
Abstract
Introduction
As mastectomy presently plays a major role in breast cancer treatment, breast reconstruction continues to be an option chosen by many women with the rates of breast reconstruction increasing in various countries around the world. 1 Breast reconstruction surgically attempts to restore the shape of the breast and provide aesthetically pleasing results. 2 To achieve this, there are many different procedures women can choose from with the benefit of each being dependent on individual circumstances, preferences of the patient and the surgeons’ skills. 3
Although breast reconstruction can have a positive impact in patients’ lives, it can also accomplish the opposite. 4 The concept of failure in breast reconstruction can occur when negative outcomes impact the patient experience. Critically important outcomes in breast reconstruction can vary from complications to symptoms to aesthetics. 5 Furthermore, failure extends to a negative experience that patients must live through the “reconstruction journey.” Synthesizing concepts of failure from patients’ perspectives can assist to establish congruency and clarity in navigating breast reconstruction.
There are numerous published qualitative studies detailing patients’ experiences after breast reconstruction ranging from qualitative research that solely focus on women's experience after procedural failure, such as flap loss, as well as studies that explore dissatisfaction after a procedure without complications. 6 These studies make important contributions to the breast reconstruction literature by providing a means for surgeons, researchers, policymakers, and future patients to better understand the patient experience. In addition, the literature encompasses a variety of breast reconstruction procedures from across the globe. 6 A synthesis of quotations that detail women's negative experiences with breast reconstruction can be extracted from these studies, allowing the development of a broad view of failure from patients of various backgrounds and breast reconstruction journeys.
To date, there are no reviews that summarize the results of existing studies on patient experiences of failure in breast reconstruction, highlighting the need for a synthesis of the literature in this area to identify common themes. Additionally, qualitative data, which provides critical importance in understanding patient experiences and perceptions, is increasingly incorporated in clinical decision-making. 7 In breast reconstruction, an improved understanding of patient perceptions of failure may inform the treatment options offered and clinicians’ approaches to discussions around reconstruction. Given the importance of qualitative research and its impact on clinical decision-making, there is a need to appraise the evidence quality to better discern how much confidence can be placed in study findings. 7
Thus, the primary objective of this systematic review was to identify experiences of failure from the patient's perspective following breast reconstruction in the existing qualitative literature. The secondary objective was to evaluate the reporting and methodological quality of the studies included.
Methods
Search Strategy
A systematic review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement 2020 (Supplemental 1). 8 The protocol was registered in PROSPERO (CRD42023451862). With the assistance of a medical librarian, a search of the following databases was undertaken: MEDLINE, Embase, Psychinfo, Emcare, and CINAHL on July 31, 2023 (from January 1, 2008) (Supplemental 2). Studies were included if they were: (1) available in English, (2) primary research studies, (3) qualitative research studies (ie, one-on-one interview or focus group) including mixed methods that separate qualitative results, (4) included patients who underwent breast reconstruction, and (5) had direct patient quotations describing negative experiences with breast reconstruction. This included both implant-based and autologous tissue as well as immediate and delayed reconstruction. Studies were excluded if they were (1) secondary research studies, (2) did not provide negative quotations from their participants, or (3) employed only quantitative methods (eg, Likert scale questionnaire data). An example of a study that appeared to meet criteria, but did not, was Shade et al. 9 Although it was a qualitative study on patients’ perceptions of breast reconstruction, it did not have quotations of patient's negative experiences after having the procedure as it focused on decision-making instead, and thus was excluded.
Study Selection
Studies identified in the database search were uploaded into Covidence. 10 Two reviewers (CH, AA) worked independently and in duplicate to first review title and abstracts for inclusion, followed by full-text screening using piloted extraction forms. Conflicts in the title, abstract, and full-text screening were resolved through discussion.
Data Extraction
Three reviewers (CH, AA, TB) worked independently and in duplicate for data extraction. The following data was extracted into Microsoft Excel: author, publication year, journal of publication, country, aim, type of breast reconstruction, population description, number of participants, study setting, study methodology and direct quotations reflecting patient's satisfaction and dissatisfaction with breast reconstruction. All conflicts were resolved by consensus.
Quality Assessment of Primary Qualitative Studies
Although there is no existing “gold standard” tool for quality assessment in qualitative research, 11 the Critical Appraisal Skills Programme (CASP) Qualitative checklist 12 and the Standards of Reporting for Qualitative Research (SRQR) checklist 13 were used to assess methodologic and reporting quality of included studies, respectively.
The methodological quality was determined with the CASP Qualitative Checklist. The CASP Qualitative Checklist is a 10-item checklist, 12 which is commonly used in qualitative synthesis studies. 14 To answer the question posed in each item, reviewers chose from three options: “Yes,” “Can’t Tell,” or “No” and wrote comments explaining the choice. Three reviewers (CH, AA, TB) worked independently and in duplicate to provide a CASP qualitative checklist for each study. All conflicts were settled by consensus.
