
Abstract
Introduction:
The purpose of this study was to evaluate the results of total knee arthroplasty for patients with ankylosed knees.
Methods:
We evaluated seven patients (10 knees) who underwent total knee arthroplasties for ankylosed knees from 1995 to 2008. There were two men and five women, with a mean age of 44.1 years (42–48 years). The mean follow-up period was 10.2 years (1–19.5 years). A rectus snip was performed in all cases, and V-Y quadricepsplasty was used in one case of severe quadriceps contracture. In all cases, we used the PFC Sigma PS fixed model (DePuy Orthopaedics Inc., Warsaw, Indiana, USA). The goal was more than 90° of flexion. Clinical evaluation was performed using range of motion (ROM), Knee Society (KS) Knee Score, KS Function Score, and complications. Radiographs were used to evaluate loosening or osteolysis.
Results:
The ROF was improved from 9.5° (0–30°) to 78.5° (15–115°), The Knee Score improved from 42.6 (25–70) to 68.6 (41–97), and the Function Score improved from 39 (0–60) to 66 (40–90). A radiolucent line was detected in two cases (one patient) around the tibial component, and one case had a necrosis of skin edge. Only one case had no improvement of motion.
Conclusion:
Total knee arthroplasty conversion for patients with ankylosed knees can achieve good results for motion and function without osteotomy of the tibial tuberosity when there is good quality soft tissue of the thigh.
Introduction
Recently, total knee arthroplasty has been performed in patients with ankylosed knees. However, postoperative problems may include difficulty with range of motion (ROM), wound healing, and infection. 1 –3 There may be operative field of view limitations due to intra-articular adhesions from previous surgery or contractures of periarticular soft tissue. Therefore, extensile approaches, including rectus snip exposure, V-Y quadricepsplasty, or tibial tuberosity osteotomy, have been needed in many cases. 4 –8 These approaches were used for total knee arthroplasty with ankylosed knees by many surgeons, and several advantages and disadvantages were reported. 5,6,9,10 The advantages of the rectus snip are that it is simple and is closed in routine fashion, and there is no change in the standard postoperative rehabilitation protocol. 11 However, there is a disadvantage in direct violation of the quadriceps tendon. V-Y quadricepsplasty incision stops short of the inferior lateral geniculate artery to preserve the blood supply and has the advantage of lengthening of the extensor mechanism. However, this can cause extensor lags, avascular necrosis of the patella, or delayed rehabilitation. 6,9 Tibial tuberosity osteotomy can be used for removal of a well-fixed tibial stem and to reposition the tibial tubercle to adjust the position of the patella in patella baja. However, several disadvantages are reported, including nonunion, tibial fracture, wound healing problems, extensor tendon disruption, and delayed rehabilitation. 9,10 Among these approaches, the rectus snip approach is simple and allows early rehabilitation and typically patellar eversion and excellent exposure in stiff or ankylosed knees.
The purpose of this study was to evaluate the results of total knee arthroplasty for patients with ankylosed knees using a rectus snip and gradual soft tissue release, which can reduce the damage to the extensor mechanism and soft tissue.
Materials and methods
We evaluated seven patients who underwent 10 total knee arthroplasties for ankylosed knees from 1995 to 2008. There were two men and five women with a mean age of 44.1 years (42–48 years). The mean follow-up (F/U) period was 10.2 years (1–19.5 years). The mean duration of ankylosis was 21.7 years (15–40 years). The diagnosis was rheumatoid arthritis in six knees (three patients) and pyogenic arthritis in childhood in three knees. One patient had sequelae after joint fracture. Routine F/U examination took place 3 months and 1 year after surgery, and yearly thereafter. At these intervals, the patients were examined clinically and radiologically. The Knee Society (KS) Knee Score and the KS Function Score were used for clinical evaluation. Table 1 describes the initial diagnosis and deformities observed at the time of preoperative assessment.
Patient demographics.

M: male; F: female; L: left; R: right; RA: rheumatoid arthritis; ROM: range of motion.
Operative technique
All operations were performed by the same surgeon. A midline skin incision was used with a medial parapatellar capsular approach, and the patella was dislocated laterally after osteotomy between the patella and femur. A rectus snip was performed in all cases (10 knees; Figure 1), and a V-Y quadricepsplasty was performed in one knee in a case of severe quadriceps contracture. Osteotomy of the tibial tuberosity was not required.
