
Abstract
Background:
Clinical orthopedic research needs better ability to assess patient expectations with regard to orthopedic trauma surgery outcomes. The aim of this study was to investigate to which extent patient expectations prior to surgery could be met after surgery.
Methods:
Patients (≥18 years) with surgical ankle fractures were prospectively recruited at 5 orthopedic trauma clinics in the United States (USA), Canada, and Brazil and followed up for 12 months. Patients were asked to complete a previously validated trauma expectation factor (TEF) questionnaire prior to surgery and a trauma outcome measure (TOM) 1 year after surgery.
Results:
At 1 year, 155 patients had provided complete records. Almost half (49%; 76/155) had a 1-year TOM score equaling or exceeding their preoperative TEF score (95% CI: 41–57%). The remaining scores failed to meet patient expectations. TOM scores matched or exceeded patient expectations for 33% of patients in the USA and 47% in Canada, but for 69% in Brazil (p = 0.001 (USA); p = 0.024 (Canada)). This geographical effect was attributable to higher patient expectations in North America as compared to Brazil (average TEF scores: 36 (North America) versus 31 (Brazil); p < 0.001). Patients with lower household income or smokers were more likely to be satisfied with their treatment (p = 0.02 and p = 0.05, respectively). Furthermore, patients with severe type C fractures had better rates of satisfaction (62%) than patients with simpler B (50%) or type A fractures (33%) (p = 0.01 [C type versus A type]).
Conclusions:
Orthopedic surgeons have difficulty in meeting or exceeding presurgical patient expectations of long-term outcomes for ankle fracture surgery. This study provides evidence that culture, geography, and surgeon—patient communication have considerable influence on patient expectations.
Introduction
Governmental agencies, health insurers, and healthcare providers from various countries are shifting their focus from clinical processes to outcomes, that is, concentrating on the quality rather than the quantity of healthcare. 1 –3 How much hospitals get paid for a procedure may soon depend in part upon such measurements of outcome. 4 The United Kingdom (UK) and United States (USA) health systems are in the process of verifying the appropriateness of patient-reported outcomes (PROs) in measuring the quality—as opposed to the quantity—of treatment in their hospitals. 1,4,5 Some preliminary research has been done in the field of PROs for the area of traumatology and orthopedics, 6,7 and tools have been developed to assess patient expectations. 8 But are we actually able to meet our patients’ expectations? And are patient expectations realistic? Is there a geographic difference between patient populations and what they might expect from surgery?
Generic measures of outcome, such as the Short Form-36 Health Survey and EQ-5D questionnaire, have been proposed for chronic disease or injury, 9,10 in order to assess provider performance in improving a patient’s condition. However, these measures are inappropriate for evaluating the outcome following an acute condition, such as fracture, because trauma patients are likely never to experience their baseline (pretrauma) function again. The trauma expectation factor (TEF) tool was created to measure patients’ expected outcomes. 8 When the TEF score is compared with the trauma outcome measure (TOM) score, it provides an indicator to assess performance in the eyes of the patient. The TEFTOM tool was developed specifically to be used after traumatic injury and to investigate patient expectations in orthopedic trauma outcomes (patient expectation fulfillment).
We used the validated TEFTOM tool across a Pan-American population of ankle trauma patients and applied it to our original data set. Our research questions were as follows: Can we measure patient expectations in a Pan-American ankle trauma patient population, and can we determine the extent to which patient expectations had been met? Are certain patient demographics determinant of a better outcome after an ankle fracture? Our hypothesis was that all patients in our study group would show equal expectations for clinical outcome after recovery from their surgical ankle fracture treatment.
Patients and methods
We conducted this prospective multicenter cohort study between October 2006 and February 2010. Five participating clinics in Brazil (Ribeirão Preto), Canada (Calgary), and the USA (New York City (two sites), Jacksonville) were involved, and institutional review board approval was obtained at each center. The study was registered on ClinicalTrails.gov under the short name TEFTOM (ClinicalTrails.gov Identifier: NCT01126398). Written informed consent was obtained from all patients before enrolment.