The reporting quality of individual studies were determined according to the Standards of Reporting for Qualitative Research (SRQR). The SRQR is a 21-item checklist for complete, transparent reporting of qualitative research. 13 For each item, studies were given a 1 if they met the criteria and a 0 if they did not. Scores were summed with a maximum score of 21 points. SRQR scores for the included studies were obtained from a previously published systematic review on qualitative studies in breast plastic surgery by the study's lead author. 6 If a study's SRQR score was not previously reported, two reviewers (CH, TB) worked independently and in duplicate to provide a SRQR score. All conflicts were settled by consensus.
Data Synthesis and Analysis
Qualitative synthesis is any methodology where qualitative study findings are pooled and systematically interpreted through a series of expert judgements to draw conclusions on the meaning of the collected work. 15 Thematic analysis is a type of qualitative synthesis methodology, which aims to develop themes that represent ways of understanding the combined meaning of the text. 15 Thematic analysis was chosen for this study as this method is useful for summarising the collective conclusions of included studies. 15 Specifically, a form of thematic analysis, described as thematic synthesis by Thomas and Harden was done. 16 Thematic synthesis involves three stages: (1) free line-by-line coding, (2) organization of “free codes” into related areas to construct “descriptive” themes, and (3) development of “analytical” themes. 16 Triangulation was performed to add rigour to the analysis process. 15 Two reviewers (CH, AA) independently performed each step. Codes or themes were discussed at each stage. Discrepancies in themes among the authors were discussed until an agreement was achieved.
The Confidence in the Evidence from Reviews of Qualitative research (CERQual) was used to assess confidence in the final findings. 17 The CERQual defines “confidence” as an evaluation of the degree to which a study's results logically and reasonably represent a given topic of question, whereby a study with a high confidence is one in which readers can place higher trust in its findings. 17 “Confidence” is determined based on assessment of four components: methodologic limitations, coherence, adequacy of data, and relevance. 17
Results
Study Selection
As depicted in the PRISMA flow diagram (Figure 1), 3289 studies were identified from the search and 42 studies were included in the final analysis. Study characteristics are summarized in Supplemental 3.
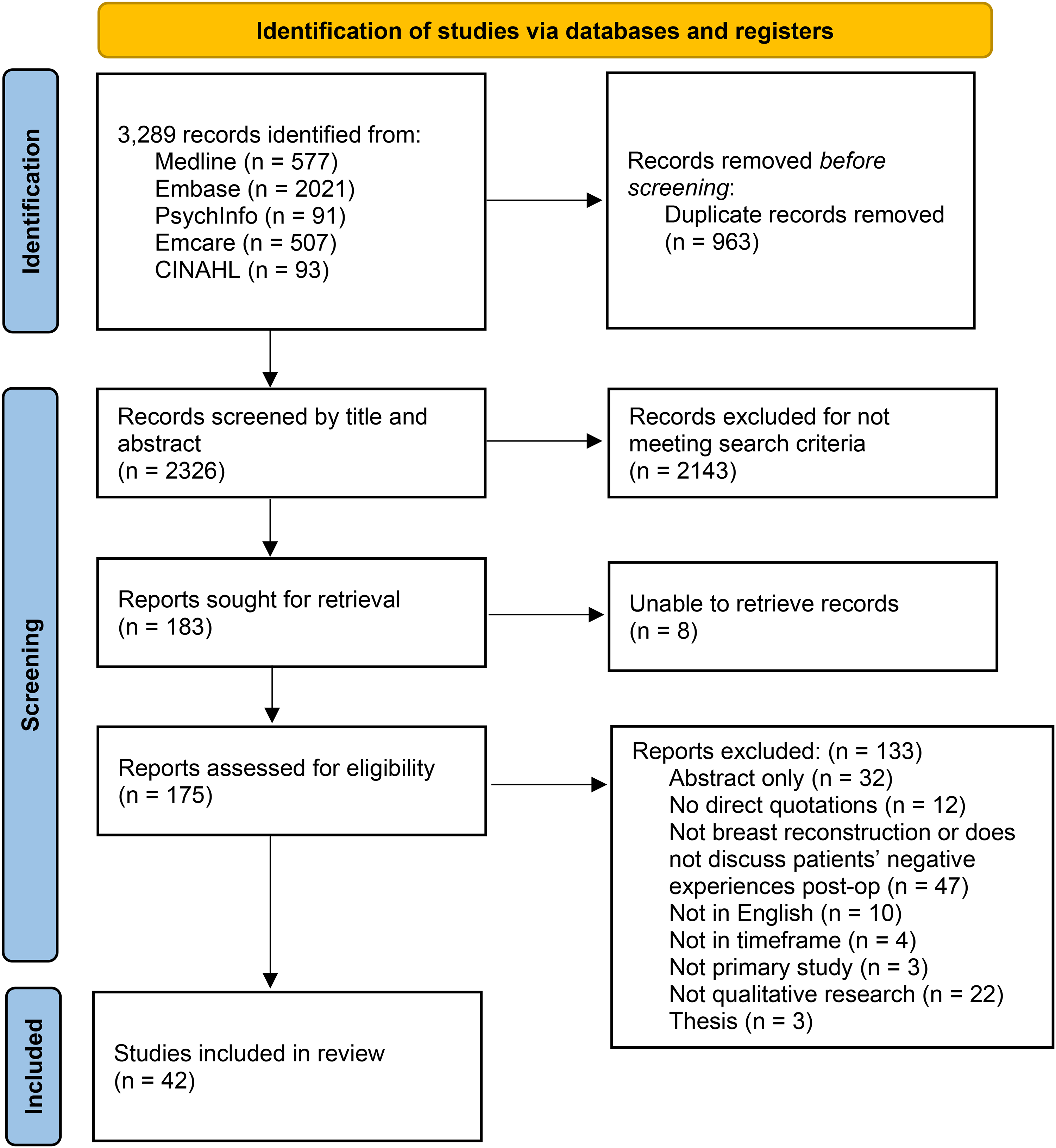
A figure of the PRISMA 2020 flow diagram.
