
Abstract
Introduction
Adolescent gynecomastia is typically a benign condition that is self-limited in 75% to 90% of cases, and usually resolves over a 1- to 3-year period without the need for intervention. 1 Therefore, in the absence of history, signs, and symptoms suggestive of an underlying pathology or secondary cause, monitoring and reassurance for patients and their families are the mainstay of early management. 2 Surgical treatment is typically reserved for gynecomastia cases that have persisted beyond 2 years.2,3
However, gynecomastia during adolescence, a period of increased awareness of one's self-image and sexual identity, has raised important questions about the psychological impact of gender-incongruent development, and the role of earlier surgical intervention in the context of significant psychosocial distress secondary to the condition.2,4,5 To date, several studies have demonstrated the detrimental psychological impact of gynecomastia during adolescence, which results in impairments in social functioning, mental health problems such as depression and anxiety, as well as diminished self-esteem.4,5 In an attempt to conceal their chest, some patients engage in coping behaviors such as wearing multiple layers of clothing, hunching their shoulders, and binding their chest with household items, which in turn may cause discomfort, pain, and even injury. 5
Surgery for gynecomastia has the potential to significantly improve patients’ quality of life. Nuzzi et al 6 previously showed that adolescent patients with gynecomastia scored significantly worse on the Rosenberg Self-Esteem Scale (RSES) and in several domains of the Short-Form 36 (SF-36) compared to unaffected male controls. Postoperatively, RSES and SF-36 scores significantly improved for gynecomastia patients and, in fact, were comparable to those of unaffected controls. 6 Similar improvements in psychosocial well-being after surgery have been reported in the adult gynecomastia population.7,8
To date, the impact of adolescent gynecomastia surgery has only been assessed using generic quality of life measures.6,9 While helpful in measuring general concepts of quality of life, generic patient-reported outcome measures (PROM) may lack the sensitivity to capture the nuanced issues of living with gynecomastia or chest differences. 10 Accurate and thorough characterization of the impact of gynecomastia surgery on adolescent patients’ quality of life can aid our understanding of the significance of this surgery for this patient population, which in turn may have important implications for destigmatizing gynecomastia surgery. To this end, the present study aims to assess adolescent gynecomastia patients’ postoperative quality of life using a PROM specific for body contouring procedures. This study will also aim to identify patient and operative characteristics associated with worse quality of life scores, as well as to identify patients who may be at higher risk of low postoperative satisfaction, and for whom additional psychosocial support may be needed.
Methods
Study Design
This was a cross-sectional study of patients who previously underwent surgery for adolescent gynecomastia. This project was approved by the Univeristy of British Columbia Children's and Women's Research Ethics Board (H23-01006). This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines 11 (Supplemental Digital Content 1).
Patients were recruited from the senior author's (JA) clinical practice at BC Children's Hospital, a quaternary hospital in Vancouver, Canada. In general, patients were considered appropriate surgical candidates if their gynecomastia had persisted for more than 2 years, and they were believed to have reached a plateau in their linear growth. Patients who underwent surgical treatment for Simon grade I, IIa, or IIb adolescent gynecomastia from May 2009 to November 2022 were eligible for inclusion in the present study. Patients with grade III gynecomastia were excluded from the present study due to low case numbers, and given that they are often treated with a surgical technique that necessitates a different type of incision and results in more significant scarring. Eligible patients were invited to participate in the study via post mail and telephone call, and informed consent was obtained.
To assess the quality of life, patients who consented to participate in the study completed the Satisfaction with Chest and Psychological Function scales of the Body Contouring Questionnaire (BODY-Q), either on an online platform or over the phone, as per participants’ preference. The BODY-Q is a PROM developed by Klassen et al 12 for assessing patient perceptions after weight loss and/or body contouring procedures. The BODY-Q consists of 29 independently functioning scales which can be individually administered to meet the specific objectives of a given research project. In the present study, the Satisfaction with Chest and Psychological Function BODY-Q scales were administered to participants to capture both their satisfaction with the physical appearance of their chest, and their psychological well-being. Both scales consist of ten items which the patient rates on a 4-point scale, with answer options ranging from “very dissatisfied (1 point)” to “very satisfied (4 points),” or “strongly disagree (1 point)” to “strongly agree (4 points).” Higher scores on these scales reflect a better outcome.