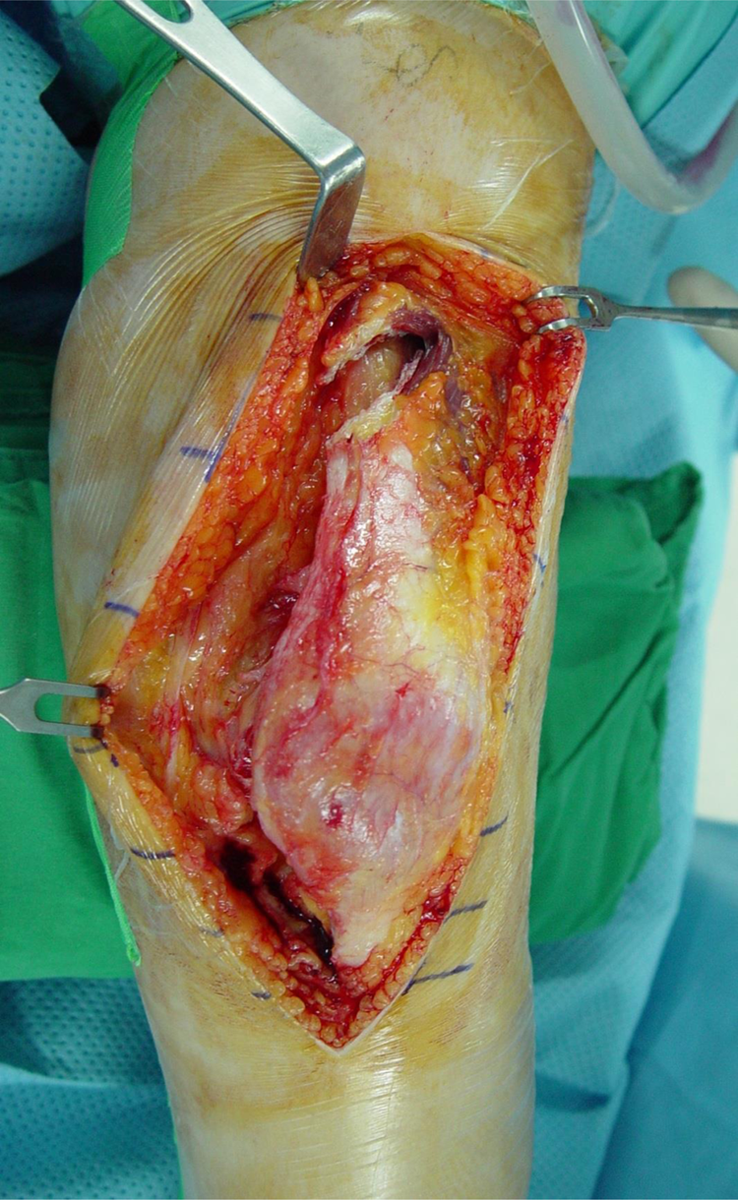
Intraoperative photograph using rectus snip approach to the ankylosed right knee.
The osseous ankylosis was taken down with attention to preservation of bone stock and careful preservation of the medial and lateral soft tissue sleeves. Intramedullary instrumentation was used for the femur and extramedullary instrumentation for the tibia. Soft tissue balancing was performed. The stability of the knee was assessed using stress radiographs with the knee in full extension and 90° of flexion after insertion of the trial components. In all cases, we used the PFC Sigma PS fixed model (DePuy Orthopaedics Inc.; Figure 2(a) and (b)). The goal was to come to rest at more than 90° of knee flexion with gravity at the end of the operation. Patellar resurfacing was not performed in all knees because of poor bone stock. Closed suction drainage was used in all knees and maintained for 48 h. All wounds were closed in 60° flexion with absorbent dressings. The knee was splinted in 90° flexion.

(a) Preoperative radiographs of a 43-year-old woman with rheumatoid arthritis showing osseous ankylosis of both knees. (b) Postoperative radiographs following bilateral total knee arthroplasty at an interval of 5 months. (c) Both knees can be flexed to 105° after 2 years postoperatively. (d) Radiographs after 6 years postoperatively show well-positioned implants without radiolucent lines at the bone–cement interface.
On the third postoperative day, not immediately, active, assisted, and gentle passive ROM exercises were started due to direct incision to the tendon of rectus femoris. Continuous passive motion (CPM) was used in patients with good quality skin and soft tissues. We used a removable night splint for a few weeks in patients where a residual flexion limitation was present after surgery. ROM exercises were carried out using a CPM machine for 4 weeks postoperatively and were then continued intensively for 3 months.
