
Abstract
Background:
Arthroscopically assisted techniques for acromioclavicular joint reconstruction have increasingly been used over the past 15 years. Long-term results are lacking.
Hypothesis:
Patients will continue to show good clinical function and sustained anatomic reduction at long-term follow-up.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Twenty patients (67%) with a known endpoint were followed up at a mean of 15 years (range, 14-16 years) postoperatively. Twelve patients (60%) had Rockwood type 5, 6 (30%) type 4, and 2 (10%) type 3 injuries. Clinical evaluation included the Simple Shoulder Test, Constant score, pain score of 0 to 10, and satisfaction graded 0 (not satisfied) to 4 (very satisfied). Fourteen patients had complete outcome scores at the final follow-up. Nine patients underwent radiographic examination and were assessed for coracoclavicular distance, posterior acromioclavicular subluxation, arthritis, ossification, and hardware displacement by 3 observers.
Results:
The respective mean preoperative, 2-year, 5-year, and 15-year outcome scores were as follows: 34.5 ± 6.9, 94.3 ± 3.2 (P < .05), 91.5 ± 4.7, and 91.2 ± 4.8 (P > .05) for the Constant score; 2.8 ± 2.1, 12.0 ± 0 (P < .05), 11.8 ± 0.5, and 11.7 ± 0.4 (P > .05) for Simple Shoulder Test; and 4.5 ± 1.9, 0.3 ± 0.5 (P < .05), 0.3 ± 0.6, and 0.4 ± 0.8 (P > .05) for pain. The 2-year satisfaction was 4.0 ± 0; the 5-year score, 3.8 ± 0.5; and the 15-year score, 3.7 ± 0.4 (P > .05). Coracoclavicular distance (mm) decreased from 20.5 ± 4.6 preoperatively to 10.5 ± 3.6 at 2 years (P < .05), 11 ± 3.2 at 5 years, and 11.3 ± 4.3 at 15 years of follow-up (P > .05). Acromioclavicular posterior subluxation remained unchanged (P > .05). Six patients (67%) had asymptomatic ossification of the coracoclavicular ligaments; their Constant score was 93.3. One patient developed acromioclavicular arthritis radiologically with clinical correlation but did not require further surgery. Three patients (10%) underwent revision stabilization within 3 months, 1 for infection and 2 for mechanical failure.
Conclusion:
Fifteen years postoperatively, good clinical results persisted and anatomic reduction was overall maintained, often with asymptomatic ossification of the coracoclavicular ligaments.
Acromioclavicular joint (ACJ) injuries account for approximately 12% of all shoulder injuries. 3 The first arthroscopically assisted ACJ reconstructions were described in the early 2000s, 24 allowing for a simultaneous assessment of the glenohumeral joint. Although a variety of surgical techniques have been described since then, there is still no consensus on the best treatment modality. Both single- and double-bundle techniques are being used for ACJ reconstruction. 3 However, double-bundle reconstruction generally leads to superior biomechanical stability compared with single-bundle techniques.2,7,27 This reconstruction better restores native anatomy. In double-bundle techniques, the lateral and medial bundles of a double-bundle reconstruction represent the trapezoid and conoid ligaments. As part of the coracoclavicular (CC) ligament complex, the trapezoid and conoid bundles provide anteroposterior and superoinferior stability, respectively. 13 Anatomic reconstruction techniques should therefore aim to restore the native anatomic relationship of both these bundles after ACJ injury.1,11,13
Our group developed an arthroscopic reconstruction technique to separately anatomically repair the torn CC ligaments using 2 suture button devices in the acute phase after injury. 21 Because tunnel and button placement have been shown to be of paramount importance in avoiding postoperative failure or loss of reduction, this technique should be performed by experienced arthroscopists. 4 Both short-term and midterm findings have previously shown encouraging results.21,25 However, to our knowledge, no long-term results of arthroscopically assisted ACJ reconstruction techniques have been reported to date.
The aim of this study was to report the long-term clinical and radiological outcomes of a previously investigated prospective patient cohort from our department. We hypothesized that this patient population would continue to show good clinical function and sustained anatomic reduction.
