
Abstract
Introduction
Point-of-care ultrasound (PoCUS) represents a new frontier in diagnostic imaging (DI). A portable and goal-directed alternative to conventional ultrasonography, PoCUS is performed at the bedside to answer focused diagnostic questions or guide procedural interventions. 1 Advancements in PoCUS technology have enabled high-definition, real-time visualization of anatomy that is accessible via smartphones and tablets. The growing clinical utility of PoCUS is reflected in its incorporation into practice guidelines recommending its use for procedures such as central venous catheterization,2,3 pleural procedures, 4 trauma assessments, 4 and paracentesis. 5
In plastic and reconstructive surgery, PoCUS is effective in diagnosing a wide array of hand pathologies, including tendon ruptures, ligamentous injuries, and peripheral nerve compression.6–8 In breast surgery, PoCUS aids in diagnosing seromas, hematomas, and deep tissue collections, 9 as well as in the assessment of implant orientation and device rupture.10,11 Beyond its diagnostic applications, PoCUS offers significant value as a perioperative adjunct. PoCUS guidance improves the precision and success of tendon sheath injections and peripheral nerve blocks.7,11–13 By enabling surgeons to accurately identify the precise location of structures of interest, PoCUS has been shown to enhance surgical planning and perioperative decision-making, resulting in decreased procedure time, complications, and patient morbidity.7,12,13 Despite these benefits, limited research has been conducted regarding the broader impact of PoCUS implementation on departmental workflow and quality of patient care in plastic surgery.
PoCUS also confers economic benefits and improved resource utilization. Most cost analyses have been conducted in emergency medicine, critical care, and internal medicine, where PoCUS has been associated with decreased per-patient expenditures and shortened hospital stays.14–16 The cost savings associated with PoCUS in these settings are primarily attributed to fewer unnecessary diagnostic tests, most commonly, a reduction in unnecessary DI studies.14–16 This pattern may extend to plastic surgery settings, where PoCUS can be applied to a broad range of pathologies 17 that traditionally depend on other forms of DI, such as computed tomography (CT) and magnetic resonance imaging (MRI). However, the potential impact of PoCUS on hospital resource utilization in plastic surgery has not been thoroughly studied.
To explore these potential benefits, a PoCUS program was introduced in the plastic surgery division of our academic-community hospital in Toronto, Ontario, Canada. This retrospective chart review aims to assess the impact of this PoCUS program on patient care, departmental practice patterns, and the utilization of hospital resources. Our primary objective was to understand how PoCUS was applied for patient care within our division. Our secondary objective was to examine the effect of surgeon-performed PoCUS on the utilization of hospital DI resources, with a focus on its potential to reduce DI referrals.
Methods
Study Overview
We carried out a retrospective cohort study enrolling eligible patients referred to the plastic surgery service at a single, academic-community hospital (“St. Joseph's Health Centre” in Toronto, Canda) between November 1, 2023, and October 31, 2024. Ethics approval for the study was obtained from the Unity Health Toronto Research Ethics Board. All patients who underwent a PoCUS assessment as part of their care were eligible for inclusion.
The PoCUS scans were conducted with one Clarius L15 HD3 High Frequency Scanner (Clarius Mobile Health). 18 The PoCUS assessments were completed by staff surgeons at our institution, who had undergone PoCUS training. Two surgeons received formal PoCUS training during their subspecialty fellowship, and one surgeon completed an accredited PoCUS curriculum through a continuing medical education certificate program.
Data Collection and Data Analysis
Patient charts were reviewed and data were extracted by 3 independent reviewers (RA, MR, and SV) using a standardized Excel document (Microsoft), designed a priori. Conflicts in extracted data were resolved by consensus. Patient demographic data (age, sex, and home address) were extracted. Clinical data, including the anatomic region scanned, the hospital department/site where the scan took place (eg, ambulatory clinic, minor surgery, ward), the clinical indication for the PoCUS scan and the need for any subsequent referral to DI for scans, were extracted.
To evaluate how PoCUS was utilized in our cohort, the clinical indication for each scan was classified into one of 3 categories: diagnostic assessment, procedural guidance, or surgical planning. Descriptive statistics were used to summarize the demographic data and present the clinical results.