Demographic, disease, and treatment characteristics were collected for those participants who additionally consented to chart review. For each patient, the latest documented Simon grade and weight and height measurements prior to the surgery date were recorded, where available. Where a definitive Simon grade was not documented, pre-operative surgery day photographs were reviewed by the senior author (JA), and a Simon grade was assigned retroactively. The Simon classification system 13 was used in the present study as it is the most common classification system reported in the gynecomastia literature. 14 Furthermore, it is the classification system that has been used in the assessment of gynecomastia patients in the senior author's clinical practice, and was thus the classification available in the medical records used to collect patient data for this study.
Surgical Technique
All patients underwent gynecomastia surgery under general anesthesia in a standard operating theatre. Direct excision of fibroglandular and fatty breast tissue proceeded via a periareolar incision. This technique does not involve the use of liposuction to remove additional adipose tissue. Following the excision of the breast tissue, the skin was closed, and a chest binder was applied. Patients were admitted for a one-night stay in hospital. Surgical drains were not routinely used in this population. After surgery, patients were advised to wear a tight compression shirt, and to refrain from physical activity and heavy lifting for one month.
Data Analysis
Descriptive statistics were used to summarize demographic, disease, and treatment characteristics for the study sample. Data are presented as medians (with interquartile range [IQR]), or proportions, as appropriate.
Raw scores from the BODY-Q scales were summed and converted into Rasch transformed scores (scale of 0–100) using conversion tables obtained from the authors of the BODY-Q. Mean and median scores were calculated for each scale of the BODY-Q, and the distribution of scores in the study sample was illustrated with box and whisker plots.
An independent samples t test was conducted to compare the mean BODY-Q scores of the study sample to previously published normative BODY-Q scores of unaffected males of a similar age and BMI range. 15 Given the nonnormal distribution of data, linear univariate regression, Kruskall-Wallis test, and Mann-Whitney U test were used, where appropriate, to examine the association between BODY-Q Satisfaction with Chest or Psychological Function scores and the following independent variables: age at the time of survey completion; BMI at the time of survey completion; pre-operative Simon grade; whether or not the patient had postoperative complications; and whether or not the patient had revision procedures. Results are presented as P-values with 95% confidence intervals (CI). Statistical significance was set to P < .05. All statistical analyses were conducted in RStudio Version 1.4.1717 (RStudio; Boston, MA).
Results
Study Participants
Based on inclusion criteria, 79 patients were eligible for inclusion in the present study. Seventy-six patients were able to be contacted via telephone or post mail, and 37 consented to complete the BODY-Q (response rate = 48.7%). Twenty-three of these patients additionally consented to chart review. A flowchart outlining patient recruitment is illustrated in Supplemental Digital Content 2.
Table 1 summarizes the demographic, gynecomastia severity, and treatment characteristics of the study sample. At the time of survey completion, the median age of participants was 23.3 years, and the median BMI was 26.5. The majority (59.5%) of patients had Simon grade IIb gynecomastia. Of the 23 patients who consented to chart review, all had idiopathic adolescent gynecomastia. Furthermore, 22 of 23 patients (95.7%) endorsed a history of bullying, teasing, or feeling self-conscious about their chest appearance. The patients consenting to participate in the present study did not differ significantly from those who declined participation with respect to age, Simon grade, and follow-up duration (Supplemental Digital Content 3).
Patient and Treatment Characteristics.
