose of this study is to analyze differences between pre- and postoperative spinopelvic parameters and sagittal profiles in LDK patients who underwent surgery using IS and to evaluate the incidence and risk factor of radiological ASD after IS fixation.
Materials and methods
Patient population
This retrospective study was approved by the institutional review board. A total of 40 patients who had underwent surgical correction and lumbar/thoracolumbar fusions with pedicle screw and IS instrumentation for LDK from August 2005 to December 2010 were screened. To minimize a bias from a variety of surgical techniques, cases with any kind of osteotomy or interbody fusion, or with early postoperative complications involving proximal portion of fused levels, were excluded. Finally, a total of 32 patients who had undergone surgical correction and lumbar/thoracolumbar posterior/posterolateral fusion with pedicle and IS instrumentation for LDK with a minimum 2-year follow-up were included for the present investigation. ISs were linked to main rods by connectors. All surgeries were performed by one experienced spine surgeon. The average length of follow-up was 75.4 months (range = 28–102 months). Ten cases with ASD (group 1) and 22 cases without ASD (group 2) were compared to evaluate pre- and postoperative parameters in sagittal plane of spine and the adjacent segment. The proximal fusion level was selected by the general principle of idiopathic scoliosis surgery; upper instrumented vertebra (UIV) was the neutral vertebra. The levels of UIV were listed in Table 1. All deformity types of patients were classified using SRS-Schwab classification. Risk factors of ASD were evaluated using variables of SRS-Schwab classification.
The levels of UIV in each group.

UIV: upper instrumented vertebra; ASD: adjacent segment degeneration.
aMultivariate analysis was used.
Radiographic evaluation
Full-length radiographs of the whole spine extending from the base of the skull to the proximal femur in the anteroposterior and lateral planes were obtained before and after surgery. For the radiography of the spine, each patient was asked to stand erect comfortably. The arms were flexed, hands were placed on the contralateral clavicle, and knees were held in extension. The radiographs were digitized and analyzed by a team of researchers. As sagittal spinal parameter, we used kyphosis of thoracic spine (T4–T12), lordosis of lumbar spine (L1–S1), and T9 offset. As pelvic parameter, SS, PT, and PI angle were measured. As coronal parameter, Cobb’s angle was measured. Parameters of both groups were analyzed before and after surgery with each parameters being tested on correlativity. We defined radiologic ASD as more than 10° of kyphosis between the UIV and the vertebra two levels above the UIV (UIV + 2), proximal junctional disk collapse, adjacent vertebral compression fracture, and pullout of proximal pedicle screws (Figure 1).

(a) Lateral standing radiograph of a 73-year-old woman with severe sagittal misalignment and osteoporosis. (b) After D10 to sacrum posterior instrumented fusion, LL and SS are increased, TK and PT are decreased, and global sagittal misalignment is corrected. (c) At 4 years postoperatively, proximal junctional failure was developed. LL: lumbar lordosis; SS: sacral slope; TK: thoracic kyphosis; PT: pelvic tilt.
Statistical analysis
All statistical analyses of data from both groups were conducted by the SPSS system (version 18.0). Mann–Whitney U-test was used to assess the difference in spinopelvic parameters between ASD and non-ASD. Simple linear regression analysis was used to examine the relationship among spinopelvic parameters. χ 2 analysis was used to examine risk factors of ASD using variables of SRS-Schwab classification. Multivariate analysis was used to evaluate correlation of UIV with the development of ASD. p Value of less than 0.05 was considered as significant.
Results
Participants were average 68.8 (53–81) years old at index operation. There was no statistical difference about age. Among ASD, there were six cases of proximal junctional kyphosis (60%) and four cases of vertebral fracture (40%). Table 2 shows the radiographic results of spinal and pelvic parameters between ASD group and the non-ASD group. Group 1, rather than group 2, showed significant increment in PI (preoperative: 62.69 ± 9.39° vs. 53.66 ± 8.66° and postoperative: 62.81 ± 9.39° vs. 53.06 ± 12.14°; p = 0.017, 0.017). Table 3 shows the comparison of the spinopelvic parameters between the preoperative and postoperative values in ASD patients and the non-ASD group patients. Preoperative PT and sacral slope (SS) did not show statistically significant difference in both groups; however, postoperative SS and thoracic kyphosis (TK) showed more statistical significant difference in group 2. LL also showed tendency to increase in group 2. Decrement of PT and increment of SS in both groups were observed, and postoperative PT showed significant correlation with PI (R = 0.813, 0.822; Tables 4 and 5). Curve types, classified using SRS-Schwab classification, were all corrected using IS; and after correction, coronal curve type was N curve and PI minus LL and PT showed tendency to decrease. Cases with preoperative sagittal vertical axis (SVA) more than 9.5 cm and with postoperative PI minus LL more than 20° were at higher risk of developing ASD (Tables 6 and 7). Multivariate analysis showed no significant correlation between the level of UIV and the development of ASD (p = 0.556).