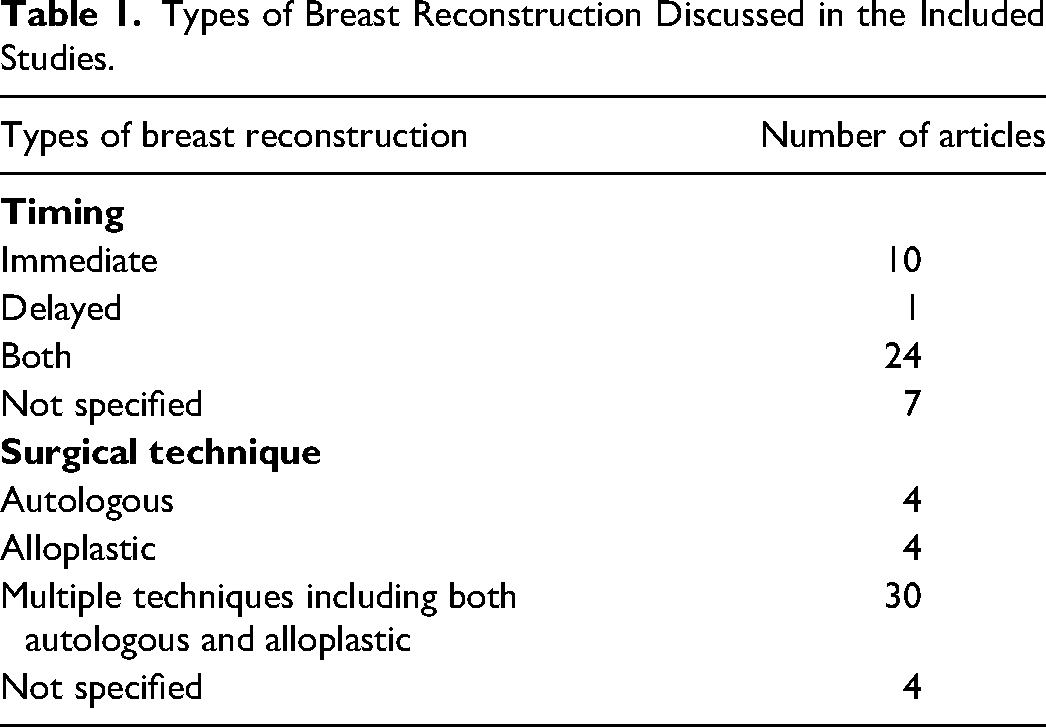
Studies took place in Australia (n = 2), Brazil (n = 1), Canada (n = 8), Egypt (n = 1), Germany (n = 1), Israel (n = 2), Korea (n = 1), Netherlands (n = 5), Sweden (n = 2), Taiwan (n = 1), UK (n = 10), and the USA (n = 10). For breast reconstruction timing, 10 studies described immediate, 1 study described delayed, 24 studies described both, and 7 did not specify. The majority of studies (n = 30) had multiple techniques for breast reconstruction including both autologous, alloplastic, or a combination of both. Four studies each looked at autologous, alloplastic, or did not specify the type of reconstruction (Table 1).
Types of Breast Reconstruction Discussed in the Included Studies.
From thematic analysis of the studies, the following four themes were identified: (1) failure occurs when expectations of restoring the original breast are not met with reconstruction; (2) failure occurs when unexpected outcomes were associated with the reconstruction; and (3) failure occurs when healthcare providers aggravated the experience of breast reconstruction through poor pre-operative patient education on expected outcomes (Table 2).