Results
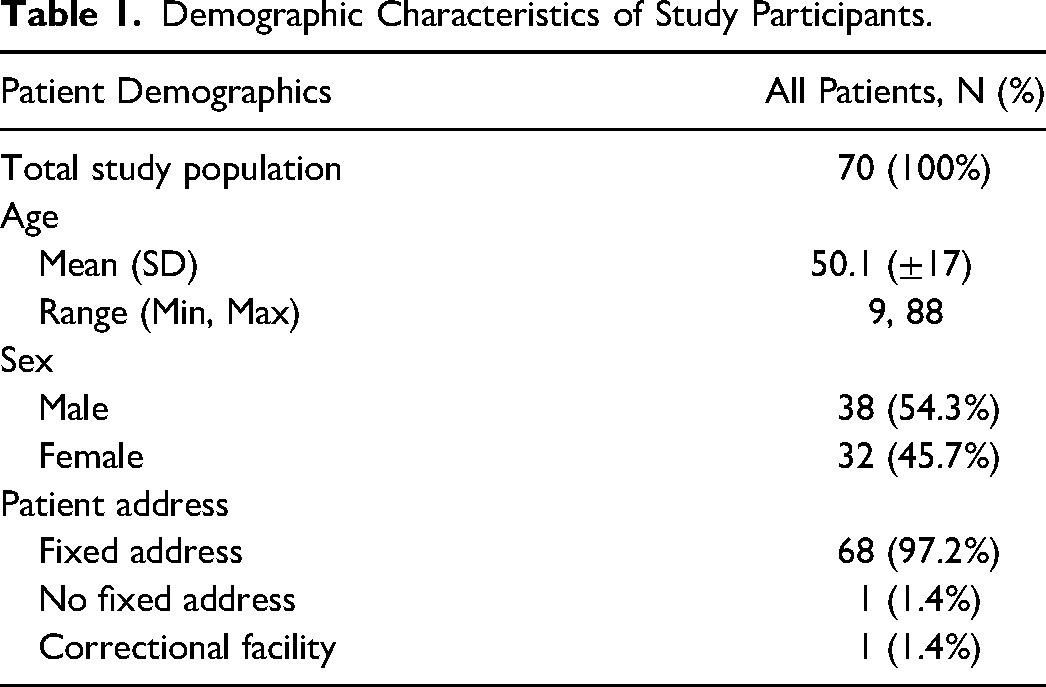
A total of 70 patients met the inclusion criteria and 72 PoCUS scans were conducted on this study population. Two patients underwent 2 PoCUS scans for different clinical indications, while the remaining patients underwent one scan each. The participants’ mean age was 50.1 years (range 9-88), and 54.3% of our study population was male. Vulnerable populations (ie, incarcerated, no-fixed address) made up 2.9% of our study population. The details of the demographic characteristics are presented in Table 1.
Demographic Characteristics of Study Participants.
The PoCUS assessments were performed primarily in the ambulatory clinic setting (65%) and minor surgery (26%), but PoCUS was also utilized in the operating room (3%), emergency department (3%), and inpatient ward (3%). The anatomical regions assessed during PoCUS most frequently were the hand (36.1%), followed by the arm (18.1%), back (13.9%), head and neck (11.1%), breast (9.7%), foot (5.6%), leg (2.8%), and chest (2.8%).
PoCUS was most frequently used for procedural guidance, accounting for 44.4% of cases (Table 2). The most common procedures were image-guided corticosteroid injections and incision and drainage (Figure 1). Diagnostic indications, such as evaluation of tendons, ligaments, soft tissue injuries, or masses, represented 37.5% of scans. Surgical planning accounted for the remaining 18.1%, including applications such as foreign body localization and perforator mapping. Table 1 details the PoCUS applications for patient care in our study.
