
Abstract
Introduction
Given the aging population, ∼10%–15% of patients with atrial fibrillation and on long-term anticoagulant therapy require elective surgery at some point. 1 Within 2 subdomains of plastic surgery, namely oculoplastics and dermatologic surgery, 25%–40% of patients are already on prescription antithrombotic medications for cardiovascular comorbidities, such as atrial fibrillation, mechanical heart valves, and prior venous thromboembolic events.2,3 Antithrombotic medications include vitamin K antagonists, direct oral anticoagulants (DOACs), and antiplatelet medications; while these medications are essential in reducing mortality and morbidity in those at risk of thromboembolism, they are associated with increased bleeding risk when taken in the perioperative period. 4 As such, plastic surgeons must weigh the risk of systemic complication due to antithrombotic medication interruption against the risk of procedural bleeding if antithrombotic medications are continued.
The perioperative management of antithrombotic therapies in patients undergoing plastic and reconstructive surgery remains a common clinical challenge for clinicians, with few published clinical trials available to address this issue.5–10 Excessive bleeding in plastic surgery is associated with complications, such as prolonged operative time, hematoma, ecchymosis, impaired flap survival, skin graft loss, scarring, poor cosmesis, poor functional outcomes, and visits to the emergency department.11–15 Impaired flap survival may necessitate a return to the operating room and need for transfusion in severe cases.6,11,12,13 These complications should be minimized wherever possible, and it is the responsibility of the treating plastic surgeon to ensure that the perioperative management of antithrombotic agents is done appropriately.
The decision to continue or interrupt antithrombotic therapies is currently made at the discretion of the treating physician, with 84% of plastic surgeons reporting that their clinical decisions are made based on personal preference. 16 The paucity of guideline recommendations within plastic surgery has led to significant heterogeneity across clinical practice.17,18 As such, a single clinical practice approach that summarizes recommendations on perioperative antithrombotic medication specific to plastic surgery is warranted to facilitate and standardize clinical decision-making. In this paper, we summarize the current American College of Chest Physicians (ACCP) guideline recommendations and present them in a more “digestible” way for plastic surgeons to implement, thus standardizing their current practice. Three clinical scenarios that are commonly faced by plastic surgeons are presented, with a 3-step approach to their perioperative management.
Clinical Scenario 1
A 70-year-old woman with a past medical history of stroke (5 years ago), type 2 diabetes mellitus, peripheral artery disease, and a coronary artery stent (12 months ago), currently on warfarin, presents to you, a plastic surgeon, with severe carpal tunnel syndrome. Carpal tunnel release is recommended.
Clinical Scenario 2
A 54-year-old woman with a past medical history of atrial fibrillation, a bi-leaflet aortic valve replacement (6 months ago), and breast cancer, currently on clopidogrel, is being considered by her surgical oncologist for right-sided mastectomy and you are asked to perform immediate breast reconstruction with a deep inferior epigastric artery perforator flap.
Clinical Scenario 3
A 74-year-old man with a past medical history of atrial fibrillation, myocardial infarction (8 months ago), and chronic kidney disease, currently on dabigatran, is referred to you by his dermatologist for surgical excision of a 7 × 5 mm biopsy-proven squamous cell carcinoma on the left alar crease of his nose.
Given the thromboembolic and bleeding risk in all 3 patients:
Should surgery be performed while each patient remains on their antithrombotic therapy? Under what circumstances should their antithrombotic therapies be stopped perioperatively? If surgery is necessary but anticoagulation cannot be stopped, how should the plastic surgeon proceed? What are the indications to consult a cardiologist or hematologist when faced with a patient on antithrombotic therapies?
Current Available Guidelines
Several guidelines have been published in recent years to guide surgeons across all disciplines on the appropriate perioperative management of patients who are prescribed antithrombotic therapies.19–22 Among the available guidelines, the recommendations put forth by the ACCP (2022)4,23 remain the most frequently used in the field and are commonly referred to by cardiologists and hematologists. Three guidelines have been identified that provide recommendations in specific domains within plastic surgery, namely in cutaneous, 24 hand and wrist, 25 and craniofacial surgeries. 26
To present a convenient clinical practice approach for use by plastic surgeons, recommendations were adapted primarily from the ACCP guidelines, 4 with supplementation from guidelines within plastic surgery domains.24–26 This was done in collaboration with a member of the ACCP clinical practice guideline panel (JD).