Themes With an Illustrative Quotation and Contributing Studies for Their Sub-Themes.
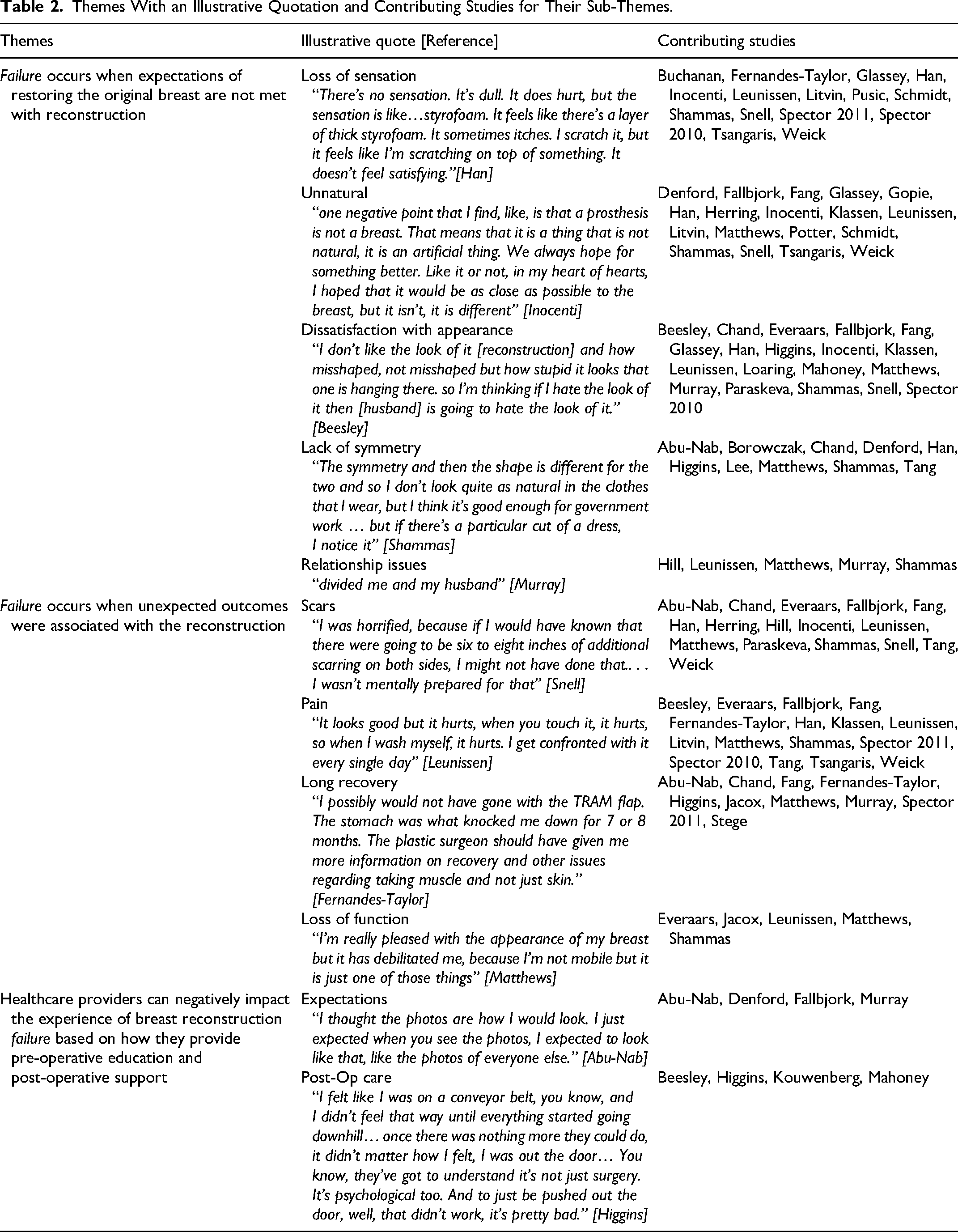
Theme 1: Failure Occurs When Expectations of Restoring the Original Breast are not Met With Reconstruction
Breast reconstruction can never fully return the breast that was lost to mastectomy. When features of the original breast are missed by a patient, this can foster dissatisfaction in their reconstruction. The loss of sensation was a repeated theme within the literature.18–32 Unlike their original breast, patients felt that the lack of feeling in the reconstructed breast was difficult to adjust to and made the reconstructed breast feel unnatural. This concept of the reconstructed breasts being unnatural was also observed.21–28,31–40 The differences in the reconstructed breast's shape, feel, and appearance from their original breast made it seem abnormal in comparison.
