
Abstract
Background
Gynecomastia is a benign condition that develops due to the proliferation of breast tissue in men. Surgical excision is the most effective treatment method. Minimally invasive techniques can be used to avoid visible scarring. We evaluated the efficacy and safety of air-assisted subcutaneous mastectomy in the treatment of gynecomastia.
Patient and Methods
10 patients with gynecomastia underwent air-assisted subcutaneous mastectomy and liposuction through a single axillary incision, between June 2022 and February 2023. Demographic and clinical data of the patients, duration of surgery, and complications were recorded. The satisfaction levels of the patients regarding physical appearance, mental status, and social environment were measured. The body Q questionnaire was performed preoperatively and in the postoperative third month.
Results
The median age was 26 (range, 18-54). Surgical excision was measured as a median of 69 gr (range, 41-177), and liposuction volume was measured as a median of 210 ccs (range, 63-400). The median operation time was 50 minutes (range, 21-60) for excision and 21 minutes (range, 20-75) for liposuction. Body, chest, and nipples related appearance satisfaction levels were measured preoperatively as a median of 44 (range, 36.5-52), 31 (range, 27.5-39), and 51.5 (range, 21-69.8) points vs postoperatively as 92 (range, 92-100), 93 (range, 93-94.8) and 90 (range, 90-100) points, respectively. The patients had a median follow-up of 6 months (range, 3-11). No complications were observed during the follow-up period.
Conclusion
Air-assisted subcutaneous mastectomy and liposuction is a feasible technique that may provide good cosmetic outcomes by avoiding anterior chest wall scarring.
Introduction
Gynecomastia is a benign condition that develops due to the proliferation of breast tissue in men. Physiological gynecomastia is common in newborns, adolescents, and elderly men. 1 To reveal the etiology of gynecomastia, careful anamnesis, physical examination, hormone tests, and ultrasonography should be performed. Breast tumors, endocrine or systemic diseases should be excluded. Gynecomastia rarely requires surgical treatment for cosmesis and analgesia. Surgery is preferred for patients with prolonged symptoms and for whom medical treatment is ineffective.1,2
Surgery for gynecomastia may cause complications such as contour irregularity, nipple-areola complex collapse and distortion, subtotal glandular resection, ischemia, necrosis, and hypertrophic scarring. 3 Minimally invasive surgical techniques are used in the treatment of gynecomastia to improve cosmetic results and reduce complication rates.4–10 Vacuum-assisted biopsy and liposuction are minimally invasive methods for gynecomastia. These methods can be performed through a small incision from the anterior axillary line and the inframammary fold. 11 Recently endoscopic mastectomy has been described as an alternative technique.12–17
We aimed to share our experience with a novel technique: air-assisted subcutaneous mastectomy through a single axillary incision. We also evaluated the efficiency and safety of this technique also its effects on patient satisfaction.
Patients and Methods
The approval of the local ethics committee (Istanbul Medical Faculty Clinical Research Ethics Committee Number: E−29654016-050.99-1475186) was acquired for our study. Detailed informed consent was obtained from all patients. Between June 2022 and February 2023, 10 patients with gynecomastia underwent air-assisted subcutaneous mastectomy through a single axillary incision. Detailed anamnesis, physical examination, breast ultrasound, and necessary laboratory tests were performed preoperatively for all patients. 1 patient who required skin excision was excluded from the study. Ten patients underwent air-assisted subcutaneous mastectomy with simultaneous liposuction. Physical appearance, mental satisfaction, and social environment-related satisfaction were assessed with the Body-Q scale three months after surgery.
Surgical Technique
The patient was positioned supine on the operating table with the arm abducted. A 1 cm axillary incision was made in the anterior axillary line and the lateral side of the pectoralis major muscle was reached. The hand pump inserted lipoplasty cannula (Figure 1) was pushed forward into the subcutaneous space through this incision. The hand pump was connected to the CO2 insufflator, the breast tissue and subcutaneous area were separated as much as possible by the insufflation of high-pressure CO2. Glandular tissue was separated from the subdermal fat layer with air assistance and the dissection of Cooper’s ligament was facilitated. Continuing the dissection in an appropriate avascular plane reduced bleeding, and minimized residual breast tissue. Aspiration-type cannula with the hand pump.