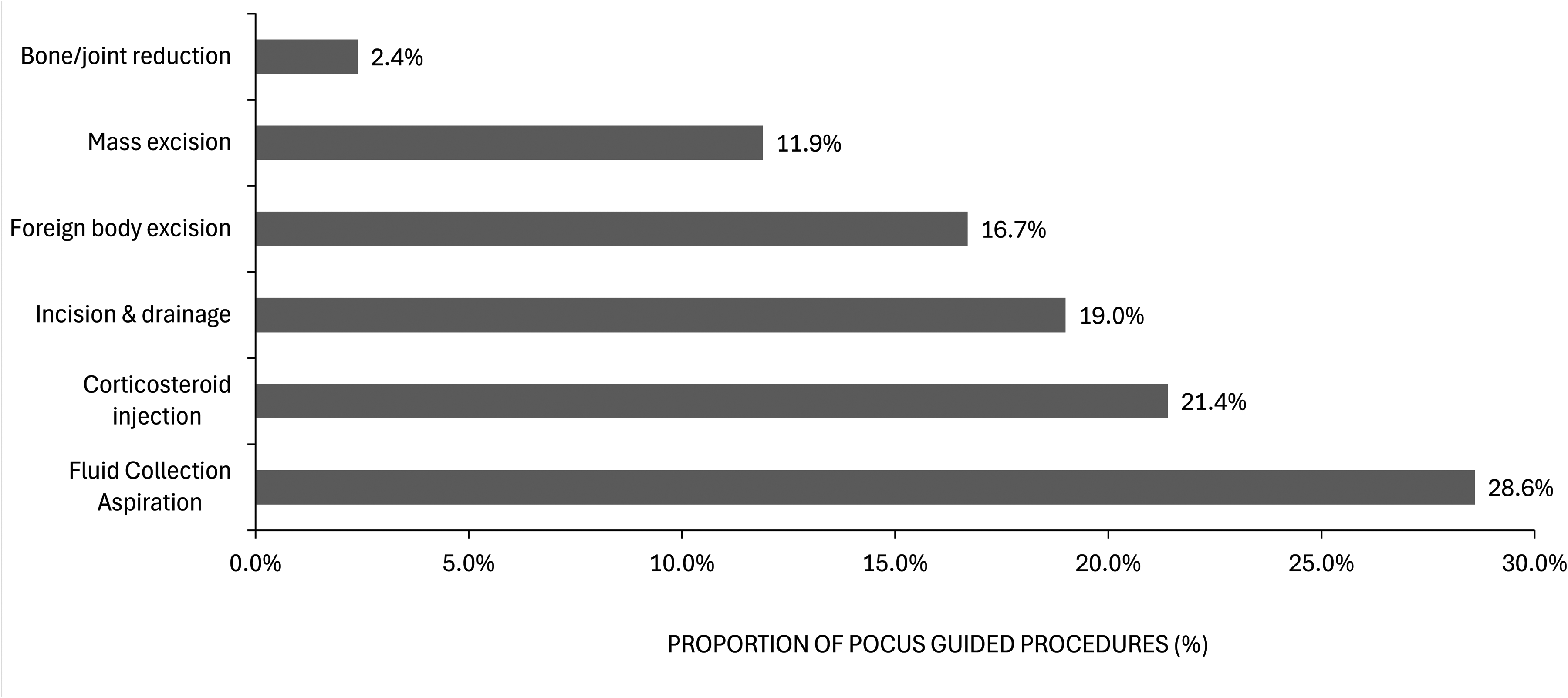
Distribution of indications for Point-of-Care Ultrasound (PoCUS)-guided procedures in the study cohort, expressed as percentages of all PoCUS procedures.
Among the 72 PoCUS scans conducted, not all patients would have typically been referred to DI for formal imaging in the radiology department. We identified 31 patients who would have been referred to radiology had PoCUS not been available in our department. Indications for further DI included foreign body assessment, breast implant/tissue expander assessment, and image guided aspiration of fluid collections (eg, breast seroma). In instances where referral to DI was indicated, PoCUS was an adequate substitute for formal DI except in one case where the findings of PoCUS assessment were inconclusive. This was for assessment of ulnar collateral ligament injury of the thumb, where diagnosis via clinical examination was not definitive. Thus, PoCUS avoided the need for further DI in 96.8% of cases where a referral to radiology would have otherwise been made.
Clinical Indications and Outcomes of PoCUS Use by Anatomical Region.