Dissatisfaction with appearance was a common theme.21–24,27,28,30,34,35,38,39,41–48 This included being unhappy about the final results of the breasts but also of the abdomen for those that underwent DIEP/SIEA/TRAM flaps. A lack of symmetry also contributed to this dissatisfaction.22,27,33,39,42,44,49–52 Women found the difference between the reconstructed breast and original breast on the other side to be unpleasant. They also noted changes to the symmetry of the breasts with time or after radiation.
Some studies found the loss of the breasts to introduce relational challenges that reconstruction could not solve.24,27,39,47,53 Women described preventing their partners from seeing or touching their reconstructed breasts because of their own discomfort with them. Additionally, the loss of the nipples impacted their sexual pleasure.
Theme 2: Failure Occurs When Unexpected Outcomes Were Associated With the Reconstruction
The risks associated with reconstructive surgery were found to create a negative experience for some women. In particular, scarring was frequently mentioned within the literature.22–24,27,28,32,34,35,37,39,42,43,48,49,52,53 Patients were unpleasantly surprised when there were longer or more scars than expected. They reported finding it difficult to cover up scars or to look at the scars when they were naked. Some scars even caused pain.
Pain in and of itself was another unexpected adverse outcome of breast reconstructive surgery.20,22,24,25,27,29–32,34,35,38,39,41,43,52 For some women, the pain became a chronic issue to the point of regret for having the operation. They also expressed surprise when the donor site was more painful than the reconstructed breasts in autologous reconstruction. The pain post-procedure introduced a long recovery period, which was another theme identified.20,29,35,39,42,44,47,49,54,55 There were instances of women being unprepared for the length of time to recover, having taken a longer time than what they expected.
Lastly, loss of function following breast reconstruction was also reported in the literature.24,27,39,43,54 The inability to move or do certain tasks as before was seen as limiting and potentially distressing.
Theme 3: Healthcare Providers can Negatively Impact the Experience of Breast Reconstruction Failure Based on How They Provide Pre-Operative Education and Post-Operative Support
Although experiences of losing a breast and living with adverse outcomes of reconstructive surgery are individualized to a patient, healthcare providers also play a role in aggravating the concept of failure. The idea of results not matching patient's expectations was identified in the literature.33,34,47,49 Some women saw pictures of reconstructed breasts but were met with disappointment when their results did not resemble those photos. There was a