
Abstract
Purpose:
To evaluate the midterm results of arthroscopic reconstruction of acute acromioclavicular (AC) joint disruption using TightRope™ system.
Methods and Material:
We retrospectively assess the results of 24 patients of acute AC joint dislocation who were operated using TightRope system. Constant and University of California, Los Angeles (UCLA) scores and coracoclavicular distance were calculated pre- and postoperatively. Data was entered into MS excel and analyzed using the SPSS version 17.
Results:
The mean follow-up was 39.45 months. Constant and UCLA scores were significantly increased postoperatively. Six patients had partial loss of reduction within 3–6 months and two patients had a failure of construct. Constant score was significantly lower in these patients.
Conclusion:
TightRope reconstruction of the AC joint is a reproducible and safe alternative to many other techniques of AC joint reconstruction. Early subluxation remains a concern and may reflect the need for technique modification.
Introduction
Acromioclavicular (AC) joint disruption is not an uncommon injury among sports person involved in contact sports. It accounts for 3–5% of all shoulder injuries. 1 Rockwood classification is most commonly used to classify these injuries. Types IV through VI are managed by surgical reconstruction and treatment of type III should be individualized based on the patient’s demand, activity level, and response to conservative treatment. Availability of a multiple techniques for reconstruction of the dislocated AC joint in the literature 2 –11 reflects that there is no gold standard or universally accepted treatment for AC joint reconstruction. Recently, TightRope has gained popularity in surgical reconstruction of acute AC joint dislocation 12 –15
We have been using the TightRope device (Arthrex, Naples, FL, USA) for arthroscopic fixation of acute AC joint disruption (<4 weeks) for the last 7 years in our hospital. The purpose of this study was to evaluate the outcome of TightRope fixation of acute (<4 weeks) AC joint dislocation.
Methods and materials
We retrospectively reviewed the medical records of 34 patients of AC joint dislocation who were treated in our hospital between January 2010 and July 2013. Only acute cases (<4 weeks old) who had a minimum 2-year follow-up with availability of all records were included in the study.
Seven patients were lost to follow-up between 3 and 6 months and three patients did not fulfill the criteria. This made the study cohort of 24 patients (Table 1). All patients were operated by the same technique described below.
Patient data.

UCLA: Constant and University of California, Los Angeles; M: male; F: female.
Consent to publish
Informed consent was obtained from all individual participants included in the study regarding publication. All procedures in this study were approved by an ethical review board of the hospital before conducting the study.
Surgical technique
The patient is positioned in lateral decubitus position after the anesthesia. The arthroscope is inserted through the standard posterior portal. An anteroinferior portal (just lateral and below the tip of coracoid) is established by outside-in technique to reach the tip of the coracoid. After diagnostic shoulder arthroscopy to see any associated glenohumeral pathology, rotator interval is debrided. Using arthroscopic shaver and radiofrequency ablation, lateral surface of the coracoid is exposed. At this stage, 30-degree arthroscope is exchanged with 70-degree arthroscope to see the base of the coracoid. The base of the coracoid is then progressively exposed using radiofrequency ablation and arthroscopic shaver. Once the inferior surface of the coracoid is exposed, a 1 cm transverse incision is made over the clavicle at the level of the coracoid. Deltotrapezial fascia is incised and anterior and posterior boundaries of the clavicle are exposed subperiosteally.