Clinical Practice Conceptual Framework
Step 1: Assessment of Procedural Bleeding Risk
Currently, there is no established consensus on the stratification of bleeding risk among plastic surgery procedures. As per the International Society on Thrombosis and Hemostasis (ISTH) recommendations, Douketis et al 4 stratified procedural bleeding risk across surgical disciplines into “high,” “low–moderate,” and “low” risk based on their 30-day risk of a major bleed. A plastic surgery-specific bleeding risk stratification was adopted based on these categories (Figure 1).
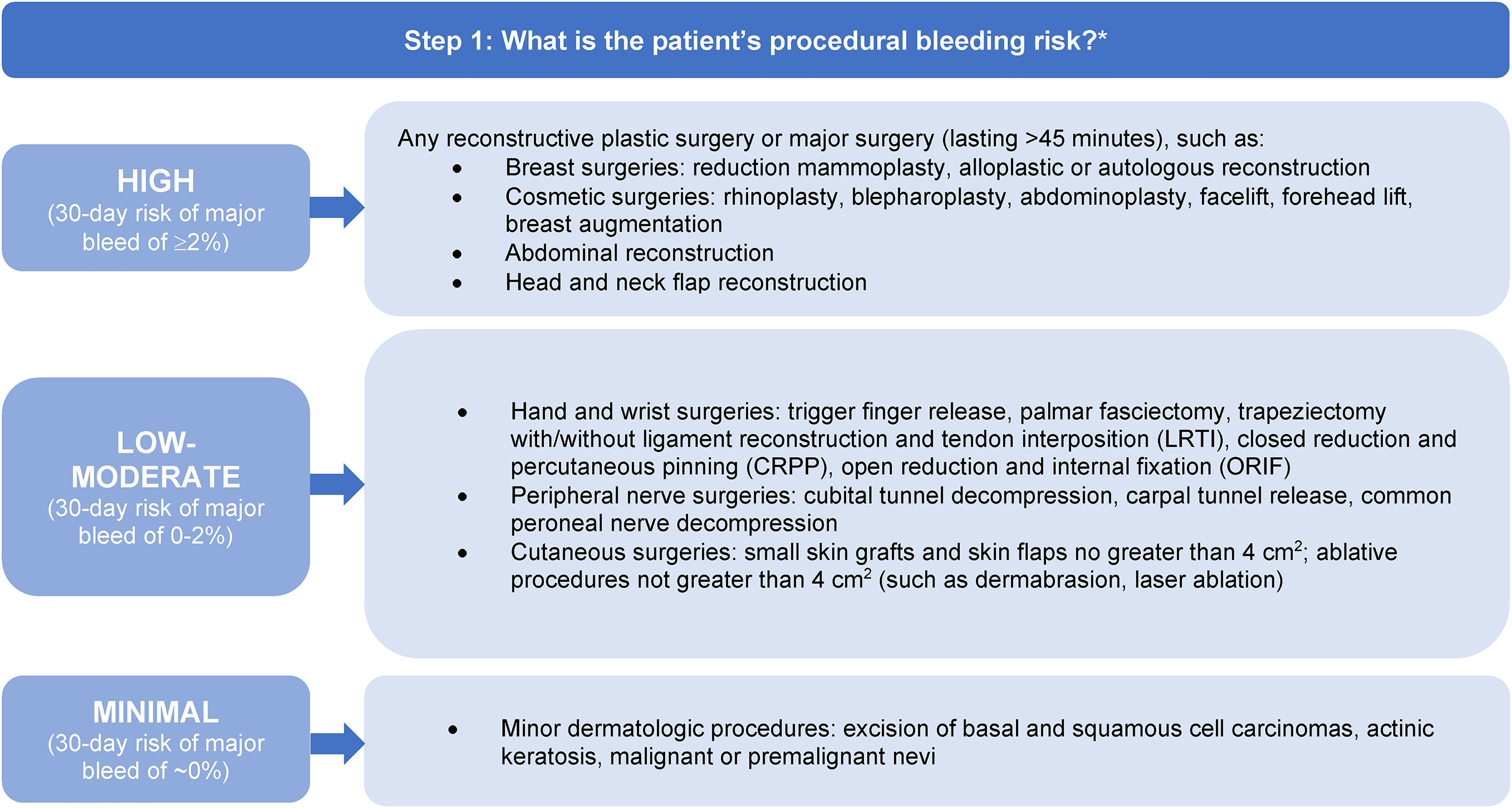
Identifying the patient's procedural bleeding risk. *Adapted from the 2022 ACCP guidelines with supplementation from the 2021 S3 guidelines on cutaneous surgery.
