
Abstract
The authors present a case of 45-year-old man with neurofibromatosis type 1 (NF-1) and thoracic scoliosis, previously undergoing fusion surgery, who developed myelopathy. This patient further complained of lightning pain when he extended and horizontally abducted the convex-side shoulder. Radiological examination revealed the progression of dystrophic scoliosis with opened spinal canals and the presence of a neurofibroma behind the spinal cord at the apical levels. Delayed development of spinal instability can occur due to dystrophy even postoperatively in patients with NF-1. After tumor resection, he had rapid recovery from myelopathy and no recurrence of radiating pain despite shoulder movement. These findings provide a speculation that high, intense amplitude movement of the shoulder toward the spinal canal causes the impingement on the neurofibroma, resulting in indirect compression of the exposed spinal cord. This is the first report describing thoracic compression myelopathy associated with paraspinal displacement of the scapula.
Keywords
Introduction
Neurofibromatosis type 1 (NF-1) is a multisystemic, autosomal dominant hereditary disorder that often causes severe spinal deformities. 1,2 Scoliosis is particularly common in patients with NF-1, 3,4 with a reported prevalence of 2–69%. 5 This scoliosis is categorized into two types—dystrophic and non-dystrophic. 6,7 Dystrophic scoliosis is manifested by vertebral scalloping, rib penciling, and dural ectasia, 6,7 resulting in more frequent development of neurological paralysis. 8,9
Severe progression of spinal curvature, malignant transformation or intratumoral hemorrhage of paraspinal neurofibromas, and displacement of the ribs into the spinal canal are causes of thoracic compression myelopathy in dystrophic scoliosis patients with NF-1. 1 However, to the best of our knowledge, no reports have described neurological paralysis caused by displacement of the scapula toward the spinal canal. Herein, we report an NF-1 and dystrophic scoliosis patient case with thoracic compression myelopathy associated with dynamic movement of the shoulder.
Case report
This study was approved by the institutional review board at Kobe University Graduate School of Medicine. Written informed consent was obtained from the patient in concordance with the principles of the Declaration of Helsinki and with the laws and regulations of Japan.
A man with multiple café au lait spots and cutaneous neurofibromas, diagnosed with NF-1 in childhood, developed severe scoliosis with a right major curve. He refused in juvenile but finally underwent scoliosis surgery at 35 years of age. However, successful completion of corrective osteotomy and spinal instrumentation was difficult because of a quite large volume of intraoperative bleeding from paraspinal tumors, and only posterior short-segment surgery including decortication of the facet joints and laminae and autogenous iliac bone grafting was performed in the thoracic spine. Bed rest with a body cast was suggested for 3 months after surgery to aim spinal fusion.
At 45 years of age, the patient presented with progressive gait and urinary disturbance and revisited our institute. Two months after the development of symptoms, at hospitalization, he was unable to walk without support. He also felt lightning pain radiating from the back to the lower limbs lasting a year. Lightning pain was recognized when he moved the right scapula to the spine, at the extended and horizontally abducted position of the shoulder.
Neurological examination revealed severe spasticity with bilateral hyperreflexia of deep tendon reflexes in the lower extremities, positive pathologic leg reflexes including the Babinski reflex, and positive Romberg sign. Manual muscle testing demonstrated weakness down to the level 4 of 5 in both lower limbs. Sensory disturbance was observed below the Th6 dermatomal level.