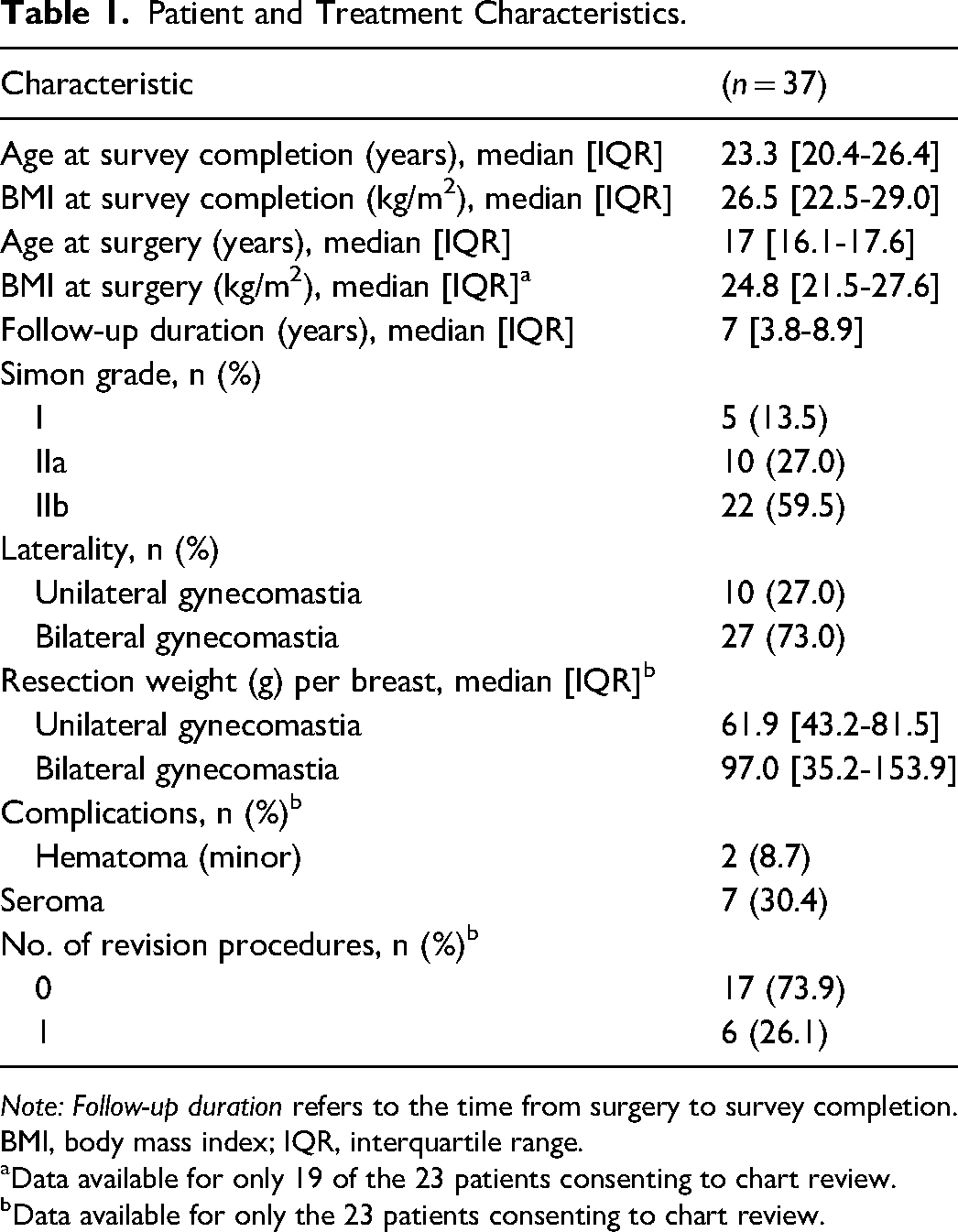
Note: Follow-up duration refers to the time from surgery to survey completion. BMI, body mass index; IQR, interquartile range.
Data available for only 19 of the 23 patients consenting to chart review.
Data available for only the 23 patients consenting to chart review.
Satisfaction and Quality of Life
The median scores on the BODY-Q Satisfaction with Chest and Psychological Function scales were 70 [IQR, 57.5-100] and 71 [IQR, 60-92], respectively (Figure 1). The mean score on the Satisfaction with Chest scale in the study sample was significantly higher than that in the normative population (73.6 and 54.0, 15 respectively; t(106) = 3.7, P = .0004). Similarly, the mean score on the Psychological Function scale was significantly higher in the study sample compared to the normative population (73.0 and 61.4, 15 respectively; t(132) = 3.3, P = .0014).