Inclusion/exclusion criteria
The main inclusion criterion was an isolated ankle (distal tibia and/or fibula) fracture in patients aged 18 years or older. The operative procedure was to be performed within 4 weeks after the injury.
Exclusion criteria included previous internal fixation surgery of the injured ankle and medical conditions that have an impact on bone union, such as metastatic cancer and metabolic bone disease. Furthermore, poly-traumatized patients, patients with severe dementia or other severe mental health problems that would preclude them from completing study questionnaires, patients who knew that they would be unable to attend all scheduled study-related follow-up visits, patients participating in other clinical trials of a drug or device, and prisoners were excluded.
Intervention
Development and validation of the TEFTOM tools have been described elsewhere. 8 TEF and TOM are two 10-item questionnaires that cover five domains: (1) pain, (2) physical function, (3) disability, (4) injury satisfaction, and (5) overall satisfaction. The questionnaires are made available to the orthopedic community without charge at www.aofoundation.org/TEFTOM (Figures 1 and 2). The most important aspect of this tool is that the composition of each question can be easily adapted to assess not only outcome but also patient expectations at any time after the traumatic event. For example, question 1 “How painful is your injury today?” can be reworded as “How painful do you expect your injury to be in one year?” to predict the level of injury expected by patients at a future point in time. The 10 items are individually scored using a five-point rating scale; thus, each item is scored from 0 to 4 (e.g. least satisfied/most satisfied) and combined to produce a single overall score ranging from 0 (lowest outcome) to 40 (highest outcome). The TEF portion of the questionnaire was administrated preoperatively, while the TOM portion was administered 1-year postoperatively (10–20 months after surgery).
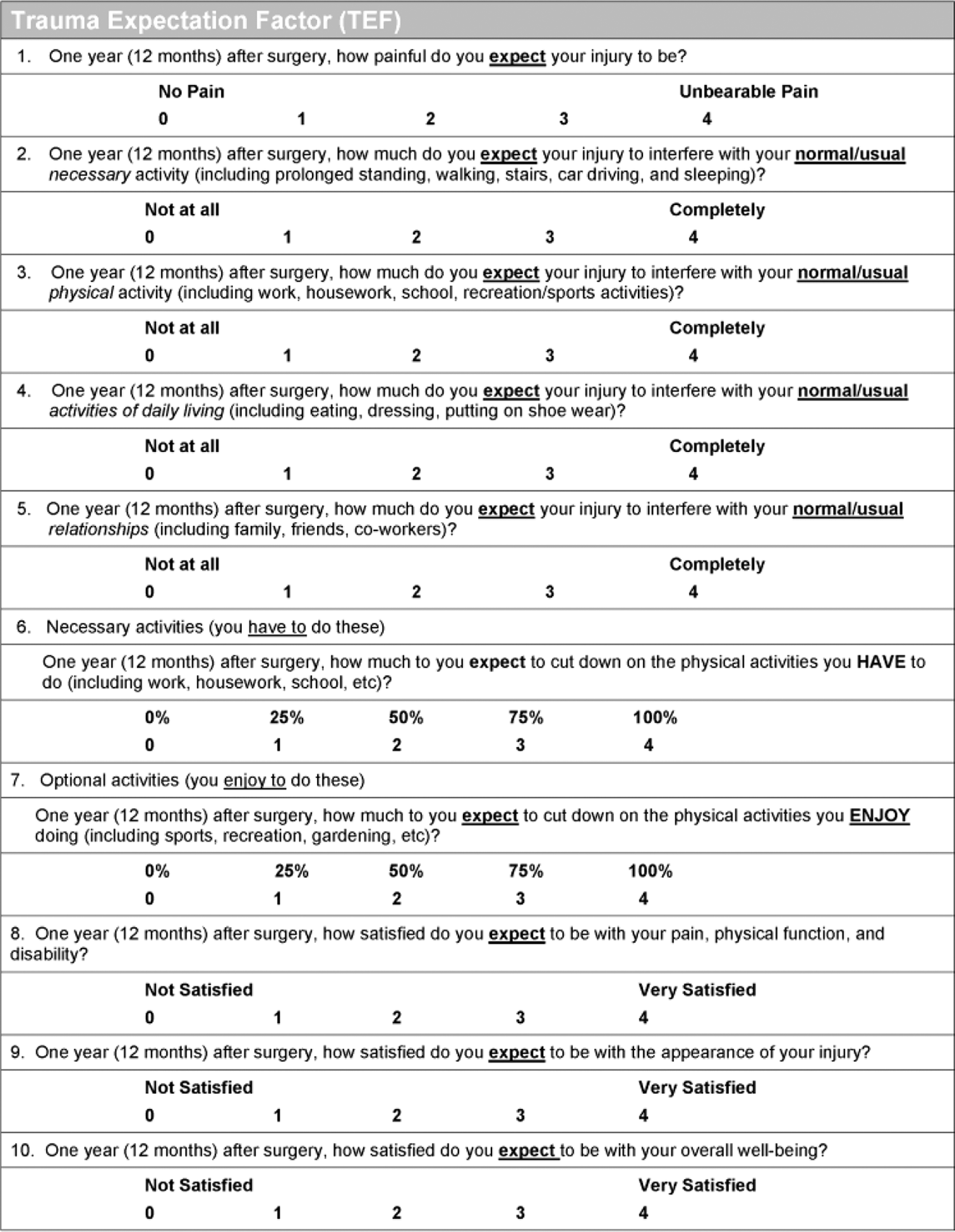
TEFTOM questionnaire validation study—The TEF questionnaire. TEF: trauma expectation factor; TOM: trauma outcome measure.

TEFTOM questionnaire validation study—The TOM questionnaire. TEF: trauma expectation factor; TOM: trauma outcome measure.
Operative intervention