Comparison of the spinopelvic parameters between the ASD and the non-ASD group.

ASD: adjacent segment degeneration; PI: pelvic incidence; PT: pelvic tilt; SS: sacral slope; LL: lumbar lordosis; TK: thoracic kyphosis; p Value: < 0.05, indicating the statistical significance.
Comparison of the spinopelvic parameters between the preop. and the postop.

PI: pelvic incidence; PT: pelvic tilt; SS: sacral slope; LL: lumbar lordosis; TK: thoracic kyphosis.
Correlation coefficients among the spinopelvic parameters in the ASD group.
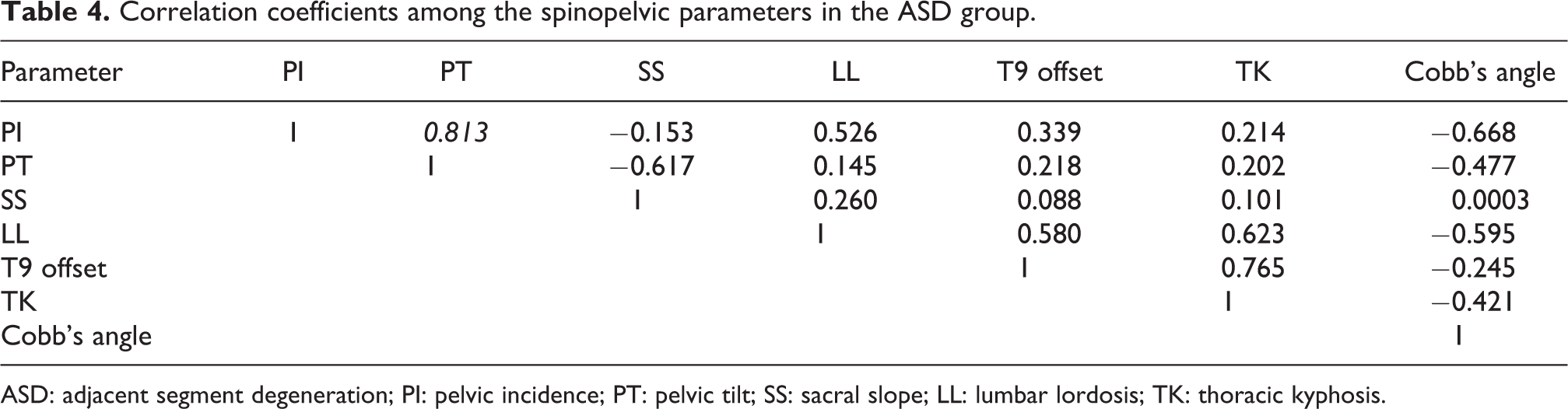
ASD: adjacent segment degeneration; PI: pelvic incidence; PT: pelvic tilt; SS: sacral slope; LL: lumbar lordosis; TK: thoracic kyphosis.
Correlation coefficients among the spinopelvic parameters in the non-ASD group.