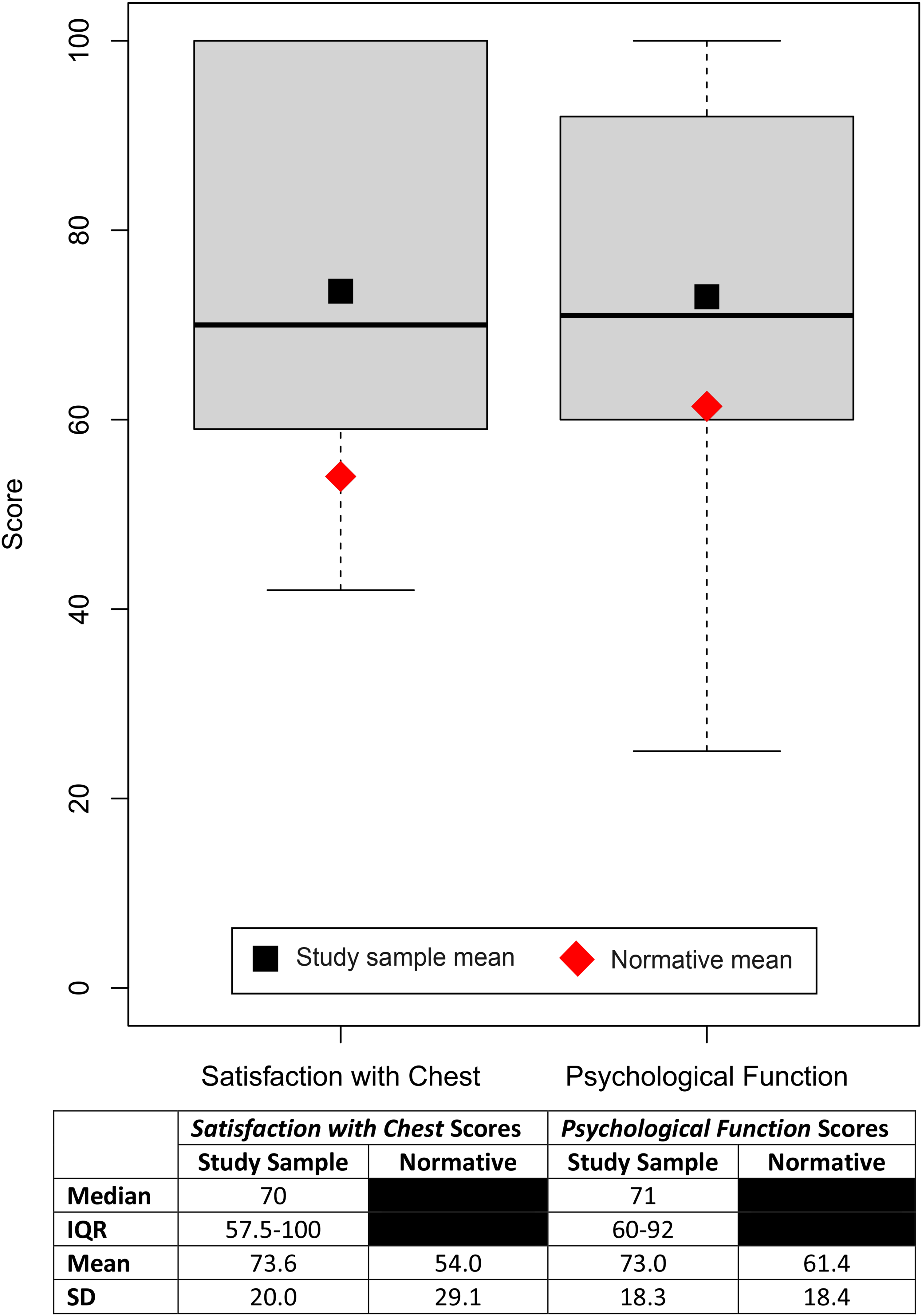
Body Contouring Questionnaire (BODY-Q) score summary.