A standardized protocol of surgical care was practiced in accordance with the standard care at each of the participating institutions. Half of the patients (80) were treated within 5 days after the trauma (range: 0–27 days). The median duration of the surgery was 80 min. The primary surgical intervention for 137 (88%) patients was open reduction with internal fixation, followed by 17 (11%) patients who initially received external fixation prior to the open reduction and internal fixation procedure; only 1 (1%) underwent percutaneous fixation.
Ninety-nine (64%) fractures were treated by chief surgeons who had previous experience with more than 30 of the same surgical procedures. Seventy-six (49%) operations were performed without supervision, and in 151 cases (97%), surgeons were satisfied with the final immediate postoperative outcome.
Study population
A total of 203 patients were recruited in the TEFTOM study. Two patients declined to participate in the study before surgery was performed. Four patients did not satisfy the isolated ankle fracture inclusion criteria but received a waiver from the orthopedic surgeon, who rated their secondary fractures as unlikely to interfere with their perception of the ankle fracture. Therefore, a total of 201 patients were enrolled in the study. Of these, 155 provided complete records of measurements taken preoperatively and 1 year after surgery within the specified time windows. The statistical analysis reported in this article was performed on this population of 155 patients.
Baseline patient sociodemographic characteristics are presented in Table 1. The patient population comprised 68 women (43.9%) and 87 men (56.1%), with a median age of 41 years. A majority (80.7%) of study participants were Caucasian and over half of them (54.8%; 85/155) were married. A total of 95 patients (61.3%) had only primary school or high-school education. Over 70% (114) of patients were employed, with almost two of three patients (65.8%) having an annual household income lower than $75,000. Canada, United States and Brazil (CAN, USA, BRA).
Patient sociodemographic characteristics.

SD = standard deviation.
Statistical analysis
Statistical analyses were performed using Intercooled Stata Version 11 statistical software (Stata Corp, College Station, Texas, USA).
We defined success as a 1-year TOM score that exceeded or matched the patient’s preoperative TEF score. We compared rates of success across different groups of patients in order to identify factors that are associated with success from a patient perspective. t-Test was used to compare the mean TEF score of each category with the baseline level. We performed logistic regression to compute odds ratios and associated Wald p-values. Linear regression was used to estimate the baseline TEF scores.