A retrospective study by Thomas et al 27 of 95,687 patients undergoing plastic surgery revealed increased bleeding complications in patients undergoing breast reconstruction with a free flap and breast reconstruction with a pedicled transverse rectus abdominis musculocutaneous flap. Other procedures associated with an increased frequency of blood transfusion, return to the operating room, and 30-day mortality included the following: any other procedures involving flaps and grafts; wound debridement; drainage of a hematoma, seroma, or fluid collection; excision of excess skin or subcutaneous tissue; mastopexy; and any other reconstructive procedures. Many additional procedures were included in this analysis to assess complication rates. Additional factors predictive of a higher incidence of hematoma development include combined procedures, breast procedures, procedures performed in the hospital rather than in the office, increasing patient age, and male sex. 28 The treating surgeon may consider these prognostic factors when assessing patient-specific bleeding risk.
Step 2: Assessment of Patient Thromboembolic Risk
Once the plastic surgeon has defined the procedural bleeding risk, they may proceed to determine the patient's thromboembolic risk using the ISTH stratification, which has been described in the existing literature and cited in guidelines across disciplines (Figure 2). 4 A patient's individual thromboembolic risk may be designated as “high,” “moderate,” or “low” based on their past medical history of a mechanical heart valve, atrial fibrillation (using the CHA₂DS₂-VASc score), and/or venous thromboembolism.