Dissection was headed towards the areola through the separated superficial plane by a vessel sealing device. Breast tissue was completely dissected from the subcutaneous tissue except the nipple-areola complex, then the nipple was lifted upwards manually and the nipple-areola complex was separated with the vessel sealing device by applying traction towards the thorax wall. Thus, it was aimed to reduce depression by leaving a thicker retroareolar area. After all of the glandular tissue was separated from the subdermal layer, deep plane dissection was performed and the breast tissue was dissected over the pectoralis major muscle. The plane between the breast tissue and the pectoral muscle was dissected through the incision at the lateral border of the pectoral muscle, the breast tissue was lifted upwards from this area with a vessel sealing device. The breast tissue was separated from the pectoral muscle by using this plane. Mobilized breast tissue was removed from the axillary incision (Figure 2). Peroperative photographs.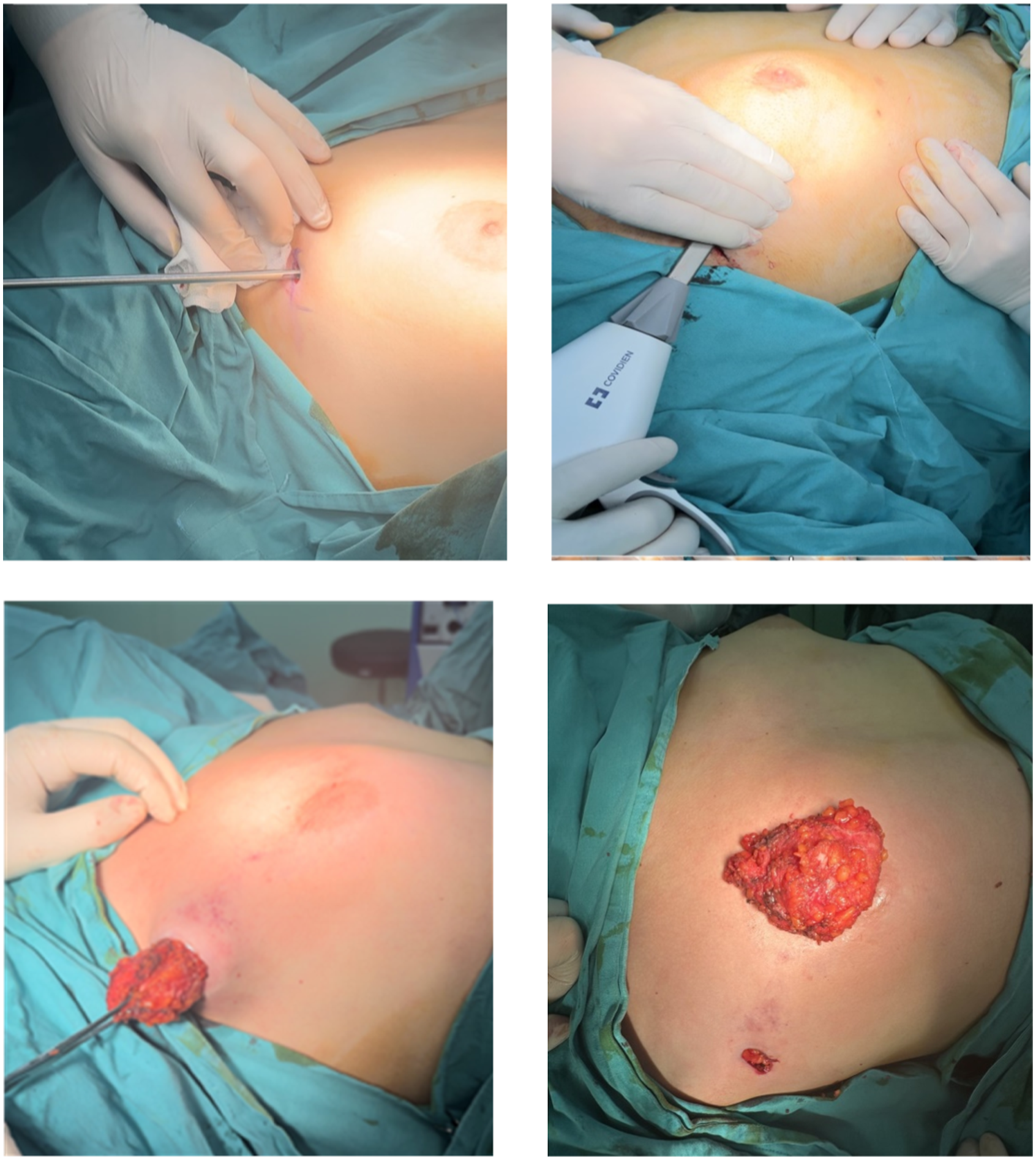