Methods
Study Design and Patient Population
We performed a prospective consecutive cohort study of a twice previously investigated (2 and 5 years postoperatively) cohort of 26 of 30 patients, who were treated with arthroscopically assisted double-bundle ACJ reconstruction for acute ACJ injuries (<3 weeks after injury 18 ) between 2006 and 2007 in our department.21,25 Of the 30 operated patients, 20 (67%) with a known endpoint were included for final analysis (Figure 1). A long-term Kaplan-Meier survival analysis was carried out. Three patients (10%) underwent revision surgery within 3 months of follow-up (2 due to mechanical failure and 1 due to infection), which constituted their study endpoint. These 3 patients were excluded from further evaluation as they were not comparable to the rest of the cohort. Follow-up with survival and satisfaction scores was available for 17 further patients at long-term evaluation at a mean of 15 years (range, 14-16 years) postoperatively. Fourteen of these had complete clinical outcome scores, whereas 3 had missing data as they were not able to present for examination again for personal reasons (very busy with work, family crisis, or other health issues not associated with the shoulder). Of these 14 patients, 9 additionally underwent long-term radiological investigation; the other 5 declined as they were symptom-free. Inclusion criteria were all patients of the prospective consecutive cohort who were previously investigated after 2 and 5 years postoperatively.21,25 Excluded were patients who were lost to follow-up before a minimum of 12 years after surgery. Institutional review board approval from Technical University Munich was applied for and granted ahead of study commencement (reference No. 2083/08 S).
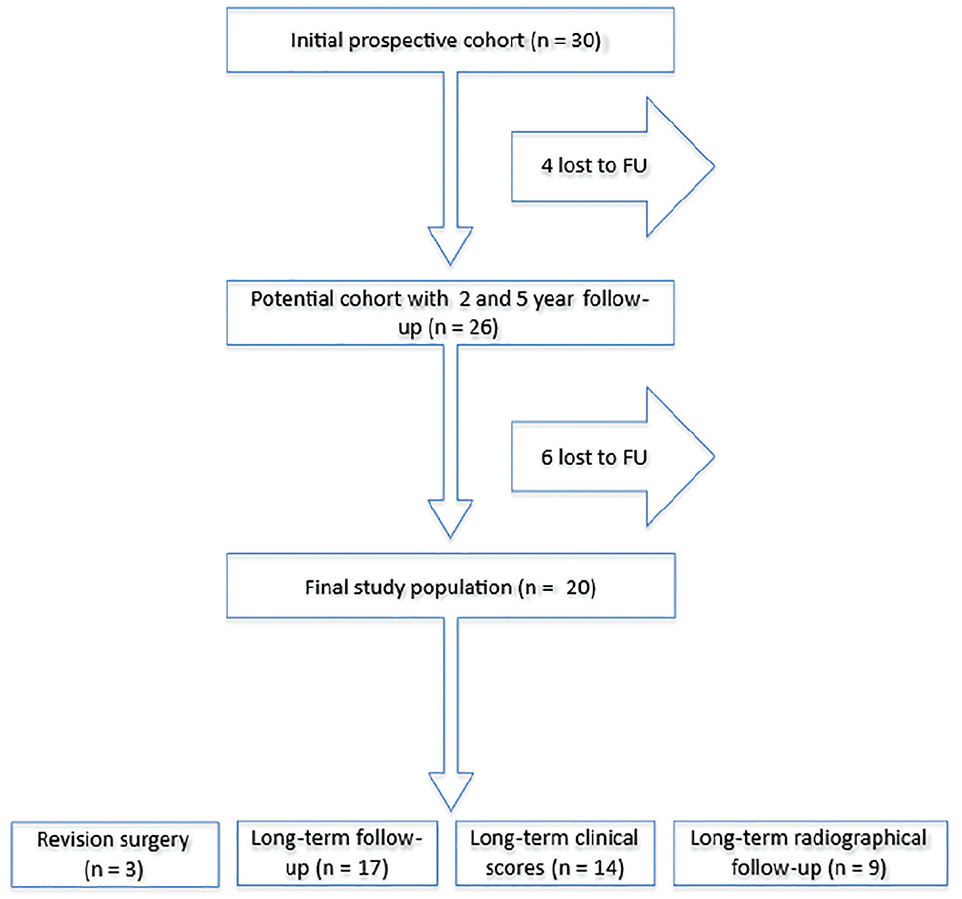
Flowchart showing the patient recruitment process. FU, follow-up.
Surgical Technique and Postoperative Rehabilitation
The surgical technique has been described in previous publications.21,25,27 Operations were performed under general anesthesia in the beach-chair position. Standard posterior, anterior, and anterolateral arthroscopy portals were established. Next, a detailed diagnostic shoulder arthroscopy was carried out to establish whether any concomitant injuries were present. Therapeutic intervention was carried out as necessary according to these findings. With the arthroscope in the anterolateral portal and the radiofrequency ablation device in the anterior portal, the inferior arch and base of the coracoid process were prepared. After this, a 3-cm incision was made over the clavicle about 3.5 cm medial to the ACJ. The ACJ was reduced through axial elevation of the arm against the scapula. Two Kirschner wires were placed through the clavicle and coracoid in the anatomic position of the trapezoid and conoid ligaments. This was carried out according to the positioning described by Rios et al 16 and Salzmann et al. 20 Then 2 independent bone tunnels were drilled with a 3.5-mm cannulated drill over the Kirschner wires through the clavicle and coracoid. Subsequently, 2 first-generation TightRope suture button devices (Arthrex) with a round clavicular and oblong coracoid button were inserted to replace the CC ligaments. The free ends of the sutures were tied with alternating surgical knots over the superior button after anatomic reduction of the ACJ, as confirmed by fluoroscopy. The deltotrapezoid fascia, subcutaneous tissue, and skin were closed and the arm put into a Gilchrist sling for 6 weeks with limited passive motion of up to 90° of abduction. Free active range of motion was resumed after 6 weeks, and return to contact sports was allowed after 6 months.