We based the total recruitment of 200 patients on a sample size estimation made prior to commencing this study. Since there were no good estimates of effect sizes using the TEF as a predictor, a true power analysis was not possible for this study. A ratio of 40 patients per predictor was deemed appropriate. Three independent risk factors, in addition to the TEF, were estimated to be possible predictors of TOM scores. With a total of four predictors multiplied per 40, 160 ankle fracture subjects needed to be enrolled and followed up. An estimated loss of follow-up and refusal to participate of 10% each compensated for loss of power, resulting in approximately 200 ankle fracture patients to be recruited.
Data was prospectively dichotomized as to greatly simplify the presentation of the results. Multivariate analysis was not performed as the idea of the study was to analyze the main outcome of the study as binary (despite the small disadvantage of losing a small amount of information).
Source of funding
The present clinical investigation was performed with the support of the AO Foundation via the AO Trauma Network.
Results
A total of 155 patients had both baseline and 1-year postoperative measurements taken in the specified visit windows that could be used for the evaluation. Nearly half (49%; 76/155) of the patients had a 1-year TOM score equaling or exceeding the preoperative patient TEF score (95% CI: 41–57%), while the remainder of scores failed to meet the patient’s expectations. Forty-six patients did not have complete data sets or were lost to follow up and were not kept in the final data pool for analysis. The authors know of no confounders or differences of this group of patients from the final 155 patients who had complete data sets.
Table 2 points at factors associated with success (met or exceeded patient expectations). Logistic regression did not find any association between patient expectation fulfillment and age, gender, race, employment status, marital status, premorbid medical comorbidities, sport activity, fracture location, or cause of a fracture. However, a geographic phenomenon was identified: USA and Canadian patients were less likely to meet their expectations (merely in 33% and 47% of the cases, respectively), while Brazilian patients met their expectations in 69% of the cases (Wald test p-value = 0.001 for comparison with USA and p-value = 0.02 for comparison with Canada). This effect was directly attributable to higher patient expectations in North America as compared to Brazil (average TEF score 36 in North America versus 31 in Brazil; t-test p < 0.001, both for comparison with USA and Brazil data). There was also an association between satisfaction and fracture severity: patients with severe type C fractures had better rates of satisfaction (62%) than patients with simpler B (50%) or type A fractures (33%) (Wald test p-value = 0.01 for comparison of type C versus type A). Smokers had outcome expectations that were met more often (p = 0.05). Individuals of higher income expected their outcomes to be better than individuals with lower income, resulting in lower TOM score success rates than their counterparts (p = 0.02). This was reflected by the educational level of patients, where higher educated patients presented with lower TOM success rates compared to lower educated patients (62% success for patients with primary school education compared to 33% for graduate/postgraduate patients; p = 0.07). Also, when a consultant was with a patient, their expectations were met less often than if a resident was seen as the caregiver (p = 0.01).
Factors associated with met or exceeded expectations, defined as success, in the Pan-American TEFTOM study.

TEF: trauma expectation factor: TOM: trauma outcome measure; CI: confidence interval; N/A: not applicable; OR:= odds ratio; ORIF: open reduction internal fixation; TEF: Trauma Expectation Factor; DeNovo: first and only surgery on ankle; AO: Association for the Study of Internal Fixation.
Discussion
Many variables may have an impact on the fulfillment of patient expectations regarding their anticipated orthopedic surgery and outcome. 11,12 This study showed that severity of orthopedic diagnosis, certain patient characteristics like smoking, income and education levels, and country of origin may impact both on long-term expectations and personal fulfillment after injury. Patients from the USA were the most difficult to help in relation to personal fulfillment of their preoperative expectations after ankle fracture surgery, compared to patients in Canada and Brazil.