After the excision was done, liposuction was performed by the Plastic Reconstructive and Aesthetic surgeons with the wet technique. Forty milligrams of lidocaine and 1 milligram of adrenaline were added to 1000 milliliters of %0.9 NaCl solution to prepare the infiltration solution. Then, a total of 300 to 350 milliliters of the solution was administered to each breast. After waiting for seven minutes, pre-tunneling was performed through the small mastectomy incision and liposuction was completed with the standard cannula and without any power-assisted devices. The liposuction aimed to smoothen the chest contours and avoid any gross asymmetries of the resection sites. Liposuction was focused on subcutaneus fat tissue around the glandular excision area. Care was taken to avoid any depressions under the nipple-areola complex and the mastectomy flaps. Each breast is checked for asymmetry and subcutaneous roughness, and additional liposuction is performed if necessary. The drain is placed, and after resection of 1 millimeter of incision margins wound is closed subcutaneously. Compression dressings were applied to reduce dead space and patients were advised to wear these dressings for two months.
Statistical Analysis
The statistical analysis tool, Statistical Package for the Social Sciences (SPSS) version 25.0 (IBM Corp., Armonk, NY, USA) is used to evaluate the findings of the study. Satisfaction levels related to physical appearance, mental status, and social environment were scaled using the 10-point Visual Analog Scale (VAS). Shapiro-Wilk test, descriptive statistical methods, Spearman correlation test, Mann-Whitney U test, and Pearson Chi-Square test were used in statistical analysis.
Results
Patient Characteristics
Patient Characteristics.
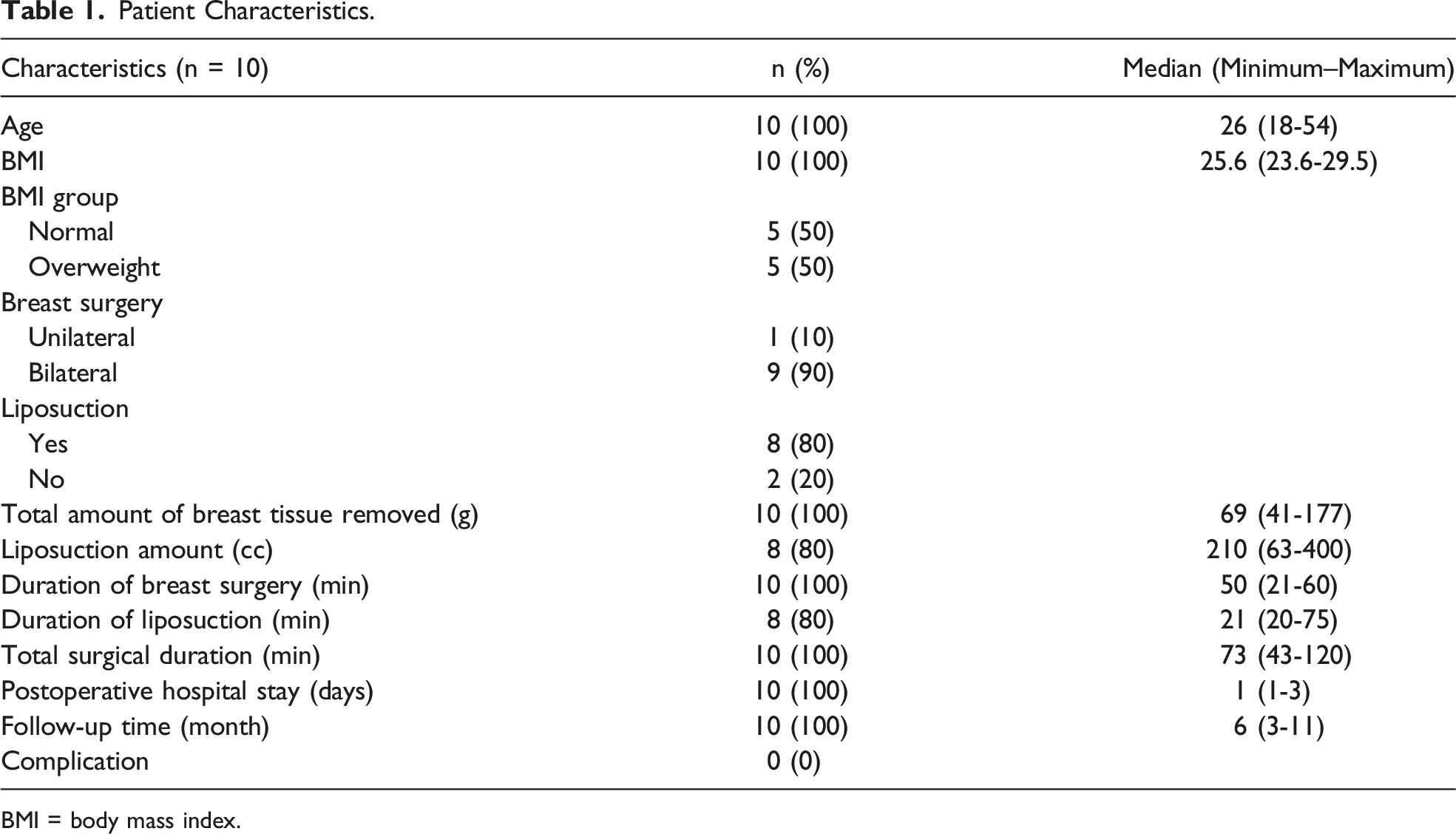
BMI = body mass index.
BODY-Q Scales
Appearance Satisfaction
Preoperative and Postoperative BODY-Q Scores.
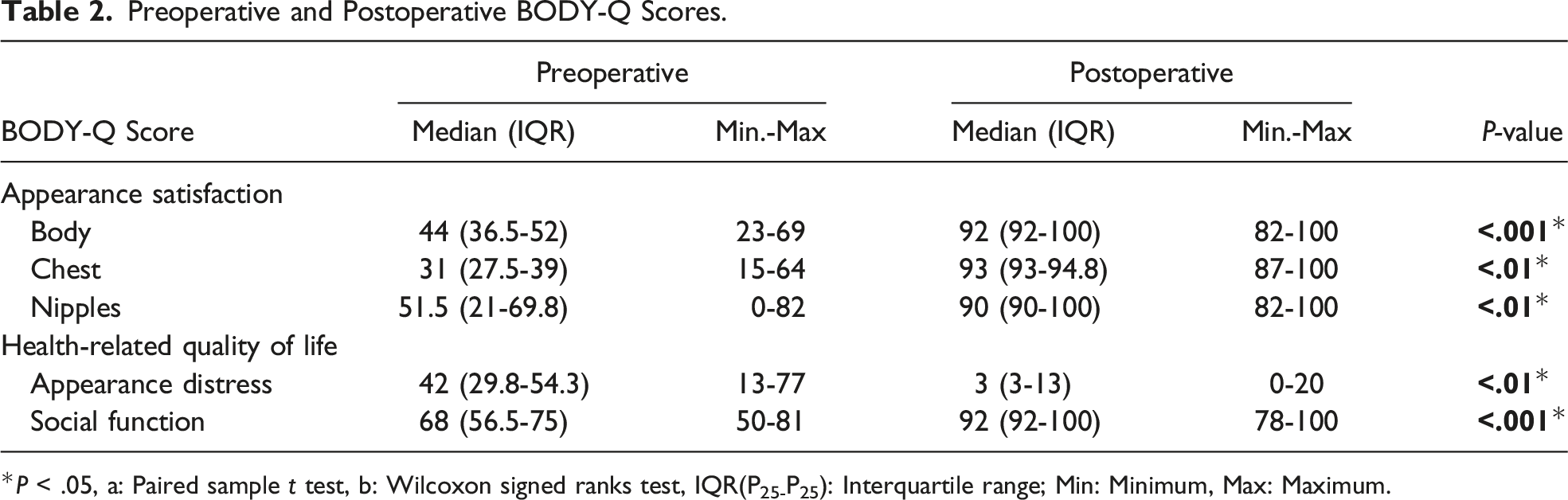
*P < .05, a: Paired sample t test, b: Wilcoxon signed ranks test, IQR(P25-P25): Interquartile range; Min: Minimum, Max: Maximum.