Clinical Evaluation
All patients from the previously investigated cohort were prospectively invited for clinical and radiological evaluation 2, 5, and >12 years after surgery. Clinical evaluation included questionnaires with validated patient-reported outcome measures (PROMs) and a history and clinical examination that was performed by a board-certified orthopaedic surgeon (B.D.K.). PROMs included the Simple Shoulder Test (SST), 9 visual analog scale pain score (0-10), and satisfaction (graded 1-4, where 4 = very satisfied, 3 = satisfied, 2 = partially satisfied, 1 = not satisfied). Additionally, the Constant score (CS) was calculated for each patient according to the method by Constant and Murley. 5 The minimal clinically important difference (MCID) of 16.6 points on the CS was utilized according to previous research regarding ACJ stabilization. 23 Abduction strength was measured using the Isobex isometric dynamometer (Cursor). Pain on palpation of the ACJ and pain at the ACJ elicited during the cross-body adduction test were investigated as clinical signs of arthritis of the ACJ. 12
Radiological Evaluation
All patients were offered radiological follow-up as part of the follow-up visit. Nine of the 14 patients who were available for long-term follow-up underwent radiographic investigation. This was carried out according to the previously implemented protocol to allow direct comparisons.21,25 Unilateral AP (Zanca view 29 ) stress (5-kg weight held) and axillary view radiographs were obtained and compared with previous preoperative, 2-year follow-up, and 5-year follow-up images. The CC distance was measured as the shortest interval between the apex of the superior border of the coracoid process and the opposing undersurface of the clavicula on AP stress views (Figure 2). The anteroposterior displacement was measured on the axillary view radiographs as the distance between the anterior edge of the lateral clavicula and the anterior edge of the acromion. Negative values represented posterior displacement. Tunnel widening of the clavicular tunnels was investigated on the AP stress views and measured at the inferior cortex (Figure 2). This was expressed as a mean value between the medial and lateral bundle tunnels. Coracoid tunnels were not measured as these could not be reliably visualized on radiographs in most cases. Sintering or dislocation of the suture buttons was recorded. Ossification of the CC interval was quantified according to the percentage of the distance ossified on the AP stress view. Development of ACJ arthritis was noted in comparison with the previous images. The evaluation was carried out in absolute consensus between 3 authors (B.D.K., M.H., and M.W.).
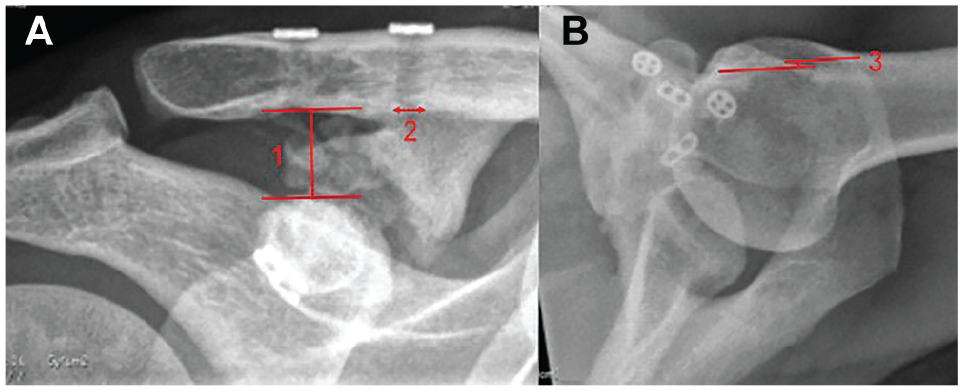
(A) Coracoclavicular distance (1) was measured from the cranial apex of the coracoid to the undersurface of the clavicula. Tunnel width (2) was measured at the inferior end of the tunnels. (B) Acromioclavicular subluxation (3) was measured as the distance from the leading edge of the clavicula to the anterior border of the acromion.