The AC joint TightRope variable drill guide with coracoid drill stop attachment (Arthrex) is inserted through the anteroinferior portal. If AC joint TightRope variable drill guide is not available, then use of posterior cruciate ligament reconstruction tibial jig may also facilitate proper placement of the jig on the inferior surface of the coracoid. The guide tip is positioned under the base of the coracoid under arthroscopic vision. The top of the guide is positioned over the clavicle in the line of the coracoid. A guide pin of 2.4 mm (Arthrex) is inserted into clavicle and then into the coracoid under arthroscopic vision. Guide pin is stopped from further advancing beyond the inferior cortex of coracoid by a drill stop. Reaming is then done over the guide pin with 4 mm cannulated drill. After removing the guide pin (not the cannulated drill), a Nitinol suture passing wire (Arthrex) is passed down through the drill keeping the suture loop superiorly and taken out through the anteroinferior portal using an arthroscopic grasper. The drill is removed and traction sutures of TightRope are pulled down through the tunnel using a Nitinol wire loop. The oblong button is then flipped to enable the button to pass through the tunnel. Sometimes the oblong button may partially flip in the tunnel while passing the TightRope, a knot pusher is very useful in this situation to facilitate passage of TightRope. The Nitinol suture passing wire is then drawn out of the anteroinferior portal under direct vision. When button is seen under the coracoid, the trailing suture is used to flip it, under the bone. The position of oblong button is confirmed arthroscopically and then clavicle is reduced. Reduction is confirmed in image intensifier and then fiber loop wire is tied over the clavicular circular button. The wound is closed in layers and portals are closed.
Patients were given sling for initial 6 weeks. Passive mobilization and pendulum exercises were started as soon as the pain relieved. Active abduction and flexion were started after 2 weeks up to 30 degrees and gradually increased to 90 degrees by 6 weeks. Full active motion was allowed for 10 weeks. Patients were put on strengthening exercises after 3 months.
Patients were evaluated clinically using Constant and University of California, Los Angeles (UCLA) evaluation methods pre and postoperatively. Radiological evaluation included anteroposterior, axillary lateral, and Zanca view (AP view with 15-degree cephalic tilt). Coracoclavicular (CC) distance was calculated pre- and postoperatively on X-rays with the same magnification as the perpendicular distance between uppermost point of superior cortex of the coracoid and the undersurface of clavicle and compared with normal side.
Statistics
Data was entered into MS excel and analyzed using the SPSS version 17. Descriptive statistics in the form of mean and standard deviations (s.d.) were used to characterize the study sample. For quantitative data, the difference between the means of the two independent groups was compared by t-test (for a normal distribution). A p value of less than 0.05 was considered statistically significant.
Results
Out of the total 24 patients, there were 21 males (87.5%) and 3 females (12.5%). The mean age of the study population was 28.7 years (s.d. = 3.4). According to Rockwood classification, 33.3% (n = 8) were type III and remaining were type V (n = 16; 66.7%). Occupation wise 16 participants (66.7%) were involved in sports. The mean years of follow-up of the study group were 39.45 months (s.d. = 6.72). There was no gender wise difference seen between the two variables (p > 0.05).
The constant scores and UCLA scores of the study group significantly increased in postoperative period. There was a highly significant difference in CC distance in pre- and postoperative period too (Tables 2 and 3) The mean CC distance of normal side was 9.60 mm as compared to dislocated side which was 21 mm. The mean CC distance postoperatively was 11.43 mm. The mean CC distance in case of postoperative subluxation was 15.93 mm.
Comparison of surgical parameters of the study population in pre- and postoperative period at final follow-up.
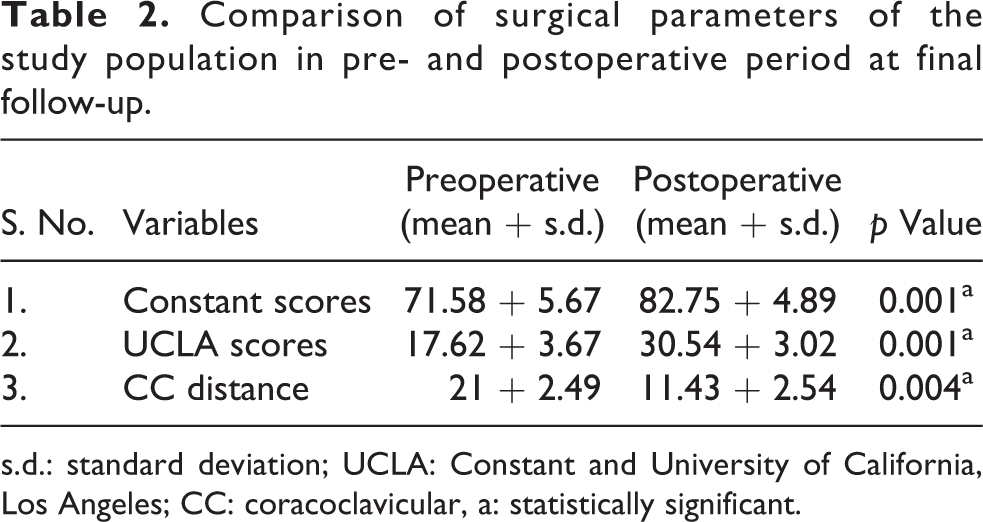
s.d.: standard deviation; UCLA: Constant and University of California, Los Angeles; CC: coracoclavicular, a: statistically significant.