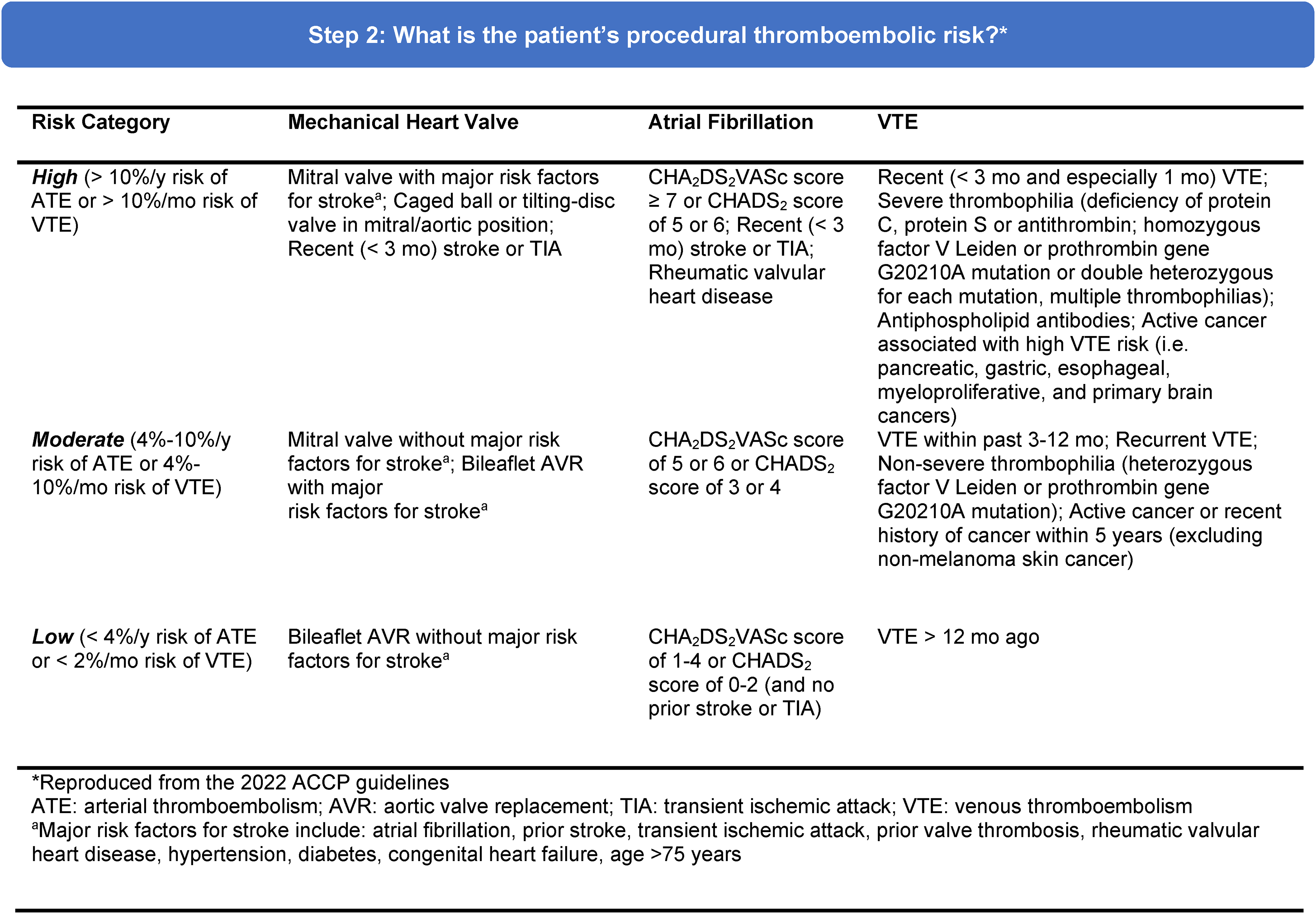
Identifying the patient's thromboembolic risk. Adapted from Douketis et al. 4
Step 3: Clinical Decision-Making Based on Antithrombotic Medication Type
Appropriate decision-making steps on whether to continue, interrupt, or bridge the patient's antithrombotic medication are outlined in Figure 3. Recommendations are made based on (1) the type of antithrombotic agent prescribed and (2) the procedural bleeding risk, with additional considerations based on patient thrombotic risk. The mechanisms of action of these antithrombotic agents are beyond the scope of this article. For those interested, this information has been previously summarized. 29
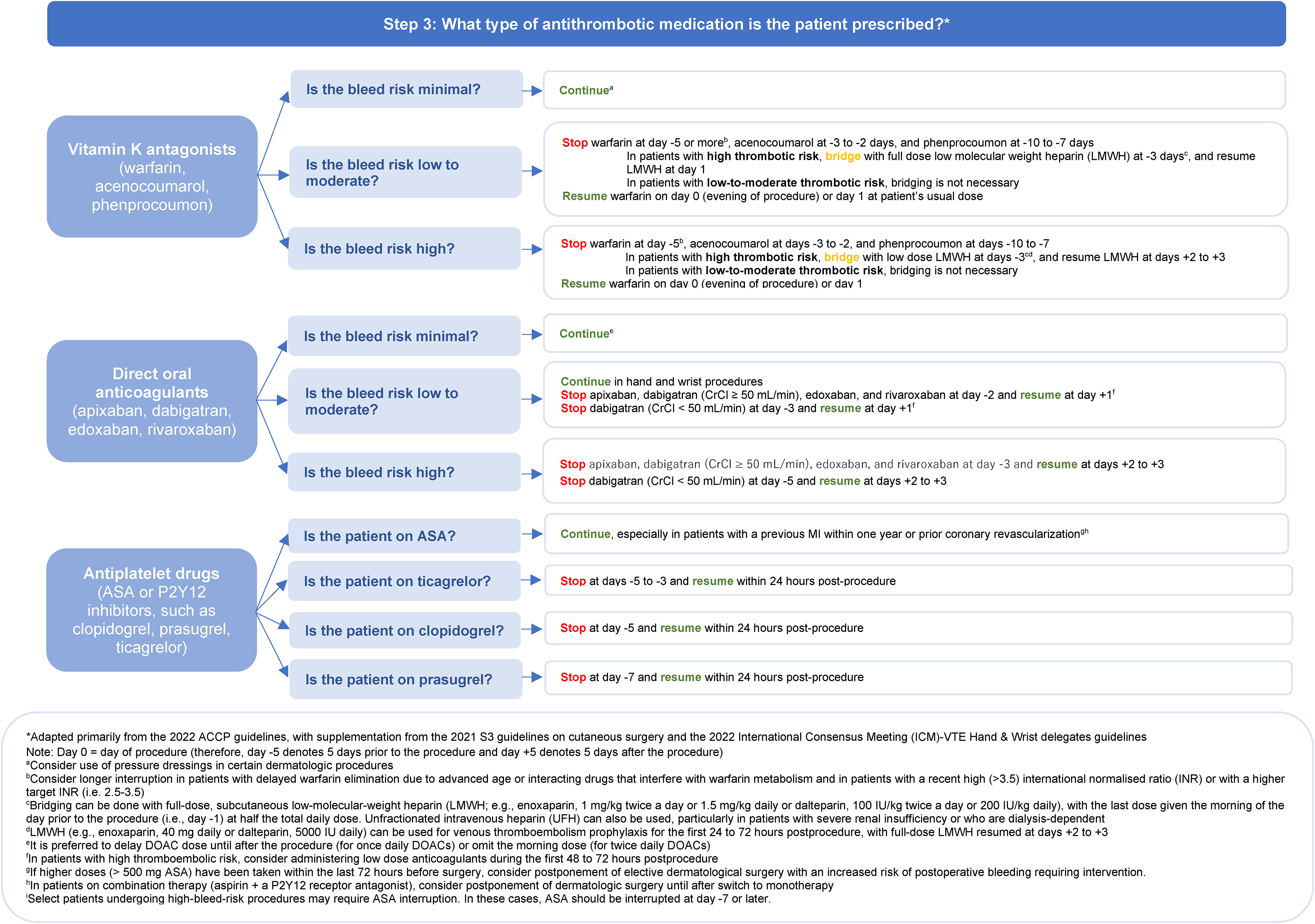
Clinical decision-making guide based on type of antithrombotic medication. Adapted from Douketis et al. 4
Case Resolution
By following the clinical practice approach outlined, one can determine the appropriate measures for a plastic surgeon to take in the case of clinical Scenario 1, which requires surgical carpal tunnel release. As per Step 1, her procedural bleeding risk is low to moderate, indicating a 30-day risk of major bleeding of 0%–2%. Based on her past medical history, her CHA2DS2VASc score is 7, which places her in the high category for thromboembolic