Statistical Methods
Statistical analysis was performed using SPSS Version 27.0 statistics software (IBM Corp). The Shapiro-Wilk test was used to confirm normal distribution. The 2-tailed Student paired t test was used to investigate statistical significance of normally distributed paired longitudinal values. For nonparametric data, the Wilcoxon signed-rank test was used. The significance level was set at a P value <.05. Outcome data are reported as mean ± standard deviation. A graphical Kaplan-Meier survival analysis was carried out. All available patients from the cohort were included; nonetheless, a power analysis was carried out to ensure the final cohort would be adequately powered. The power calculation was carried out using G*Power Version 3.1.9.7 statistics software (HHU Duesseldorf). To detect a change of half of the MCID for the CS (half of 16.6 = 8.3 points) at a standard deviation of 4.7 (from our published midterm follow-up data), a standard error of 1.766 was calculated.23,25 Under these assumptions, with the significance level set at an α of .05 and a power of 95%, for a 2-tailed paired t test a minimum sample of 7 patients was required.
Results
Patient Characteristics
Fourteen of the 17 patients included at final follow-up were male. The mean age at surgery was 35 years (range, 18-50 years) and correspondingly 50 years at final follow-up. Preoperative diagnosis was an ACJ injury according to Rockwood 17 type 5 in 12 cases (60%), type 4 in 6 cases (30%), and type 3 in 2 cases (10%). Additionally, 5 patients (29%) were found to have superior labrum anterior-posterior (SLAP) tears and were treated with concomitant biceps tenotomy and subpectoral tenodesis accordingly. The mean time from injury to surgery was 8 days (range, 2-20 days).
Survival Analysis
Three patients required surgical revision of the stabilization. All these failures occurred within the first 3 months postoperatively. Two of these patients had mechanical failure, and 1 had a postoperative infection. The Kaplan-Meier survival curve is presented in Figure 3.
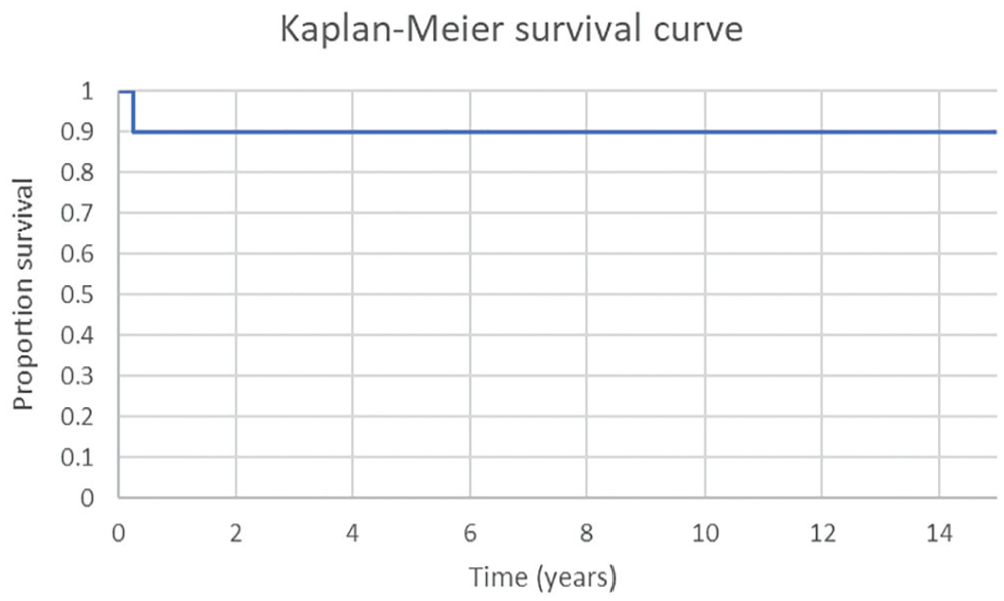
Kaplan-Meier survival curve of the initial cohort of 30 patients.