Comparison of postsurgical scores with the outcomes among the study participants at final follow-up.
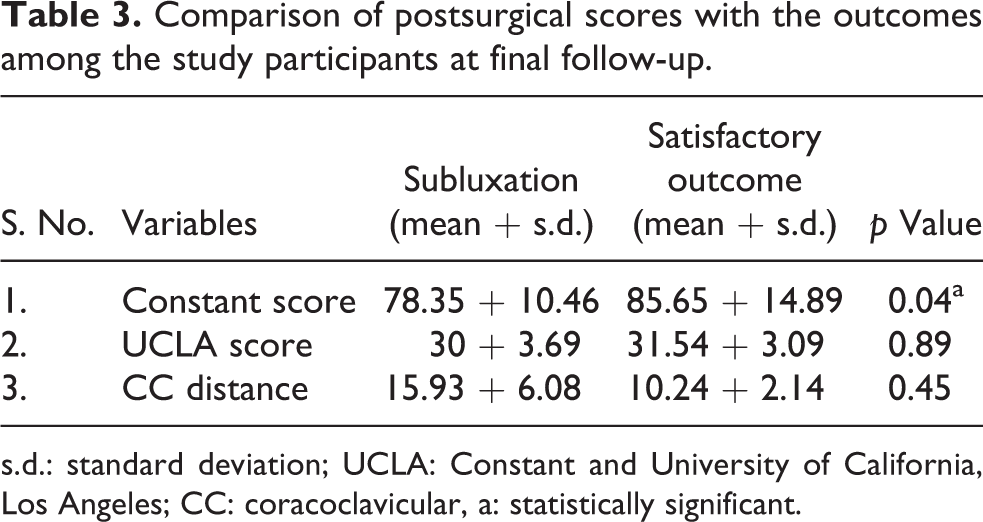
s.d.: standard deviation; UCLA: Constant and University of California, Los Angeles; CC: coracoclavicular, a: statistically significant.
Partial loss of reduction (Figure 1) occurred in six patients between 10 and 24 weeks. Constant score was significantly less in patients in whom subluxation occurred at the final follow-up (Table 3). Two patients came back with recurrence of pain and deformity at 12 and 30 weeks, respectively. X rays (Figure 2) of both of these patients showed construct failure. The mean time to return to work (excluding one gymnast in whom construct failed at 30 weeks) was 8 months (s.d. = 5.78). One gymnast in whom construct failed at 30 weeks refused resurgery and changed his profession. Satisfactory reduction was maintained till the last follow-up in the rest of the patients (Figure 3a and b). Intraoperatively clavicular fracture occurred in one patient (Figure 4). This patient lost to follow up after 2 months, so not included in the study. Two patients had concomitant anteroinferior labral injuries and one patient had superior labral anterior and posterior (SLAP) tear type II tears which were repaired simultaneously. Improvement in outcome measures was independent of the type of injury (p > 0.05). Over correction was not seen in any case.

Zanca view of the shoulder joint showing osteolysis around clavicular button and partial loss of reduction due to sinking of a button into the clavicle.

Eccentric drilling may fail the construct early by suture cut out. See in the picture that inferior cortex is not drilled.

(a) Pre- and (b) postoperative X rays of type V AC joint dislocation showing good correction of dislocated AC joint.

Clavicular fracture can occur due to excessive pressure during reduction maneuver intraoperatively.