Radiographs of the thoracic spine 3 months after the initial surgery showed the 83° right scoliosis by the Cobb angle from Th2 to Th8 (Figure 1(a)) and the 64° kyphosis at the same levels (Figure 1(b)). Radiographs at rehospitalization of 10 years later demonstrated the worsened spinal curve with 91° in an anteroposterior view (Figure 1(c)) and 72° in a lateral view by the Cobb angle between Th2 and Th8 (Figure 1(d)). Computed tomography (CT) images exhibited postoperative or spontaneous vertebral body fusion between Th3 and Th6 with the 79° right curvature in the coronal plane and with the 57° posterior curvature in the midsagittal plane (Figure 2(a) and (b)), postoperative left facet and lamina fusion between Th3 and Th8 with the 70° posterior curvature in the left-sagittal plane (Figure 2(c)), dystrophic disappearance of the posterior components of the right thoracic spine in the three-dimensional reconstruction (Figure 2(d)), and no obvious fractures around the apical vertebrae. Magnetic resonance images displayed a large, high to intermediate intensity lesion behind the spinal cord at Th5–Th8 levels on T2-weighted images, suggesting a tumor mass (Figure 3(a) and (b)). To determine the mechanism of lightning pain, we performed conventional and CT myelographic evaluation. Myelography revealed the flowed contrast agent was blocked at Th7–Th8 level when an examining table was tilted head down (Figure 4(a) to (c)). Then, CT myelographic examination at multiple positions of the right shoulder revealed an inward shift of the scapula toward the thoracic spinal canal, which was severe enough to impinge on the spinal cord through the paraspinal tumor, at the extended and horizontal abducted position (Figure 4(d) to (f)). Magnetic resonance examination at the indicated position of the convex-side shoulder was difficult due to the recurrence of severe radiating pain.

Radiographs of the thoracic spine. The R indicates the right side of the body. (a) A posteroanterior radiograph showing the right-curved scoliosis of 83° by the Cobb angle between Th2 and Th8 3 months after the initial surgery. (b) A lateral radiograph showing the kyphosis of 64° by the Cobb angle between Th2 and Th8 3 months after the initial surgery. (c) A posteroanterior radiograph showing the right-curved scoliosis of 91° by the Cobb angle between Th2 and Th8 10 years after the initial surgery. (d) A lateral radiograph showing the kyphosis of 72° by the Cobb angle between Th2 and Th8 10 years after the initial surgery.

CT images of the thoracic spine. The R indicates the right side of the body. (a) A coronal CT image showing vertebral body fusion between Th3 and Th6 with the 79° right curvature and no obvious fractures around the apical vertebrae. (b) A midsagittal CT image showing vertebral body fusion between Th3 and Th6 with the 57° posterior curvature. (c) A left-sagittal CT image showing facet and lamina fusion between Th3 and Th8 with the 70° posterior curvature. (d) A three-dimensional CT image showing bone fusion of the left posterior spinal components (white arrow), dystrophic disappearance of the right posterior spinal components (gray arrow), and the right scapula located close to the spinal canal (black arrow). CT: computed tomography.

Magnetic resonance T2-weighted images of the thoracic spine. The R indicates the right side of the body. (a) A sagittal image showing a high to intermediate intensity lesion along behind the spinal cord at Th5–Th8 levels (arrow), suggesting a tumor mass. (b) An axial image showing a paraspinal tumor (arrow) and the left-shifted spinal cord.

Conventional and CT myelographic images of the thoracic spine and physical images of the right shoulder. The R indicates the right side of the body. (a) A posteroanterior radiograph during myelography showing incomplete blockade of the flow of the contrast agent at Th7–Th8 level (arrow). (b) A lateral radiograph during myelography showing incomplete blockade of the flow of the contrast agent at Th7–Th8 level (arrow). (c) A sagittal CT myelographic image showing incomplete blockade of the flow of the contrast agent at Th7–Th8 level (arrow). (d) An axial CT myelographic image showing narrowed dural tube (white arrow), dystrophic spinal canal (gray arrow), and the right scapula at a neutral position of the right shoulder (black arrow). (e) An axial CT myelographic image showing narrowed dural tube (white arrow), dystrophic spinal canal (gray arrow), and the right scapula at an extended and horizontally abducted position of the right shoulder (black arrow), revealing paraspinal displacement of the scapula on the convex side. (f) Photographs of the back with characteristic multiple, large cutaneous and subcutaneous neurofibromas at the lightning pain-generating position of the right shoulder; extension (a′) and then horizontal abduction (b′). At this position of the shoulder, the scapula could be displaced toward the thoracic spinal canal (c′). CT: computed tomography.