risk. As she is currently on warfarin, the recommendation is to discontinue her warfarin at 5 days preoperatively, followed by bridging with low-molecular-weight heparin (LMWH) at 3 days preoperatively and resuming at day 1 postoperatively. Warfarin can be resumed at day 0 postoperatively. If she had been on prasugrel, for example, the medication would have to be stopped 7 days preoperatively, with a resumption in the first 24 h postoperatively. If this patient had been on a DOAC, she may have been able to continue her medication (if she had been on apixaban, for example).
In Clinical Scenario 2, since the patient is considering undergoing a lengthy and invasive reconstructive surgery for right-sided breast reconstruction, she is in the high-risk category for procedural bleeding. Her medical history of a bi-leaflet aortic valve replacement, atrial fibrillation, and active breast cancer, places her in the moderate category for thromboembolism risk. Regardless of her thromboembolism and procedural bleed risk, the conceptual framework advises the interruption of clopidogrel at 5 days preoperatively, with resumption in the first 24 h postoperatively. If she had been on warfarin, it would be stopped 5 days preoperatively without necessitating bridging with LMWH; warfarin would be resumed at day 0 postoperatively. If she had been on rivaroxaban, for example, rivaroxaban would have been interrupted 3 days prior and resumed at days 2 to 3 postoperatively.