Clinical Outcomes
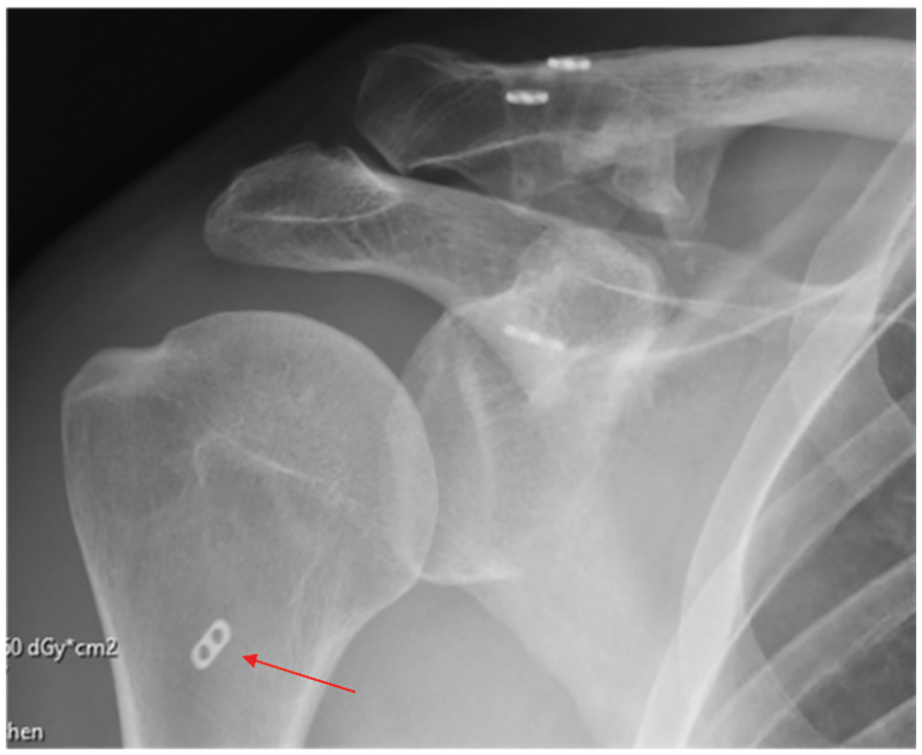
The change in PROM scores over the postoperative follow-up period from preoperatively is shown in Figure 4. The longitudinal functional outcomes as quantified by the CS are presented in Figure 5. At the 15-year follow-up, the 4 patients who had undergone concomitant tenodesis of the long head of the biceps tendon for concomitant SLAP tears had a comparable clinical result to the rest of the cohort (CS, 92.8). Two patients described a mild discomfort on palpation of the clavicular buttons; all others were symptom-free. One patient (7%) described moderate palpatory pain of the ACJ as well as moderate superior shoulder pain during the cross-body adduction test and was found to have radiological signs of arthritis of the ACJ (Figure 6) but did not undergo further surgery. No other patients showed clinical or radiological signs of arthritis of the ACJ.
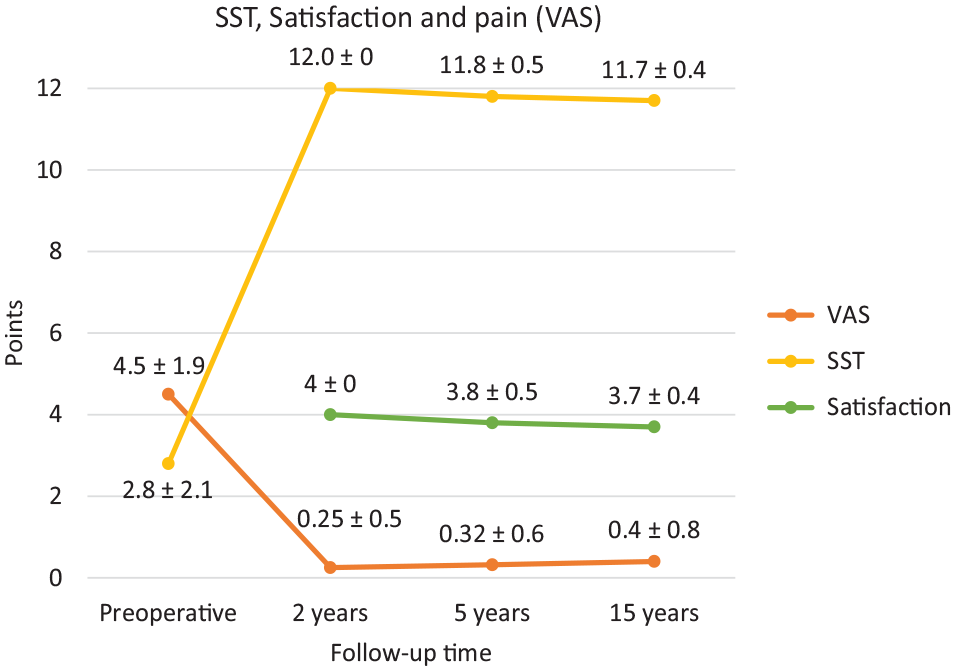
Development of patient-reported outcome measurements (mean ± SD) from preoperatively to long-term follow-up. Statistical significance was reached between preoperative and all postoperative values of the visual analog scale (VAS) and Simple Shoulder Test (SST) (P < .05). There was no significant difference between 2-, 5-, and 15-year follow-up scores for VAS, SST, or satisfaction (P > .05).