Factors Associated with Satisfaction and Quality of Life
Patients who underwent a revision procedure had a median Satisfaction with Chest score 25.5 points lower than those who did not undergo a revision (Mann-Whitney U-test; P = .045, 95% CI,
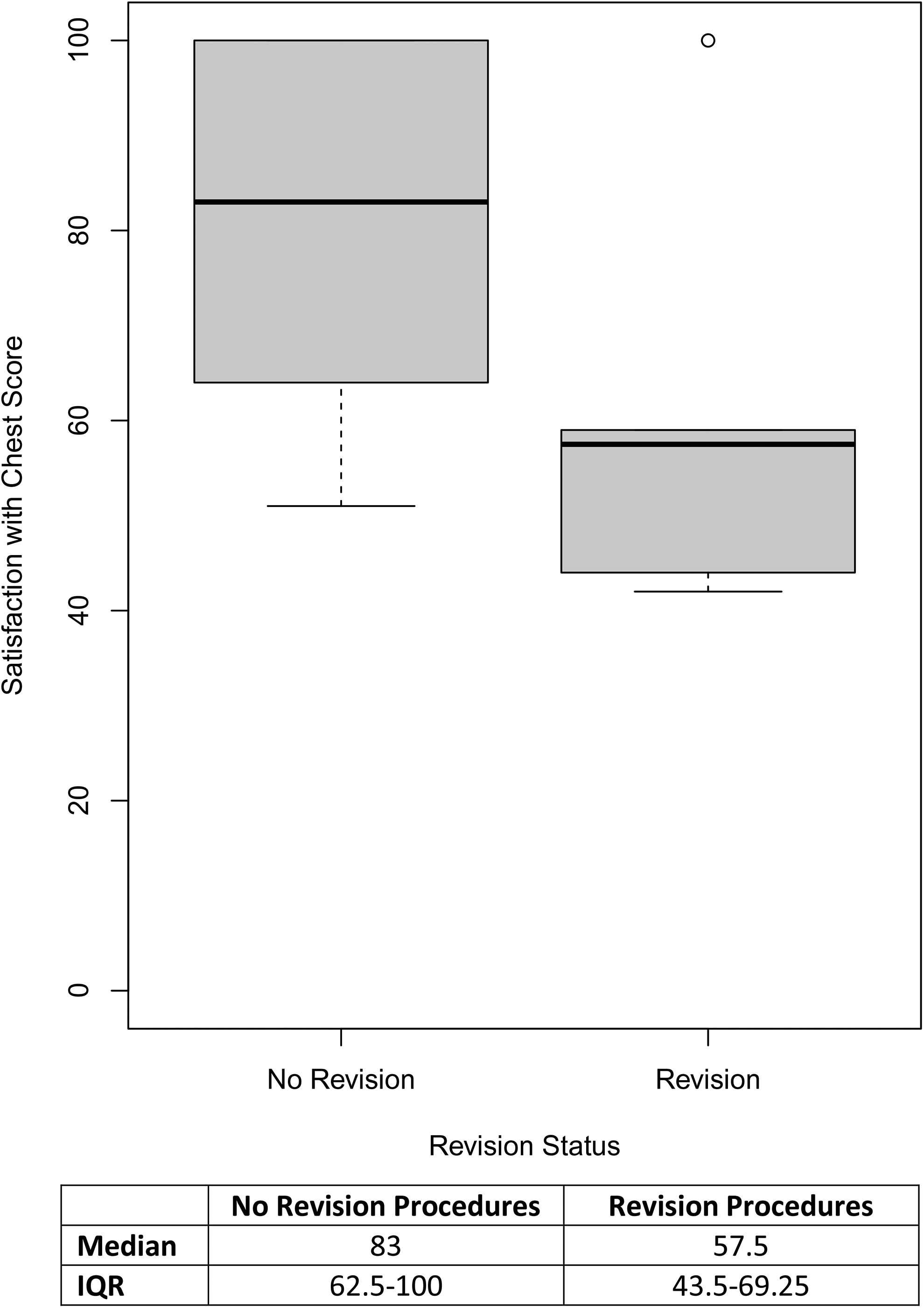
Satisfaction with chest scores by revision procedure status.
Univariate linear regression did not demonstrate Satisfaction with Chest scores to be significantly associated with age at survey completion, R2 = 0.034; F(1, 35) = 1.2; P = .28, nor BMI at survey completion, R2 = 0.037; F(1, 35) = 1.4; P = .25. Psychological Function scores were also not associated with age at survey completion, R2 = 0.069; F(1, 35) = 2.6; P = .12 nor with BMI at survey completion, R2 = 0.022; F(1, 35) = 0.78; P = .38. A Kruskal-Wallis test was performed and did not reveal Simon grade to be a significant predictor of neither Satisfaction with Chest, H(2) = 2.7; P = .26, nor Psychological Function, H(2) = 2.2; P = .34 scores. Finally, a Mann-Whitney U-test showed that the presence of postoperative complication(s) was not significantly associated with Satisfaction with Chest (P = 1; 95% CI, −17.0-30.0) or Psychological Function (P = .51; 95% CI, −25.0-16.0) scores.
Discussion
To our knowledge, the present study is the first to assess the quality of life in adolescent gynecomastia patients with a PROM specific for body contouring procedures. The BODY-Q Satisfaction with Chest scale captures the nuanced aspects of living with a chest difference, thus allowing for a more sensitive and accurate characterization of patients’ thoughts and feelings posttreatment. Mean BODY-Q Satisfaction with Chest and Psychological Function scores were higher by 19.6 and 11.6 points, respectively, in our study sample compared to normative scores from unaffected males of a similar age and BMI (Figure 1).