While minor cutaneous surgeries are normally considered to have a minimal bleeding risk, Clinical Scenario 3 would fall under the low–moderate risk category of procedural bleed risk as per the S3 Cutaneous Surgery clinical practice guidelines 24 ; this is because the excision would involve the nose, an area well vascularized. With a CHA2DS2VASc score of 2 given the patient's past medical history of atrial fibrillation and myocardial infarction, he is at a low risk of thromboembolism. As per the clinical practice conceptual framework, perioperative management of his dabigatran can be decided based on his creatinine clearance (CrCl). If his CrCl exceeds 50 mL/min, the dabigatran should be discontinued 2 days prior to surgery and resumed 1 day postoperatively. If his CrCl were below 50 mL/min due to advanced chronic kidney disease, the dabigatran should be discontinued 3 days prior to surgery instead of 2 days. If he had been taking acenocoumarol, for example, this would have been stopped at 2 to 3 days preoperatively without necessitating bridging with LMWH given his thromboembolic risk. If he had been taking acetylsalicylic acid, for example, this would have been continued without interruption.
Conclusions and Areas for Future Research
The present clinical practice conceptual framework may be implemented in clinical practice to guide plastic surgeons on the appropriate perioperative management of patients who are prescribed antithrombotic medications, while reducing the number of referrals made to the thrombosis service. A plastic surgery-specific clinical practice guideline addressing this topic is certainly lacking; however, the development of a specific guideline within plastics may potentially duplicate the extensive efforts that have been made by established groups, such as the ACCP, to answer these questions in all areas of surgery. While we acknowledge that the ACCP recommendations presented here have been previously reported and are not novel, we aimed to enhance the preexisting guidelines by making them more applicable to plastic surgery.
Future efforts should be made to allow plastic surgeons to more confidently use the existing guidelines. In particular, there is no established consensus on the procedural bleed risk stratification in plastic surgery. As such, plastic surgeons should exercise caution when adapting the ACCP guidelines to their own clinical practice. For example, all hand procedures were combined under a “mild-moderate” risk category for procedural bleeding. However, the bleed risk across different types of hand and wrist procedures is heterogeneous, and it may not be clinically appropriate to use the same perioperative approach to management across all of these procedures. A Delphi consensus may therefore be conducted to clarify which common procedures within plastic surgery fall under the “high,” “low–moderate,” and “minimal” bleed risk categories. Alternatively, data from previously published studies on bleeding complications associated with procedures in plastic surgery may also be used to classify procedures into different bleeding risk categories. 27
Clinical Disclaimer and Special Circumstances
The proposed 3-step approach provides plastic surgeons with a simplified overview of the perioperative management of patients on antithrombotic agents. The complete ACCP guidelines should therefore be consulted as needed for detailed recommendations as many of the individual recommendations are accompanied by patient-specific considerations. A hematologist, cardiologist, and/or thrombosis service should be considered in high-risk patients (Box 1). The management of patients undergoing nonelective procedures is beyond the scope of this conceptual framework. Ultimately, decisions should be made at the plastic surgeon's discretion, who must determine whether the proposed recommendations can be safely applied to their patient population with support from experienced colleagues when they are unsure. This prudence when making clinical decisions will ensure that the plastic surgeon has taken the appropriate medico-legal precautions to minimize unintended outcomes.
Indications for consultation with a hematologist or cardiologist. 4
Patients with poorly controlled cardiac disease or recent unstable coronary symptoms. Patients taking dual antiplatelet therapy (aspirin and one of: clopidogrel, ticagrelor, or prasugrel). Patients who have had a prior venous or arterial thromboembolic event around the time of a surgery or procedure. Patients with a drug-eluting stent implanted within the past 2 years. Patients with a mechanical heart valve prosthesis. Patients on a DOAC or warfarin with venous thromboembolism within the past 12 months. Patients on a DOAC or warfarin with a stroke within the past 12 months.
Footnotes
Author Contributions
TB: conceptualization, methodology, and writing—original draft preparation; EF: conceptualization, methodology, and writing—original draft preparation, HR: conceptualization, methodology, and writing—reviewing and editing; JD: methodology and writing—reviewing and editing; AT: supervision, conceptualization, methodology, and writing—reviewing and editing.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Achilles Thoma is an editor of the book Evidence-Based Surgery: A Guide for Understanding and Interpreting the Surgical Literature and receives royalties from Springer. All other authors have no potential conflicts of interest to declare.
Ethical Statement
This article does not contain any studies with human or animal subjects.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.