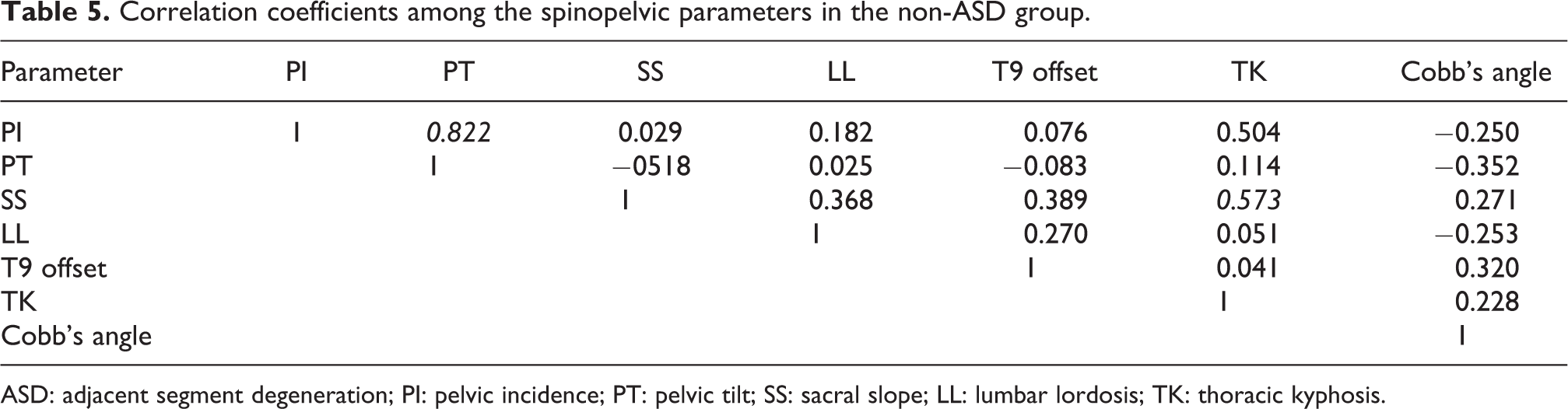
ASD: adjacent segment degeneration; PI: pelvic incidence; PT: pelvic tilt; SS: sacral slope; LL: lumbar lordosis; TK: thoracic kyphosis.
Risk factor through preoperative SRS-Schwab classification.

ASD: adjacent segment degeneration; PI: pelvic incidence; LL: lumbar lordosis; SVA: sagittal vertical axis; PT: pelvic tilt.
Risk factor through postoperative SRS-Schwab classification.
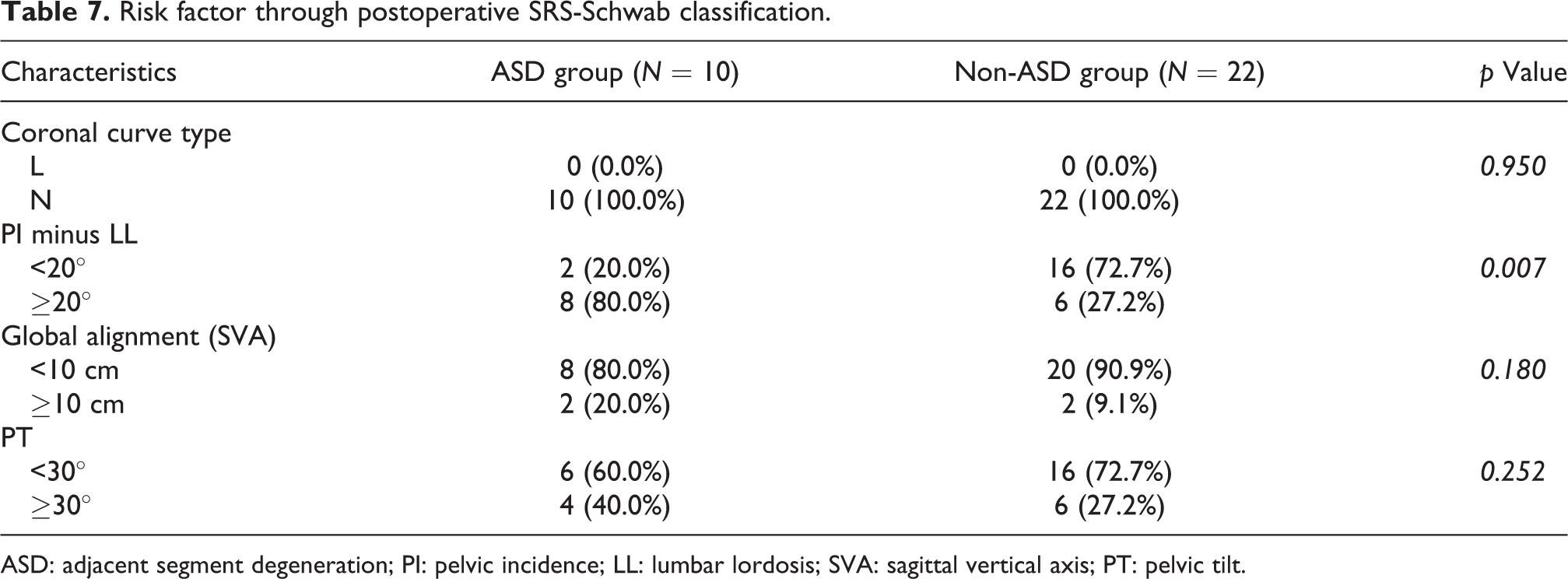
ASD: adjacent segment degeneration; PI: pelvic incidence; LL: lumbar lordosis; SVA: sagittal vertical axis; PT: pelvic tilt.