Based on neurological and radiological findings, the preoperative diagnosis was thoracic compression myelopathy resulting from the progression of scoliosis and opened spinal canals due to dystrophy, the presence of a paraspinal tumor indicating neurofibroma, and high and excessive amplitude movement of the shoulder on the convex side. We tried but thought that revision surgery of scoliosis such as correction and instrumentation is too risky because of adhesion from the initial surgery, exposed spinal cord, and an increased number of subcutaneous and paraspinal neurofibromas introducing additional bleeding. To rescue from myelopathy with reduced invasion, we performed en bloc resection of the paraspinal tumor only. There was completed bone fusion only on the concave side of the apical thoracic vertebrae and more proximal and distal segments were moved, affirming the progression of scoliosis. Although the spinal cord was exposed because of dystrophic disappearance of the laminas and pedicles on the convex side of the apical vertebrae, no apparent adhesion between the paraspinal tumor and surrounding tissues was observed. Further, the spinal cord was not compressed directly by the tumor mass. However, marked impingement of the tumor and then the spinal cord by the scapula was found under extension and horizontal abduction movement of the shoulder. Consequently, the tumor was removed easily (Figure 5(a) and (b)). Finally, no direct spinal cord compression by the scapula at every position after removal of the tumor was confirmed.
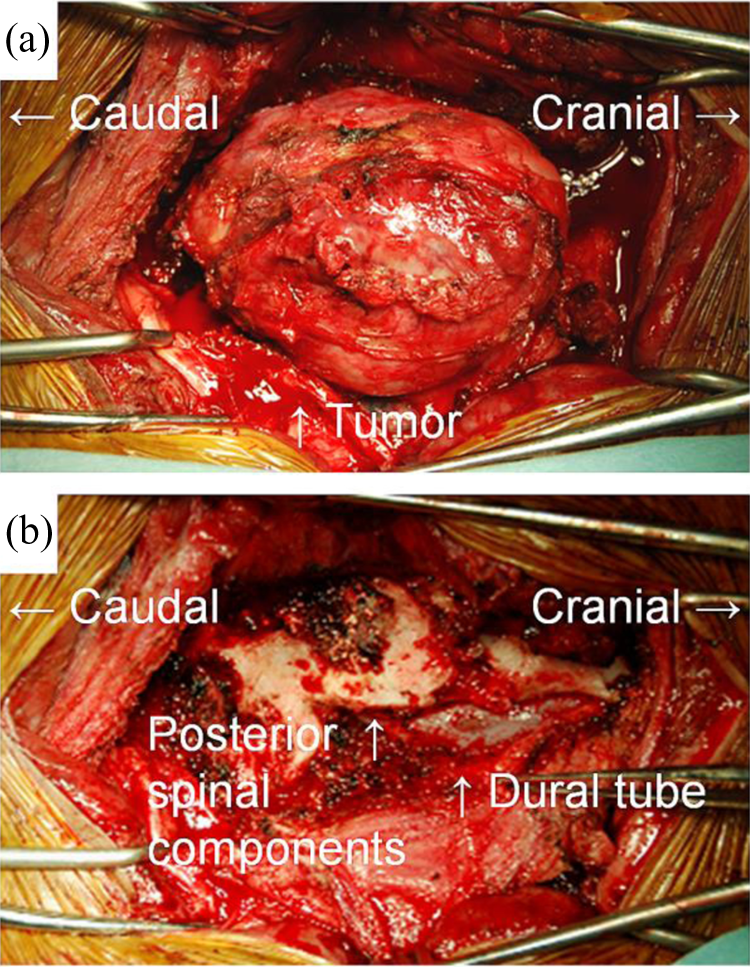
Intraoperative findings of tumor resection. (a) A photograph before tumor removal showing the presence of a paraspinal tumor 12 × 7 × 3 cm in size along behind the thoracic spine. (b) A photograph after tumor removal showing the disappearance of the laminas and pedicles on the convex side of the apical vertebrae. The spinal cord was not adhered with or compressed directly by the tumor.