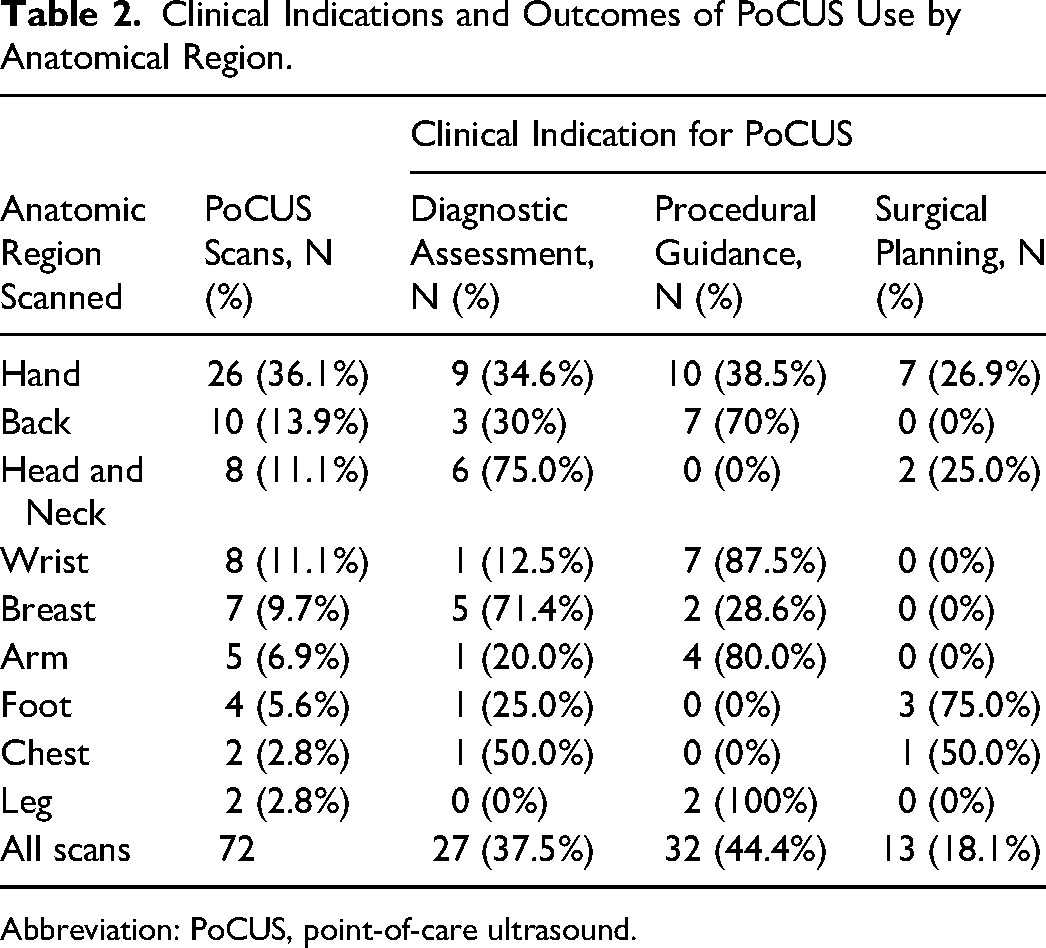
Abbreviation: PoCUS, point-of-care ultrasound.
Discussion
Procedural guidance represented the primary clinical indication for PoCUS, with ultrasound-assisted interventions performed in 44.4% of cases. Aspiration (21.4%) and injection (19.0%) were the most frequently performed procedures. 18 In these procedures, PoCUS was applied to improve technical performance and increase patient safety. These procedures are often otherwise performed using landmark-based or “blind” techniques. PoCUS, however, has been shown to improve patients’ functional outcomes and risk of adverse outcomes in these procedures relative to a landmark-guided approach.19–21
Diagnostic assessment emerged as the second most common clinical indication for PoCUS use in our cohort, reinforcing its value as a frontline diagnostic tool for the plastic surgeon. The most frequently scanned anatomical regions included the hand, arm, and back, reflecting common musculoskeletal and soft tissue concerns in outpatient plastic surgery settings. In particular, PoCUS was frequently used to assess tendon and ligamentous injuries of the hand, aligning with previous research demonstrating its accuracy in visualizing flexor tendons and collateral ligaments.6,8,22 Evaluation of soft tissue masses was another common diagnostic application.
Although surgical planning was the least common clinical indication in our study, it remains an important and emerging application of PoCUS. In selected cases, PoCUS supported operative decision-making—most notably through the localization of retained foreign bodies. This aligns with existing evidence demonstrating that PoCUS offers high specificity (92%; 95% CI: 88%-95%) and moderate sensitivity (72%; 95% CI: 57%-83%) for detecting soft tissue foreign bodies. 23 Incorporating PoCUS into preoperative assessment may improve surgical efficiency, reduce unnecessary tissue dissection, and guide incision planning.