Statistical analysis
We used the Wilcoxon signed rank test to compare preoperative and postoperative variables. Statistical significance was assumed at p < 0.05.
All statistical analyses were performed with SPSS Statistics version 19.0 (IBM Co., Armonk, New York, USA).
Results
The mean ROM improved from 9.5° (0–30°) preoperatively to 78.5° (15–115°) at the final F/U (p = 0.005; Figure 2(c) and (d)). One case achieved only 15° flexion due to severe quadriceps contracture.
The mean KS Knee Score improved from 42.6 (25–70) to 68.6 (41–97) points, (p = 0.005) and the mean Function Score improved from 39 (0–60) to 66 (40–90) points (p = 0.007)
Six of seven patients had significant reduction in pain following surgery. Table 2 summarizes the results, including the current degree of deformity, the degree of movement obtained after a minimum of 1 year of F/U, and the KS Knee Score and Function Score assessments.
Results of total knee arthroplasty in patients with ankylosis of the knee after final F/U.
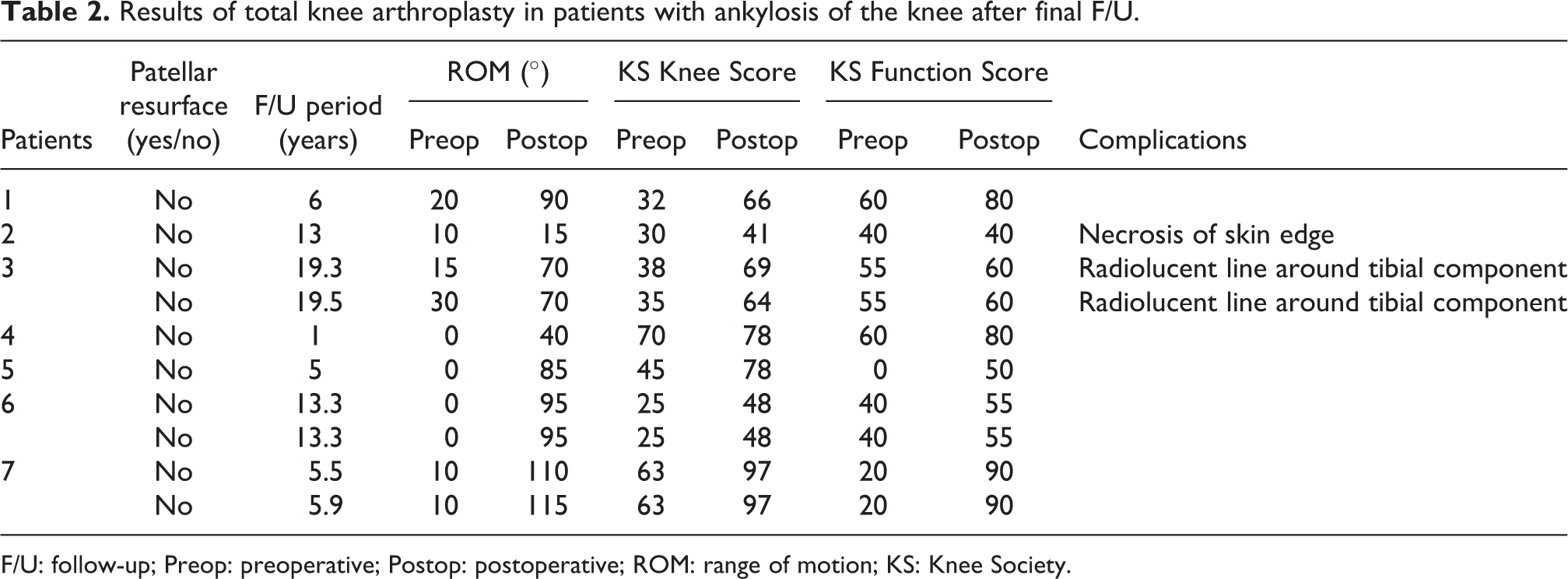
F/U: follow-up; Preop: preoperative; Postop: postoperative; ROM: range of motion; KS: Knee Society.
Postoperative complications occurred in three knees. Two knees showed radiolucent lines around the tibial component. These were incomplete, nonprogressive, asymptomatic, and less than 2-mm wide over the period studied. Skin necrosis of the incision edge occurred in one knee and resolved with conservative treatment.