Discussion
The risk factors of ASD are known to include old age, female sex, high body mass index (BMI), osteoporosis, rigid fusion such as posterior lumbar interbody fusion (PLIF) and pedicular screw system, fusion length, and preexisting adjacent level degeneration. 17 –22 Besides the above factors, restoration of spinopelvic balance has gained increasing attention recently. 4,13 –16 Glassman et al. 23 reported positive sagittal balance to be the most reliable predictor of clinical symptoms and emphasized on restoration of sagittal balance. When planning realignment surgery for adult spinal deformity, Schwab et al. emphasized that restoring low SVA and PT values is a critical goal and should be combined with proportional LL to PI (SVA less than 4 cm, PT less than 20°, and LL = PI ± 10°). 24 Because new SRS-Schwab classification system is clear and has excellent intra- and inter-rater reliability, we regarded curve type and three sagittal modifiers of SRS-Schwab classification as possible risk factors of ASD. 24
Although there was no controlled group, as shown in this study, IS usage seemed to be effective in reducing PT and increasing SS in LDK. For those with high PI, it might be a risk to cause ASD, and SS increment has correlation with TK in non-ASD group (Table 4). It is well established that PI is attributed to the pelvic shape and is strongly linked to SS and PT in normal and scoliotic spines as reported by Duval-Beaupere et al. 25 and Legaye et al. 26 PI in the ASD group was significantly greater than in the non-ASD group in our study. Cho et al. reported that the preoperative sagittal imbalance and high PI proved the most significant risk factors of sagittal decompensation after long instrumentation. 27 And Park et al. reported that the development of ASD was closely related to postoperative PI and PT in the patients with spondylolytic spondylolisthesis. 28 In patients with LDK, the mean SS and LL were significantly lower than those of normal individual. 4 –6 Because PI is the algebraic sum of SS and PT, the mean PT was significantly greater in LDK. High PI usually indicates steep SS and then larger LL in normal individual. However, in patients with LDK, high PI meant high PT and relatively marked loss of the SS. This is probably due to weakness of the lumbar extensors seen in LDK patients. In the present study using ISs, there was a tendency to reduce PT and increase SS postoperatively. Especially in non-ASD group, SS increment had a correlation with TK and increased SS induced normal TK. Curve types, classified using SRS-Schwab classification, were all corrected to N curve postoperatively, and PI minus LL and PT showed a tendency to decrease.
The patients who developed ASD in our series presented a postoperative high PI–LL mismatch and preoperative SVA more than 10 cm, which reflected the fact that they had required larger amount of correction of LL than performed. Mendoza-Lattes et al. 29 reported that the most important factor was achieving LL exceeding TK in a reconstructive surgery. Schwab et al. also suggested a simplistic formula of achieving LL within 10° of PI. 24,30
However, this study was a retrospective case control study (level III evidence) with an average follow-up of about 6 years. Our study had certain limitations such as the number of patients was limited and study design was not a randomized controlled and was not a fused level-matched cohort analysis. Lack of the controlled group without ISs makes this study not to show the effect of ISs on sagittal profiles after LDK surgeries.
In conclusion, the presence of high PI and cases with preoperative SVA more than 10 cm and postoperative insufficient LL restoration seemed to be the most significant risk factors for ASD after surgical correction of LDK using ISs and should be primarily considered before surgical correction. The authors reported that gaining normal thoracic and lumbar angle through the increase in SS by IS fixation and correction of SVA less than 4 cm and PI minus LL below 20° were important to avoid ASD after IS fixations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.