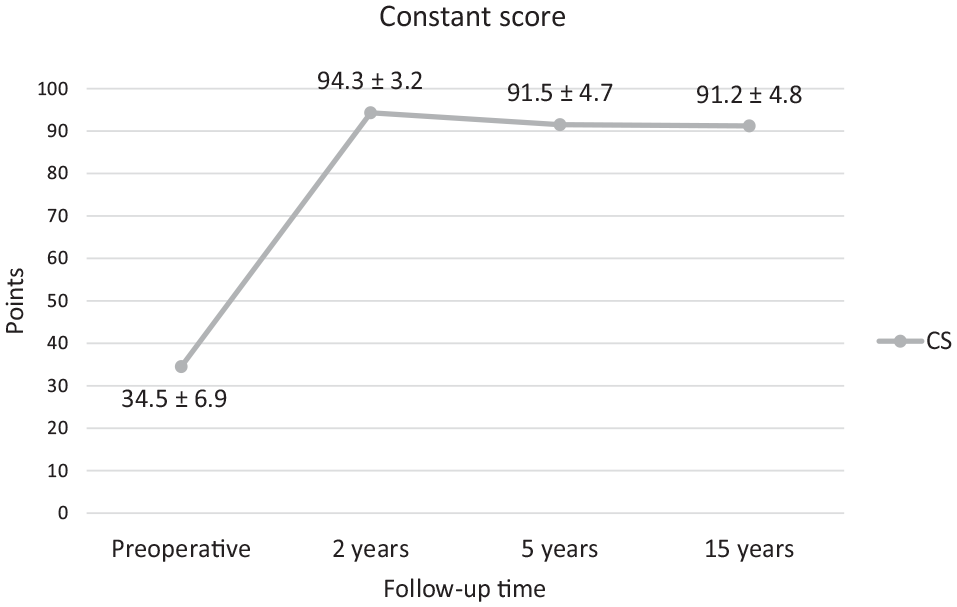
Outcome values of the Constant score (CS) (mean ± SD) presented over time from preoperatively to long-term follow-up. Statistical significance was reached between preoperative and all postoperative values (P < .05). There was no statistical difference between postoperative values of any time points (P > .05).

AP radiograph of the acromioclavicular joint (ACJ) (Zanca view) 15 years postoperatively obtained in the 1 patient with clinical signs of arthritis of the ACJ, showing joint space narrowing and osteophyte formation at the ACJ. No other patients showed clinical or radiological signs of arthritis of the ACJ. Ossification of the coracoclavicular ligaments was a commonly seen phenomenon.
Radiological Outcomes
The CC distance measured on AP radiographs preoperatively and at each follow-up time point remained unchanged compared with short-term and midterm follow-up, as shown in Figure 7 and illustrated by Figure 8.
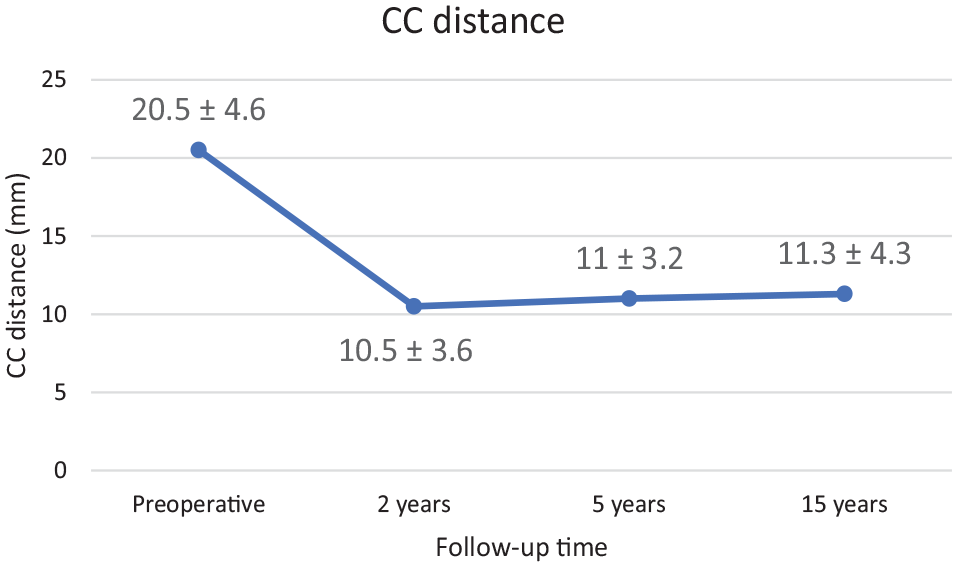
Measured coracoclavicular (CC) distance (mean ± SD) at each follow-up time point. There was a statistically significant difference between preoperative and all postoperative values (P < .05). There was no significant difference between any postoperative values (P > .05).