At present, the only available data on minimally important differences (MID) for the BODY-Q comes from a study in patients undergoing body contouring after weight loss surgery, in which the MID was determined to be 4.5. 16 By this standard, the differences in scores between our study sample and the normative population are considered clinically significant, although it should be cautioned that this MID may not be reflective of the gynecomastia population. Future research to establish a MID for the BODY-Q in this patient population is needed.
While we cannot make definitive conclusions regarding the reason for higher chest satisfaction scores in our study sample compared to the normative population, we speculate that gynecomastia surgery may confer gains in chest-related quality of life that extend beyond simply addressing the perceived physical deficits experienced by adolescent males with gynecomastia. In a study by Mundy et al, 17 researchers compared normative BREAST-Q scores to pre- and postoperative scores from a sample of women who had undergone breast augmentation. Pre-operatively, patients reported Satisfaction with Breast scores that were significantly lower than normative values, while postoperative scores were significantly higher than in the normative sample. The researchers suggested that breast augmentation surgery may not only correct perceived deficits, but also results in psychological benefits that enhance patients’ quality of life. 17 Similarly, in gynecomastia patients, who are known to have impaired psychosocial functioning as a result of gender-incongruent chest development, gynecomastia surgery may do more than simply give them a perceived “normal-appearing” male chest—it additionally imparts psychological benefits which in turn may enhance one's satisfaction with their appearance and body image. Alternatively, the higher chest satisfaction scores in our study sample may be explained by the Hawthorne effect, which posits that research participants may improve their behavior as a result of their awareness of being studied. 18
Satisfaction with Chest scores were comparable to postoperative scores reported in the adult gynecomastia literature.8,19,20 Satisfaction with chest appearance was found to be significantly lower in those patients who underwent a revision procedure after the primary gynecomastia surgery. This is consistent with several other reports of decreased satisfaction among patients who required revision surgery versus those who did not, across a variety of surgery types.21–23 We speculate that this difference in satisfaction scores may be the result of unmet expectations, compounded by the added burden of undergoing additional treatment. Given the relatively high rate of revision procedures after primary gynecomastia surgery, 24 this finding has important implications for preoperative counseling, and management of patient expectations. Surgeons should have this discussion pre-operatively, especially with patients at higher risk of requiring a revision procedure. Revision rates have previously been shown to be associated with gynecomastia severity, with higher rates reported in patients with more severe gynecomastia. 24 While we did not find significant differences in Simon grade between patients who underwent revision surgery and those who did not in our study sample, this may be due to the small sample size and the relatively low number of revision events.
Patients’ satisfaction with chest appearance was not associated with age, BMI, Simon grade, or postoperative complication status. Furthermore, none of the assessed patient, disease, and treatment factors were significantly associated with BODY-Q Psychological Function scores. This is consistent with existing gynecomastia literature demonstrating gains in health-related quality of life postgynecomastia surgery, irrespective of BMI, gynecomastia severity, and complication status. 9
Gynecomastia and its surgical treatment remain stigmatized in the medical community and society at large. 25 There has been relatively little research dedicated to studying gynecomastia and its impact on patients, and gynecomastia treatment is often seen solely as a cosmetic procedure. 25 This is in stark contrast to the abundance of research on breast surgery in females, and the successful medicalization of breast reconstruction, augmentation, and reduction for female patients.25,26 In addition to the stigma, gynecomastia patients also face financial barriers in accessing treatment. Rasko et al 27 found that only 14 of the 61 US insurance companies evaluated in their 2019 study considered coverage for gynecomastia surgery for adolescent patients. In British Columbia, our provincial health insurance provides coverage for gynecomastia surgery for both adolescent and adult patients, thus removing this financial barrier. The relatively high satisfaction and psychological function scores seen in our sample demonstrate that patients fare well after undergoing surgical treatment for adolescent gynecomastia, which in turn may be a positive step towards the destigmatization of this procedure, understanding its significance for the psychosocial well-being of this patient population, and increasing awareness and access to surgical treatment.