Discussion
In this study, there were good clinical and radiological results after total knee arthroplasty for patients with ankylosed knees without need for tibial tuberosity osteotomy or constrained prosthesis.
Total knee arthroplasty conversion in ankylosed knee joints requires extensile approaches such as the rectus snip, V-Y quadricepsplasty, and tibial tuberosity osteotomy. Adequate knowledge of extensile exposure techniques is important to avoid intra and postoperative complications. The rectus snip was developed by Insall to assist in exposing stiff knees. 12 Following a long medial parapatellar arthrotomy, an oblique incision is made at the proximal apex of the quadriceps tendon at an approximately 45° angle directly in line with the fibers of the vastus lateralis. Several authors reported good results with this method in stiff knees. Garvin et al. and Barrack et al. reported no difference in clinical results including quadriceps strength compared to a standard approach. 4,5 V-Y quadricepsplasty was described by Coonse and Adams for the exposure of the stiff knee, 13 involving a V-shaped turndown of the entire distal quadriceps; this was modified by Insall using a standard medial parapatellar incision, extending distally and laterally at 45° along the tendinous portion of the vastus lateralis. 12 Tibial tubercle osteotomy was described by Dolin and later modified by Whiteside. 8,14 Whiteside and Ohl used this method for difficult total knee arthroplasty, which became popular for exposing ankylosed knees. 15 This method involves using an oscillating saw to transect the tibial crest 8–10 cm below the tibial tubercle while elevating the tibial crest from the tibia.
Many authors reported variable results for total knee arthroplasty in stiffness or ankylosis. Kim and Kim reported the results of total knee arthroplasty with 99 ankylosed knees. 16 They used V-Y quadricepsplasty in 73%, without osteotomy of the tibial tubercle. Mean ROM improved to 79°, and clinical results, including Hospital for Special Surgery, KS, and Western Ontario and McMaster University Osteoarthritis index scores improved significantly. However, 27% of patients had complications and needed additional treatment. Bhan et al. reported satisfactory results in 26 total knee arthroplasties for ankylosed knees using four posterior-stabilized implants and 22 condylar constrained prostheses. 17 The arc of flexion improved from 0 to 3–77, but there were major complications in four of the 26 knees. Camanho reported good results with total knee arthroplasty in nine ankylosed knees followed up for at least 5 years, with 63° motion and a significant reduction in pain. 7 Two cases of late infection requiring surgical cleaning were reported. Naranja et al. reported high complication and revision rates in patients who had arthroplasty for ankylosed knees. 18 They reported a 57% complication rate, including 24% short-term complications and 35% major complications, with a 14% infection rate. Suh et al. performed total knee arthroplasty with an extensile rectus snip approach using posterior-stabilized prosthesis in the ankylosed knee with a previous history of patellectomy, and a satisfactory result was obtained with the improvement of motion. 19
Similar to the results of previous publications, we obtained good clinical results after total knee arthroplasty for patients with ankylosed knees. ROM improved from 9.5° to 78.5°, and clinical scores including the KS Knee Score and Function Score also improved in our study. Three complications, including two cases of radiolucent lines around the tibial component and one case of necrosis in the skin edge of the incision occurred, but there were no major complications, and further surgical treatment was not needed. Immobilization in 90° flexed knee after total knee arthroplasty in ankylosed patients may cause anterior skin problem. However, we tried the knee fixed 90° to allow lengthening extensor mechanism by stretching the soft tissue, and only one case of skin problem, which was not needed surgical treatment, was occurred.
All but one of our cases had good soft tissue quality of the thigh. We utilized a rectus snip in all 10 cases, and a V-Y quadricepsplasty was also performed in one case of severe quadriceps contracture. The field of surgical view was sufficient without osteotomy of the tibial tuberosity. Therefore, we were able to perform surgery using a posterior-stabilized implant rather than a varus–valgus constrained implant, thereby preventing complications, including tibial fracture and problems in the extensor mechanism from osteotomy of the tibial tuberosity. Early rehabilitation was possible without a more extensile approach such as tibial tuberosity osteotomy. This may be meaningful to total knee arthroplasty for patients with ankylosed knees compared to other previous published studies.
There are some limitations in this study, such as its retrospective design, absence of a control group, and relatively small number of patients. Thus, we suggest that comparative and further large-scale studies should be conducted later.
Conclusions
Total knee arthroplasty conversion for patients with ankylosed knees can achieve good results for motion and function without osteotomy of the tibial tuberosity when there is good quality soft tissue of the thigh.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.