Point-of-care ultrasound was also found to be a versatile tool applicable across a broad spectrum of patients in our department. Notably, PoCUS was used in patients facing barriers to consistent healthcare access, including individuals with no fixed address and those who were incarcerated. The study population ranged in age from 9 to 88 years, reflecting its feasibility in both pediatric and geriatric care. For these populations, the ability of PoCUS to facilitate immediate diagnostic or procedural intervention without the need for additional follow-up appointments (eg, formal ultrasound and subsequent follow-up) may reduce healthcare inequities. Incarcerated individuals, in particular, face systemic barriers to medical access, such as limited availability of correctional staff to accompany patients to off-site appointments.24,25 This challenge is reflected in the high “did not attend” rates among incarcerated individuals, which reach 43% for females and 48% for males—significantly higher than the 26% observed in the general population. 26 These findings suggest that PoCUS may serve as a practical tool to mitigate access-related delays in care.
Surgeon-performed PoCUS also demonstrated a meaningful impact on hospital resource utilization, particularly in reducing referrals to the DI department for ultrasound or MRI scans. In 96.8% of cases PoCUS negated the need for additional imaging, which would have otherwise been ordered had PoCUS not been available. This finding highlights its potential to streamline clinical workflows in the hospital setting. These findings are consistent with prior intensive care unit‐based studies showing that PoCUS can significantly reduce imaging burden, including chest radiographs, radiologist interpreted ultrasounds, and CT scans, with fewer imaging studies required across all modalities in the PoCUS group compared to controls (P < .01). 14 Our findings add to this growing body of evidence, illustrating that in plastic surgery settings, surgeon-performed PoCUS can similarly reduce reliance on formal DI resources.
By contrast, PoCUS facilitates a streamlined, single-provider model in which imaging is performed and interpreted in real time at the bedside. Prior studies in emergency and critical care settings have shown that this approach reduces healthcare costs and improves workflow efficiency14–16; our findings suggest these benefits may extend to surgical environments. To our knowledge, this is one of the first systematic evaluations of surgeon-performed PoCUS in plastic surgery. By demonstrating feasibility, efficiency, and access benefits in a specialty where adoption is still emerging, our study extends the evidence base beyond traditional medical contexts and highlights its unique value for surgical care.
Limitations
This study has several limitations. First, it was conducted at a single academic-community hospital with a relatively small sample size, which may limit generalizability. Additionally, while all scans were performed by ultrasound-trained staff plastic surgeons, their variability in PoCUS exposure may have influenced the diagnostic accuracy or decision-making following PoCUS assessments. In a small subset of cases, additional DI referral may have been avoidable with more advanced PoCUS proficiency, highlighting the importance of ongoing training and standardization in PoCUS use. Lastly, while this study demonstrates the potential for PoCUS to reduce imaging utilization and procedural burden, we did not perform a formal cost analysis; future studies should aim to quantify these economic impacts more precisely across diverse surgical settings.
Conclusions
This study demonstrates that surgeon-performed PoCUS is a versatile and effective tool within a plastic surgery department, with broad applications across patient demographics, anatomical regions, and clinical indications. PoCUS use was also associated with a reduced need for referral to DI for additional imaging in nearly all cases. Our findings suggest that PoCUS may support more efficient resource utilization by streamlining care pathways and reducing reliance on DI services. PoCUS represents a valuable adjunct in care with the potential to improve care delivery, expand access, and reduce costs. Future studies should aim to validate these findings in larger, multicenter cohorts and further explore the economic implications of PoCUS integration in surgical practice.
Footnotes
Author Contributions
Maleka Ramji contributed to the conceptualization of the study, the collection and analysis of data, and the drafting of the original manuscript, as well as revision and editing of the final manuscript. Veronica Pentland contributed to the analysis of the data, the drafting of the original manuscript, and the review and editing of the manuscript. Ryan E. Austin contributed to the conceptualization of the study, the collection of data, and the review and editing of the manuscript. Sophocles H. Voineskos contributed to the conceptualization of the study, the collection of data, and the review and editing of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval Statement
Approval for this study was obtained from the Unity Health Toronto Research Ethics Board for St. Joseph's Health Centre (study hospital site) and it was conducted in compliance with the Declaration of Helsinki for ethical research practices. (Ethics application number: REB 25-049).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided through the Wooster Family Surgical Innovation Award by the Department of Surgery at St. Joseph's Health Centre. This grant supported the purchase of the ultrasound device and related accessories.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Statement of Previous Study Presentations
Oral Presentation, Canadian Society of Plastic Surgery Annual General Meeting 2025.