mismatch between the expectations going into the surgery and the results they came out with. There were also many reports of women feeling unsupported with their post-operative care.41,44,46,56 This manifested as poor communication with their doctor when unsatisfied with the results. Women reported a lack of relational support when experiencing complications in particular, and at times felt like they were treated as a problem more than a person.
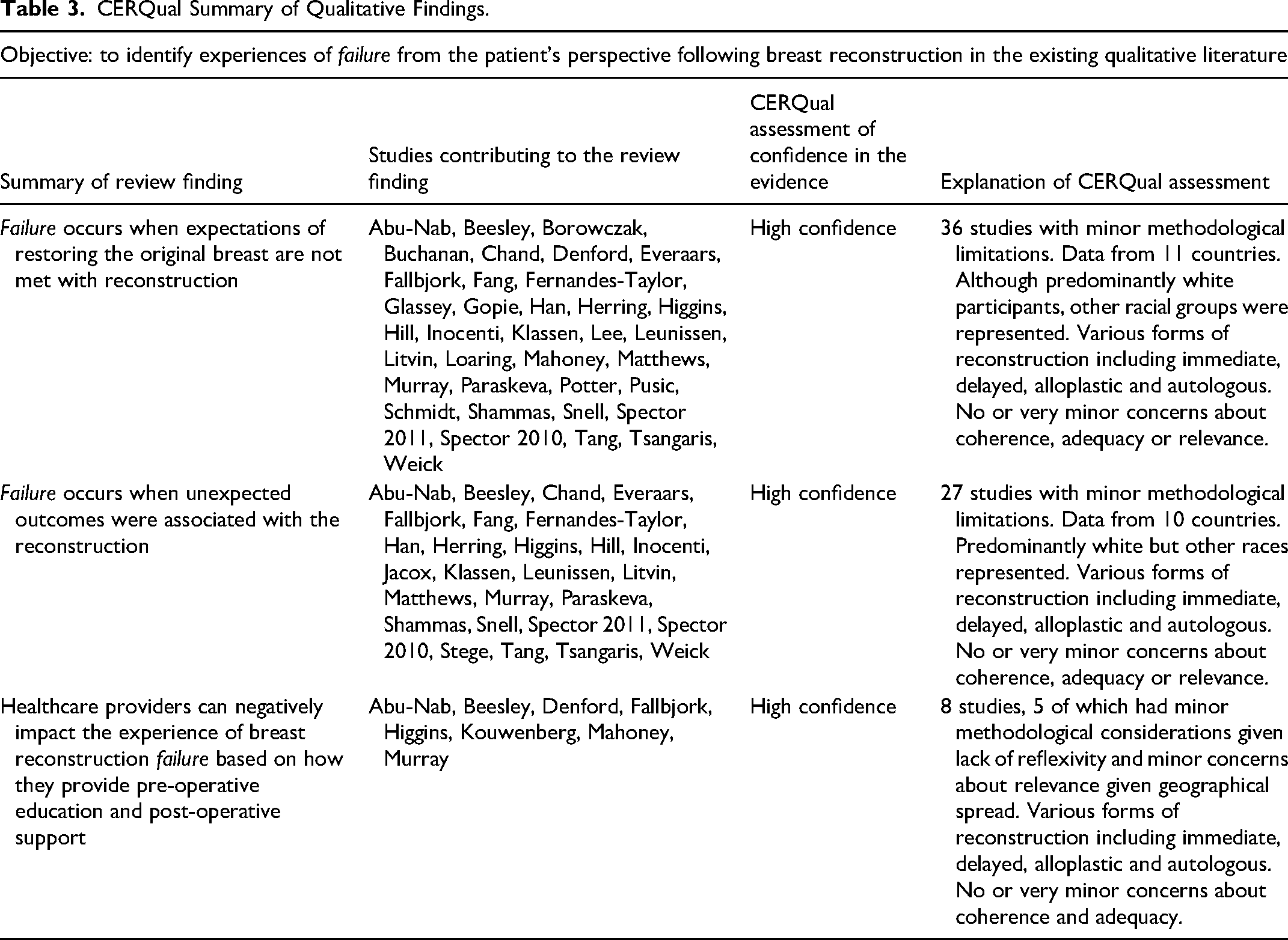
CERQual Assessment
Themes 1-3 obtained high confidence in CERQual assessment (Table 3, Supplemental 4).
CERQual Summary of Qualitative Findings.
Reporting and Methodological Analysis
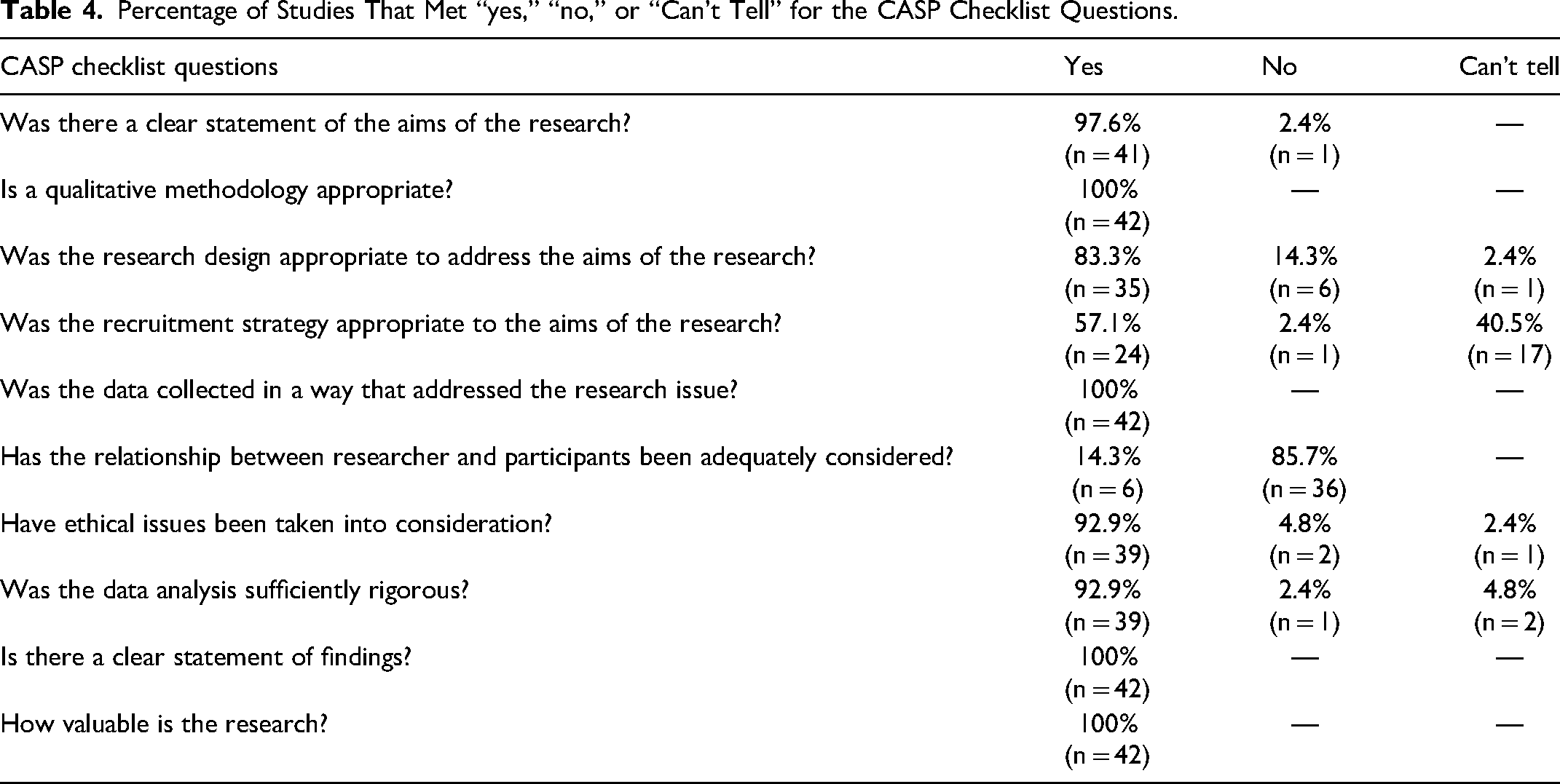
The median SRQR score was 16 out of 21 (min: 10, max: 21) of the 42 papers included. A majority of the studies scored “yes” on 8 out of 10 of the CASP questions (Table 4). For the question “has the relationship between research and participants been adequately considered?,” the majority of studies (85.7%) scored a “no.” Additionally, a large portion (40.5%) scored a “can’t tell” for “was the recruitment strategy appropriate to the aims of the research?” (Supplemental 5).
Percentage of Studies That Met “yes,” “no,” or “Can’t Tell” for the CASP Checklist Questions.
Discussion
To our knowledge, this is the first systematic review to summarize qualitative findings on patients’ experiences with failure following breast reconstruction. Although failure of breast reconstruction can be an individualized concept based on a patient's circumstances, this review sought to identify concepts of failure from patient experiences encompassing a variety of breast reconstruction techniques. Thus, concepts of failure identified in this review can broadly be applied to improve patients’ experience with breast reconstruction despite the diversity in the field. Breast reconstruction surgeons with long clinical experience may have surmised these concepts of failure already. This qualitative review sought to confirm these concepts from direct patient quotations.
One overarching theme identified—that patients felt their reconstructed breast did not fully replace their original breast—supports findings from a cross-sectional study by Siquiera et al that utilized a questionnaire to assess the quality of life in women who had breast reconstruction or no reconstruction following mastectomy. They report that overall satisfaction with the operation had a greater impact on quality of life than whether the operation included reconstruction or not. 57 If the reconstructed breast is seen as “unnatural” through appearance or sensation, it can create dissatisfaction. Furthermore, if the reconstructed breasts are associated with unwanted scars, pain, and loss of function, this can also cause distress to patients. These potential challenges faced by women who have undergone breast reconstruction may explain why previous studies have found poorer or equal quality of life outcomes in patients with reconstructed breasts compared to patients in a non-reconstructed cohort.57,58