Mahomed et al. 13 stated that patient expectations were important independent predictors of increased functional outcomes and satisfaction after total joint arthroplasty in a population of Canadian and American arthroplasty patients. Furthermore, patients with fewer medical comorbidities and increased education tended to expect better outcomes. 13 We found similar results among educated patients and those of higher income levels expecting better outcomes. Wealthier and educated patients, simply put, had higher demands from the system and were not as easily pleased with their personal outcome. However, in our study, patient expectations were not proved to have any association with age, gender, race, marital status, or type of surgery. Other authors 11,13 had documented this as well supporting the fact that many demographic features play little role in long-term patient satisfaction.
Patients in our study expected a good outcome after surgery despite having a range of ankle fracture types. Although this could not be statistically confirmed, expectations of patients experiencing worst type C fractures seemed to be lower than those of patients with less severe fractures. In turn, these patients were more accepting (higher fulfillment) than their less seriously injured colleagues. Other researchers 13,14 have found that despite worse preoperative disability or seriousness of chronic disease, patients expected equally positive results. Mancuso et al. 12 had found that excellent patient fulfillment after total hip arthroplasty was related to less severe impairment preoperatively. Conversely, having increased pain relief expectations in spine surgery can be associated with more pain and less satisfaction postoperatively. 15 In our study, patient expectations seemed to follow surgical education; if patients were told that they had a serious injury, early and long-term expectations of the patient seemed lower and more obtainable.
Smokers and patients with lower education and income levels had lower expectations and longer term personal fulfillment in our study. This concurs with other authors’ findings 16,17 who observed that the psychosocial situation and the mood of the patient can play a large role in relation to the long-term outcome of the patient. Patients with higher education and income levels in our study, regardless of site of study, expected better results than patients with less financial security. Self-efficacy (patient confidence in the ability to perform specific behaviors) has been shown to be a modifiable determinant of increased functional outcomes in other disease states. 18 Certain members of our patient population had the expectation to recover from their injury and be able to walk without any disability whatsoever. Those patients tended to be educated and of high income.
Brazilians had more fulfillment of expectations in relation to long-term functional outcomes and this was highly significant when compared to both the USA and Canadian patients. Perhaps the USA medical system creates barriers and high expectations when providing care for patients. In 2009, Snyder and Aaronson 19 reported patient-related outcomes in clinical practice. They stated that outcomes could be facilitated by addressing barriers that exist in patients’ lives and systems of care. Potentially, this is one of the issues that most affects American interpretation of medical care provision as compared to the Brazilian health care system.
In this context, cultural differences in patient expectations can be an unintentional bias and therefore, one limitation of this study. During the conduct of this study, differences in the culture may have had influence on the patient–surgeon relationship. For example, Brazilian surgeons tended to spend more time with their patients during their encounter and may have had a relevant impact on further patient expectations. With this knowledge, above-mentioned bias could have been minimized by a standardized setting of the patient–surgeon communication within this study.
The TEFTOM score was designed for the purpose of orthopedic trauma expectation assessment and specifically validated for the foot and ankle. 8 There is no reason to expect TEFTOM not to be valid for other trauma patients. Nevertheless, to improve its overall applicability, more studies on other trauma populations and including different regions should be conducted to investigate patient expectations in orthopedic trauma outcomes in a more general way.
In conclusion, orthopedic surgeons have difficulty in meeting or exceeding presurgical patient expectations with regard to long-term outcomes for ankle fracture surgery. However, recognizing that culture, geography and surgeon–patient communication have considerable influence on patient expectations, which in turn play a critical role in PROs.
Footnotes
Authors' contribution
MS was involved in study design, data acquisition, manuscript review, and manuscript approval. MD contributed in study design, data analysis, data interpretation, manuscript drafting, manuscript review, and manuscript approval. RB was involved in study design, data acquisition, data interpretation, manuscript drafting, manuscript review, and manuscript approval. DL contributed in study design, data acquisition, manuscript review, and manuscript approval. DH was involved in study design, data acquisition, manuscript review, and manuscript approval. BH was involved in study design, data interpretation, manuscript review, and manuscript approval.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.