Discussion
Many surgical techniques with successful results have been published, including both open 3 –8 and arthroscopic procedures. 10,12 –15 Arthroscopic techniques have the advantage of less morbidity fast recovery and no need of the second procedure for removal of hardware. TightRope-based reconstruction of the AC joint is an arthroscopic nonanatomical CC ligament reconstruction, which is no longer a new procedure for reconstruction of the dislocated AC joint. TightRope fixation has been described as an alternative to other open and arthroscopic anatomical procedures with successful results by many authors. 12 –17 Many biomechanical studies 18,19 have shown that TightRope system provides excellent superoinferior stability with load to failure higher than native ligament. However, anteroposterior stability remains a concern with this procedure. We witnessed six (25%) cases of partial loss of reduction in this series. All of these patients had the inferior constant score at the final follow-up compared to the rest of the patients. However, this is in contrast to previously published studies 11,13 which showed that radiological failure did not influence outcome.
This 25% rate of partial loss of reduction reflects the need for biomechanical modification of the procedure. Many surgical techniques have been published in the literatures which have some restraint in addition to CC ligament reconstruction (AC ligament reconstruction, use of two TightRope for both conoid and trapezoid ligament reconstruction and ligament augmentation) for better stability in anteroposterior direction. 10,11,16 But the long-term results of these techniques in a large cohort are still not available.
TightRope fixation of acute AC joint dislocation relies on the principle that if AC joint is kept reducing it will allow healing of torn AC ligaments. 20 Healing ligaments may not gain strength equal to native ligament even at 1 year. 21 It means any disruption before the healing of torn ligaments will fail the construct either partially or fully. We have seen two modes of failure: partial loss of reduction and complete failure of construct. Early failure occurs when a fiber loop cuts through the cortex of clavicle. We witnessed eccentric drilling through the anterior cortex instead of inferior cortex as one important cause of it (Figure 2). Osteolysis around clavicular button and its sinking in clavicle is the most common cause for partial loss of reduction (Figure 1). TightRope gives only vertical stability and it may not prevent horizontal motion at the AC joint. Such early motion while doing physiotherapy may lead to motion around the clavicular button and resultant osteolysis. Superior surface of lateral clavicle where the clavicular button rests is not as flat as the button itself. This lack of conformity may give rise to potential motion between clavicle and button leading to osteolysis.
Fiber loop breakage is a cause of early failure of the construct. Strength of fiber loop no. 5 is fairly reliable with maximum load to failure above 620 N. 22 Only likely reason of suture breakage for this strong suture is that it might have eroded while pulling down through the tunnel. A smooth passage without struggle should be ensured to avoid suture abrasion. Instead of pulling forcefully while passing the TightRope, a knot pusher should be used to pass it.
Recently, with the increasing trend of arthroscopic CC fixation using transcoracoid technique, many authors have reported coracoid fracture as a potential complication. 23 We did not have any such complication. This may be due to proper visualization of the inferior surface of coracoid and drilling with 4 mm drill at the base of the coracoid (widest part) where it projects from the scapula. In a recently published cadaveric study, Rylander et al. 24 demonstrated that a 4-mm tunnel is significantly stronger than a 6-mm tunnel. We used single tunnel in all cases as creating two tunnels in relatively small coracoid can increase the risk of fracture and tunnel convergence. Also, a study by Beitzel et al. 17 showed that there was no significant difference between single and double clavicular tunnel techniques with regards to stability imparted to AC joint.
Conclusion
Following conclusions were drawn from the study: AC joint disruption is predominantly seen in male patients. TightRope fixation of AC joint disruption is a safe alternative to other techniques with reproducible and comparable results. In this study, partial loss of reduction occurred early (within 6 months) and no loss of reduction was seen after that. This probably reflects that healing of torn ligaments also imparts stability in addition to TightRope. This also indicates that additional fixation along with TightRope may prevent early loss of reduction. Radiological failure/subluxation was associated with inferior outcome. We observed 25% subluxation rate that indicates the need for technique modification to prevent it. In cases where no early loss of reduction occurred, TightRope system was capable of providing long-term stability.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.