Limitations
Patients were recruited from the clinical practice of a single surgeon at a quaternary center, thus limiting the generalizability of these results. The exclusion of Simon grade III gynecomastia patients further limits the scope of our findings. The relatively small sample size (n = 37) and a response rate of 48.7% may limit the reproducibility of these findings and increase variability in the final results. However, it should be noted that a response rate of 40% is generally considered adequate, 28 and those who agreed to participate did not differ from those who did not participate with respect to age, Simon grade, and follow-up duration. A further limitation is that the lack of preoperative quality of life scores does not allow us to directly assess the impact of gynecomastia surgery. Future research should employ a prospective cohort design and assess quality of life both before and after treatment, so as to more directly assess the impact of gynecomastia surgery on patients. Changes in scores should be compared against established clinically important differences for BODY-Q scores.
Conclusion
Patients who underwent surgery for adolescent gynecomastia with a periareolar incision to directly excise fibroglandular and fatty breast tissue fare well with respect to satisfaction with chest appearance, and psychological function. Surgeons may consider performing surgery on appropriate adolescent candidates, as there was no difference in outcomes based on age, BMI, gynecomastia severity, or complication status. Revision procedures may result in lower postoperative satisfaction with chest appearance, and this should be an important point of discussion in pre-operative counseling and expectation management, particularly in patients with more severe gynecomastia, which has previously been shown to be associated with higher revision rates. Our findings demonstrate a positive patient-reported impact of gynecomastia surgery among our survey respondents, and this is an important step towards increased awareness, access, and acceptance of gynecomastia treatment in adolescents. Future research should measure quality of life before and after surgery, to allow for more definitive conclusions about the salutary effects of gynecomastia surgery.
Supplemental Material
sj-docx-1-psg-10.1177_22925503241249753 - Supplemental material for Quality of Life Measured Using the BODY-Q After Adolescent Gynecomastia Surgery: A Cross-Sectional Analysis
Supplemental material, sj-docx-1-psg-10.1177_22925503241249753 for Quality of Life Measured Using the BODY-Q After Adolescent Gynecomastia Surgery: A Cross-Sectional Analysis by Marta Karpinski, Young Ji Tuen, Rebecca Courtemanche and Jugpal S. Arneja in Plastic Surgery
Supplemental Material
sj-docx-2-psg-10.1177_22925503241249753 - Supplemental material for Quality of Life Measured Using the BODY-Q After Adolescent Gynecomastia Surgery: A Cross-Sectional Analysis
Supplemental material, sj-docx-2-psg-10.1177_22925503241249753 for Quality of Life Measured Using the BODY-Q After Adolescent Gynecomastia Surgery: A Cross-Sectional Analysis by Marta Karpinski, Young Ji Tuen, Rebecca Courtemanche and Jugpal S. Arneja in Plastic Surgery
Supplemental Material
sj-docx-3-psg-10.1177_22925503241249753 - Supplemental material for Quality of Life Measured Using the BODY-Q After Adolescent Gynecomastia Surgery: A Cross-Sectional Analysis
Supplemental material, sj-docx-3-psg-10.1177_22925503241249753 for Quality of Life Measured Using the BODY-Q After Adolescent Gynecomastia Surgery: A Cross-Sectional Analysis by Marta Karpinski, Young Ji Tuen, Rebecca Courtemanche and Jugpal S. Arneja in Plastic Surgery
Supplemental Material
sj-docx-4-psg-10.1177_22925503241249753 - Supplemental material for Quality of Life Measured Using the BODY-Q After Adolescent Gynecomastia Surgery: A Cross-Sectional Analysis
Supplemental material, sj-docx-4-psg-10.1177_22925503241249753 for Quality of Life Measured Using the BODY-Q After Adolescent Gynecomastia Surgery: A Cross-Sectional Analysis by Marta Karpinski, Young Ji Tuen, Rebecca Courtemanche and Jugpal S. Arneja in Plastic Surgery
Footnotes
Acknowledgments
The author would like to thank the patients who participated in this study, as well as Sophia Shayan for administrative support.
Authors’ Contributions
MK, YJT, RC, and JA contributed to the study conceptualization and design, data interpretation, manuscript writing and editing, and approved the manuscript version to be published. MK, YJT, and RC contributed to data collection and analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This project was approved by the University of British Columbia Children's and Women's Research Ethics Board (H23-01006). All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all patients for being included in the study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the BC Children's Hospital Research Institute Summer Studentship, Faculty of Medicine, University of British Columbia (grant number GR027183, and Surgery Clinical Faculty Research Support Award for Dr. Jugpal Arneja).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.