Health-related Quality of Life
The preoperative appearance distress level of the patients decreased from the median 42 (range, 29.8-54.3) points to 3 (range, 3-13) points in the early postoperative period (P < .01) Figure 3. The preoperative social function-related quality of life level increased from 68 (range, 56.5-75) points to 92 (92-100) points (P < .001) (Table 2). Preoperative and early postoperative images of a patient who underwent air-assisted minimally invasive surgery and liposuction.
Discussion
Periareolar, transareolar, and inframammary incisions with or without skin excision can be used for surgical treatment of gynecomastia. The free nipple technique can be performed in patients who require a large amount of skin excision. 3 Ohyama et al performed Endoscope-assisted transaxillary glandular tissue removal in gynecomastia. 18
Jarar et al performed liposuction with the injection of lipolysis solution through a 15 mm incision at the anterior axillary line. They excised the remaining fibroglandular tissue by entering with the endoscope from the same incision. 5 Yang et al performed endoscopic subcutaneous mastectomy and liposuction in 45 cases of gynecomastia. They performed liposuction by giving a tumescent solution from a 3 cm axillary incision and subcutaneous mastectomy was completed with sharp dissection using Metzenbaum scissors with the help of retractors. 14 In this study, the pneumocooper is formed with the CO2 insufflation from a cannula and the cooper ligaments are dissected through a single port without using any retractor. The vessel sealing device is used for dissection, so bleeding is minimal. Excessive fat tissue around breast tissue is removed by using liposuction after the excision of fibroglandular tissue. Cosmetic outcomes may be improved with this approach.
Varlet et al performed endoscopic subcutaneous mastectomy with 3 ports and in their study, the mean operation time was found to be 93 minutes for each breast. 13 Tukenmez et al 19 performed endoscopic mastectomy from a single axillary incision for 30 gynecomastia patients and they reported 120 minutes of median operation time. The technique we described does not use a port or continuous insufflation, and as a consequence problems and difficulties of endoscopic surgery wouldn't occur. CO2 insufflation into the subcutaneous space with a hand pump and the large jaw vessel sealing devices also facilitates the dissection. Therefore, the operation time is shorter in our study compared to other techniques (median 73 minutes).
Liposuction can be used alone or in combination with other techniques in gynecomastia surgery. 9 Especially in cases with excess subcutaneous adipose tissue, depression may occur around the nipple-areola complex after the breast tissue is excised. Liposuction may be useful for correcting the depression of the nipple-areola complex, asymmetry, and roughnesses.
Patients with gynecomastia suffer from anxiety, depression, and social phobia. Successful surgery cosmetically corrects the chest area and it also has a positive effect on psychological well-being. 20 Similarly, in our study, mental and social environment satisfaction levels that were evaluated using Body-Q scales were found to be high in patients who underwent gynecomastia surgery.
Air-assisted minimally invasive mastectomy has many advantages over open surgery, such as a small incision, less tissue trauma, increased nipple viability, and early healing. Besides this technique is not suitable for patients who require skin excision.
Air-assisted nipple-areola-sparing mastectomy and liposuction is a safe and effective alternative for the surgical treatment of gynecomastia. This technique also achieves increased physical appearance, mental status, and social environment-related satisfaction levels. The operation time is shorter in air-assisted minimally invasive surgery compared to endoscopic techniques. Air-assisted minimally invasive surgery can be performed as an alternative method for surgical treatment of gynecomastia in experienced hands for patients who don’t require skin excision. Although our results are promising, studies with larger number of patients are needed.
Footnotes
Author Contributions
Tukenmez M: Design of the work.
Tukenmez M, Emiroglu S, Kozanoglu E, Mollavelioglu B: Acquisition of data.
Tukenmez M, Mollavelioglu B: Analysis and interpretation of data.
Tukenmez M: Drafting.
Tukenmez M, Cabioglu N, Muslumanoglu M: Important intellectual content.
All the authors have approved the final version of the manuscript to be published.
Acknowledgements
The authors are grateful to Atilla Bozdogan, MSc who helped with the preparation of the statistical analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient Consent Statement
Authors confirm that guidelines on patient consent have been met and any details of informed consent obtained.