The postoperative pathohistological diagnosis of the tumor was neurofibroma. No malignant transformation or intratumoral hemorrhage was detected. The patient had rapid recovery from myelopathy. Three months after surgery, he was able to walk without support and reported no difficulties in his daily living. There was no recurrence of myelopathy or lightning pain through postoperative 2 years.
Discussion
To date, several reports have presented a total of 21 NF-1 patient cases of intraspinal rib head displacement. 1,10 –20 However, there are no reports of intraspinal or paraspinal displacement of the scapula. In this case report, the male patient with NF-1 and scoliosis took fusion surgery of the thoracic spine at 35 years of age, but subsequently, at 45 years, developed myelopathy with lightning pain when the shoulder on the convex side was extended and horizontally abducted. Radiological examination revealed the progression of thoracic dystrophic scoliosis with opened spinal canals and the presence of a large tumor located behind the spinal cord at the apical levels. No contact or adhesion between the spinal cord and the paraspinal tumor, which was a nonmalignant neurofibroma without any intratumoral bleeding, was found through surgery. After tumor resection, he had rapid recovery from myelopathy and no recurrence of radiating pain despite shoulder movement. These findings provide a speculation that high, intense amplitude movement of the convex-side shoulder toward the spinal canal causes the impingement on the paraspinal neurofibroma, resulting in indirect compression of the exposed spinal cord. The current report does not exhibit conclusive evidence of shoulder movement-induced myelopathy; however, this case suggests the idea that the protrusion of the scapula as well as of the ribs into the spinal canal can occur in patients with severe thoracic dystrophic scoliosis, even without paraspinal tumors. Further, complaints of lightning pain during the extension and horizontal abduction of the shoulder on the convex side of the spinal curvature may be an indication of scapula-associated spinal cord compression. To the best of our knowledge, this is the first report presenting an NF-1 case with myelopathy due to the progression of dystrophic scoliosis, the presence of a paraspinal neurofibroma, and high and excessive amplitude movement of the shoulder.
Postoperative progression of scoliosis and time-dependent enhancement of spinal dystrophy by paraspinal tumors should be noted. It is well known that the quality of bone in NF-1 dystrophic scoliosis is generally low, leading to a high incidence of pseudoarthrosis after fusion surgery. 6,8,21 It is also reported that spinal deformity can progress despite the achievement of arthrodesis in patients with hyperkyphosis and short-segmented curves. 22 In this patient case, massive bleeding from paraspinal tumors, which is also a common intraoperative complication of NF-1 scoliosis, 6,8 made it difficult to conduct corrective osteotomy and spinal instrumentation during the initial surgery. Only decortication and autogenous bone grafting resulted in in-situ nonrigid spinal fusion only between short segments, which allowed the progression of the scoliosis curve and facilitated paraspinal displacement of the scapula. In idiopathic scoliosis patients, curves more than 30° is known to progress even after skeletal maturity, which is the most likely in patients with single thoracic curves between 50° and 75°. 23 Retrospectively, additional anterior fusion surgery might need to be conducted as combined anterior/posterior fusion was recommended. 8,9 However, even if rigid spinal fusion was obtained at the initial surgery, spontaneous disappearance of the posterior spinal components due to dystrophy from paraspinal neurofibromas may not be avoidable. The current patient case sheds light on the importance of acquisition of rigid spinal fusion at surgery and careful clinical and radiological follow-up in patients with NF-1 and dystrophic scoliosis.
Conclusion
We presented a case of NF-1 with thoracic compression myelopathy due to the progression of dystrophic scoliosis with opened spinal canals, the presence of a neurofibroma behind the spinal cord at the apical levels, and high and excessive amplitude movement of the convex-side shoulder toward the spinal canal. This is the first study suggesting scapula-associated neurological dysfunction. Spine clinicians, surgeons, and radiologists should recognize that delayed development of spinal instability, leading to myelopathy, can occur due to dystrophy even after fusion surgery in patients with NF-1 and scoliosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.