An additional theme across studies was that negative interactions with the healthcare team played a role in aggravating breast reconstruction failure. Patient-centred communication has been previously discussed in the context of breast surgery as a method to strengthen the patient–physician relationship and enhance patient satisfaction. 59 As such, a positive relationship between patients and physicians can lead to satisfaction in the overall breast reconstruction. 59 Pusic et al have developed the Expectations for Reconstruction Module within the BREAST-Q to measure patient expectations for reconstruction, 18 specifically surrounding expected appearance and symmetry of reconstructed breasts relative to their original breasts. The use of this module allows plastic surgeons to obtain a comprehensive assessment of their patients’ expectations, while providing the opportunity to discuss and counsel patients on these expectations prior to surgery.
The results of this study serve as a compilation of failure seen in breast reconstruction qualitative literature. This was achieved by collecting patient quotations of negative comments. As such, this review was unable to determine if these themes led to regret or were pitfalls in an overall positive experience. Additionally, as this review only searched for concepts of failure, any positive or mundane experiences were not extracted. Thus, this review cannot claim that the themes identified produce negative experiences for all women who undergo breast reconstruction, although the themes were repeated in various studies with different cohorts of patients. Nevertheless, as plastic surgeons’ responses to negative reactions were identified to be a theme in and of itself, it is important to analyze these experiences to better inform patient care.
Across the majority of included studies, one recurrent methodological flaw was the lack of reflexivity among researchers as 85.7% of the papers scored a “no” for the CASP question “has the relationship between research and participants been adequately considered?.” Reflexivity allows qualitative researchers to examine their biases as well as relationships with the participants to determine influences to their data. 13 To counteract potential bias from a lack of reflexivity, this review only assessed direct quotations from participants instead of the researchers’ interpretations of it. Although quotations included in papers can be compromised by author bias, this study included qualitative research with different objectives than its own to minimize selection bias.