AP radiograph obtained in a patient 16 years after surgery with sustained anatomic reduction of the acromioclavicular joint (ACJ). There are no signs of ACJ arthritis, tunnel widening, or material failure.
Posterior subluxation of the ACJ did not significantly change between midterm and long-term follow-up (–3.0 ± 6.7 mm at 5 years; –3.5 ± 3.1 mm at 15 years). Previously, no significant change had been found between 2-year and 5-year findings from this cohort. 25
Ossification of the CC ligaments was found in 6 patients at long-term follow-up (66%; 60% at 5 years and 30% at 2 years of follow-up). In 1 patient, this involved 10% of the CC interval; in 2 patients, 50%; and in 3 patients, >80% (Figure 9). The extent of ossification showed slight progression in only 1 patient at long-term follow-up (from 76% at 5 years to 88% at 15 years of follow-up). This radiological phenomenon showed no relationship with the clinical result, and the mean CS of patients with ossification of the CC ligaments was 93.3, with no statistical difference from the rest of the cohort (P > .05).
AP (Zanca view) radiograph showing extensive ossification of the coracoclavicular interval 15 years postoperatively. Clinically, the patient remains very satisfied, with a Constant score of 89 points. There is no evidence of arthritis of the acromioclavicular joint and perfect, unchanged position of the suture buttons without tunnel widening.
There was no change in the width of the clavicular bone tunnels between the 2-year, 5-year, and 15-year radiographs. One patient showed early signs of osteoarthritis of the glenohumeral joint with a 2-mm inferior humeral osteophyte at long-term follow-up but was subjectively very satisfied and had a CS of 90 (CS of 97 at midterm follow-up 10 years earlier). Subsidence or dislocation of the suture buttons was observed in 2 patients. One patient showed subsidence of 2 mm and 5 mm, respectively, of the medial and lateral round clavicular buttons at 48 months postoperatively, but this remained unchanged 14 years after surgery without a measurable loss of reduction of the ACJ (Figure 10).

Fourteen-year follow-up radiograph showing subsidence of the round clavicular suture buttons, which was first seen 48 months postoperatively and remained unchanged after that. No measurable loss of acromioclavicular or coracoclavicular reduction was noted.
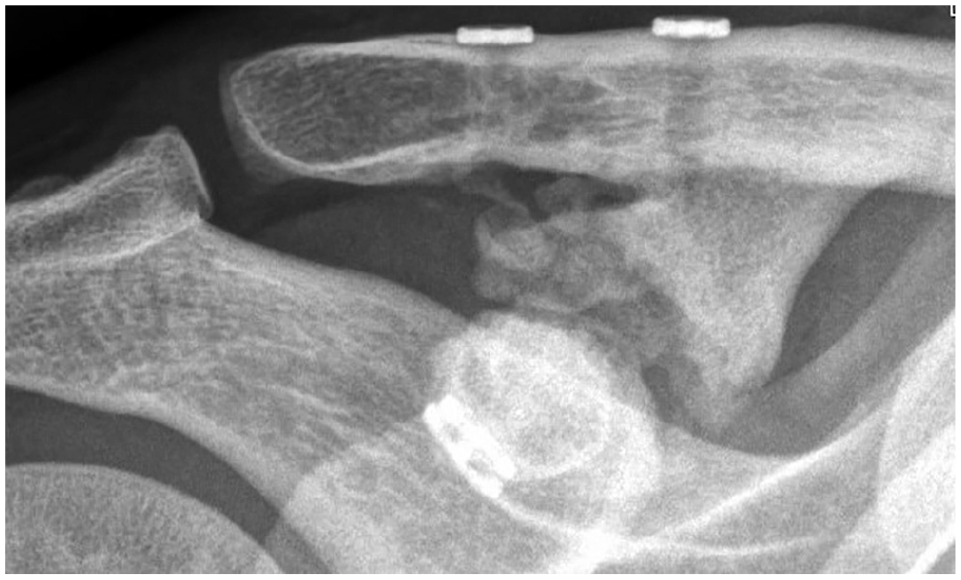
The other patient reported experiencing an injury during forestry work 3 months before the long-term follow-up appointment 14 years postoperatively. Since the injury, he has described some pain on maximal abduction of the shoulder or when carrying heavy loads. His radiographs and additional magnetic resonance imaging scan revealed dislocation of one of the coracoid buttons, which had come to lie in the inferior joint capsule, and sintering of the clavicular button of the other bundle (Figure 11). The dislocated coracoid button was removed arthroscopically, and after a further 3 months, the patient’s symptoms had resolved. A 5-mm loss of CC reduction was noted radiographically.