Although this study included qualitative research from many different countries, the majority of papers had mainly Caucasian participants. Connors et al and Shade et al highlight the unique experiences of African American and First Nations women, respectively, with breast reconstruction and found marginalized populations experience distinct challenges affecting their perceptions of and willingness to undergo the procedure.9,60 Cultural sensitivity in patient–physician conversations about breast reconstruction options are emphasized in these studies.9,60 The lack of inclusion of more marginalized patient experiences with breast reconstruction failure in this review serves as a limitation.
Another limitation is that the CASP tool is not validated. Hannes et al have previously described its shortcomings when measuring validity and generalizability compared to other appraisal instruments. 61 Yet, the CASP has been utilized in other qualitative synthesis and was chosen for this study on that basis. 14
Conclusion
This is the first systematic review of qualitative research that investigated patients’ concepts of failure in breast reconstruction. Breast reconstruction failure encompasses both the inherent constraints and undesirable results of the surgical process, even when the procedure was successful from the surgeon's point of view. This dissatisfaction is increased by procedural complications. As well, healthcare providers can play a role in mitigating this failure. Incorporating these perceptions of failure into discussions with patients can aid in their decision making.
Supplemental Material
sj-docx-1-psg-10.1177_22925503241311255 - Supplemental material for Patient Perspectives of “Failure” in Breast Reconstruction: A Systematic Review of Qualitative Literature
Supplemental material, sj-docx-1-psg-10.1177_22925503241311255 for Patient Perspectives of “Failure” in Breast Reconstruction: A Systematic Review of Qualitative Literature by Caroline Hircock, Patrick Kim, Abhishek Achunair, Tara Behroozian, Lucas Gallo, Emily Dunn and Achilles Thoma in Plastic Surgery
Supplemental Material
sj-docx-2-psg-10.1177_22925503241311255 - Supplemental material for Patient Perspectives of “Failure” in Breast Reconstruction: A Systematic Review of Qualitative Literature
Supplemental material, sj-docx-2-psg-10.1177_22925503241311255 for Patient Perspectives of “Failure” in Breast Reconstruction: A Systematic Review of Qualitative Literature by Caroline Hircock, Patrick Kim, Abhishek Achunair, Tara Behroozian, Lucas Gallo, Emily Dunn and Achilles Thoma in Plastic Surgery
Supplemental Material
sj-docx-3-psg-10.1177_22925503241311255 - Supplemental material for Patient Perspectives of “Failure” in Breast Reconstruction: A Systematic Review of Qualitative Literature
Supplemental material, sj-docx-3-psg-10.1177_22925503241311255 for Patient Perspectives of “Failure” in Breast Reconstruction: A Systematic Review of Qualitative Literature by Caroline Hircock, Patrick Kim, Abhishek Achunair, Tara Behroozian, Lucas Gallo, Emily Dunn and Achilles Thoma in Plastic Surgery
Supplemental Material
sj-docx-4-psg-10.1177_22925503241311255 - Supplemental material for Patient Perspectives of “Failure” in Breast Reconstruction: A Systematic Review of Qualitative Literature
Supplemental material, sj-docx-4-psg-10.1177_22925503241311255 for Patient Perspectives of “Failure” in Breast Reconstruction: A Systematic Review of Qualitative Literature by Caroline Hircock, Patrick Kim, Abhishek Achunair, Tara Behroozian, Lucas Gallo, Emily Dunn and Achilles Thoma in Plastic Surgery
Supplemental Material
sj-docx-5-psg-10.1177_22925503241311255 - Supplemental material for Patient Perspectives of “Failure” in Breast Reconstruction: A Systematic Review of Qualitative Literature
Supplemental material, sj-docx-5-psg-10.1177_22925503241311255 for Patient Perspectives of “Failure” in Breast Reconstruction: A Systematic Review of Qualitative Literature by Caroline Hircock, Patrick Kim, Abhishek Achunair, Tara Behroozian, Lucas Gallo, Emily Dunn and Achilles Thoma in Plastic Surgery
Footnotes
Author Contributions
AT, CH: conceived and directed the study; CH, AA: title and abstract screening; CH, AA, TB: data extraction; CH, PK, AA, TB, LG, ED, AT: contributed to the study design and interpretation of the results; CH, AA, PK, TB, LG: analyzed the data; CH, AA, PK, TB, LG, ED: contributed to the statistical analysis and reporting of the data; CH, PK, AA, TB, LG, ED, AT: contributed to the manuscript preparation.
Data Availability
All data generated or analyzed during this study are included in this published article (and its supplemental information files).
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Thoma is an editor of the book Evidence-Based Surgery: A Guide for Understanding and Interpreting the Surgical Literature and receives royalties from SPRINGER. The other authors have no conflict of interest to report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
This article does not contain any studies with human or animal subjects.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.