AP radiograph obtained in a patient with an injury to his operated shoulder 3 months before his 14-year follow-up appointment. The coracoid button from the medial bundle had dislocated and come to lie in the inferior joint capsule. The clavicular button from the lateral bundle had subsided into the clavicular bone. The dislocated button was removed arthroscopically. A 5-mm loss of coracoclavicular reduction was noted. The red arrow points to the dislocated coracoid button.
Discussion
Key Results
Our findings show that good clinical and radiological results using arthroscopically assisted double-bundle ACJ reconstruction are maintained at long-term follow-up. The MCID for the CS was surpassed, and patients were, on average, very satisfied at all follow-up time points. While AC and CC reduction remained largely unchanged, a commonly seen radiological phenomenon was an asymptomatic ossification of the CC ligaments, which progressed throughout the follow-up period. We can therefore overall accept our initial hypothesis.
Limitations
As is often a problem with long-term follow-up studies, we had difficulty in recruiting patients for a further analysis. This was due to patients having moved to another region or country or not being reachable under their known contact details. While it is likely that patients with complications would present to our tertiary referral clinic, it is possible that further revision surgery of the cases lost to follow-up was performed externally, limiting the reliability of our survival analysis to some extent. Of the 14 patients with complete clinical data at long-term follow-up, a further 5 refused radiographs to avoid radiation as they felt subjectively well. This limits the extent to which the results of the radiological analysis can be applied to the entire cohort.
Furthermore, as radiographs are a 2-dimensional imaging modality, the exact 3-dimensional position of the clavicle with respect to the coracoid process and acromion of the scapula may not be measurable. To combat this to some extent, we used reproducible standardized radiographic views in 2 orthogonal projections. However, dynamic translation cannot be accounted for using these images.
Interpretation
To our knowledge, there are no other published long-term studies of arthroscopically assisted ACJ reconstruction techniques.
Panagopoulos et al 15 recently published a study reporting on a cohort of 72 patients 6.3 years after stabilization of acute ACJ injuries with double cross-looped CC fixation using 4 Ethibond sutures. In contrast to our cohort, their cohort included mostly Rockwood type 3 injuries. Like our study, they also frequently reported asymptomatic ossification on postoperative radiographs. 15 Nine of 72 patients (12.5%) had a moderate loss of reduction, 2 (2.8%) had a recurring ACJ dislocation, and 1 (1.4%) experienced a fracture to the lateral clavicula. 15 The midterm CS was 92.1 and therefore comparable to that found in our cohort. 15 In comparison with the technique used in our cohort, perhaps this represents a viable low-cost alternative for lower-grade ACJ injuries.3,18 Aligned with this, a long-term follow-up study of a technique consisting of open acromioclavicular ligament repair and temporary Kirschner wire fixation of the ACJ reported satisfactory results in a patient cohort of Rockwood type 3 ACJ injuries. 10
For chronic Rockwood type 3 and type 5 ACJ injuries, Muench et al 14 recently showed maintained functional improvements 10 years after open anatomic CC ligament reconstruction using a tendon allograft.
Scheibel et al 22 suggested that despite overall good short-term clinical results of arthroscopically assisted double-bundle CC reconstruction for the treatment of acute ACJ dislocation, a recurrence of dynamic posterior instability was observed in some patients, and this was accompanied by inferior results. Biomechanical studies, some of which were carried out by our group, have since suggested the need for an additive acromioclavicular stabilization to prevent dynamic posterior translation of the ACJ.2,19,28
Arthroscopically assisted CC reconstruction with an additive AC cerclage has been investigated as an alternative technique to stabilize high-grade ACJ dislocations in both the superoinferior and anteroposterior plane, with good early results.6,8,26 Hann et al 8 published a CS of 90 points 2 years after arthroscopically assisted CC reconstruction with an additive AC cerclage, which, considering their cohort included only Rockwood type 4 injuries, seems comparable to the results of our cohort at early clinical follow-up.
A comparison between open hook plate and arthroscopically assisted double-bundle suture button stabilization for acute ACJ injuries by Stein et al 23 showed slightly superior results using the arthroscopically assisted double-bundle suture button technique, with a CS of 95.5 versus 91.1 at 2 years postoperatively. These data reproduce our 2-year results using a comparable arthroscopically assisted technique.
Further comparative and longer-term studies are required to determine the individualized benefits of operative techniques available. 1
Generalizability
The generalizability of our study is somewhat limited by the small sample size of young (aged 18-50 years), mainly male patients. However, this sample reflects the population that commonly requires this operation.
Conclusion
Fifteen years after arthroscopically assisted double-bundle CC reconstruction, good clinical results persisted and radiological anatomic reduction was overall maintained, often with asymptomatic ossification of the CC ligaments.
Footnotes
Submitted October 22, 2024; accepted May 1, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.B.I. has received consulting fees and royalties from Arthrex. S.S. has received consulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.