
Abstract
Introduction
Cubital tunnel syndrome (CuTS) most commonly occurs as a consequence of the ulnar nerve becoming compressed at the elbow. 1 There are approximately 75,000 incident cases of CuTS per year, making cubital tunnel syndrome the second most common compressive neuropathy. 2 Cubital tunnel syndrome left untreated can result in forearm and intrinsic hand muscle atrophy, and loss of sensation. 1 As a result, surgical management is offered to patients with persistent symptoms after a trial of conservative therapy. While the literature is rich with studies comparing the different surgical approaches,1–5 there is a lack of evidence on managing CuTS surgical patients postoperatively.
Various healthcare institutions publish their ulnar nerve transposition protocol publicly and an informal review of the current clinical practices demonstrates great heterogeneity. Protocols reveal practitioners are immobilizing patients at 90 degrees elbow flexion anywhere from one to four weeks post cubital tunnel release (CuTR).6–8 These lengths of immobilization contrast observations made in the hip and knee literature which reveal early mobilization can be achieved within 24 hours of operation, resulting in reduced hospitalization without an increase in adverse events.9–11 In addition, studies have shown that there is no beneficial effect from post-operative immobilization after carpal tunnel decompression when compared to early mobilization.12,13
The main risk with immobilization of the elbow is stiffness. 14 Elbow stiffness and contracture have significant implications on a patient's ability to complete their activities of daily living, such as feeding and hygiene. 15 Historically, immobilization was used to ensure the stability of the joint, and to reduce pain and swelling. 16 Anecdotally, the risks of mobilizing too early may include wound dehiscence, ulnar nerve injury, development of seroma, and pain. However, there is a growing body of evidence to suggest that early mobilization after elbow dislocation is a safe and effective treatment, which reduces the return-to-work times and improves functional outcomes.14,16–18
To date, there are no published systematic reviews or recent, large, clinical trials on this topic. Considering the widespread impact of this compression neuropathy and its high rate of operative management, it is imperative that the best possible postoperative functional outcomes are achieved. This systematic review aims to compare the effectiveness of early versus late mobilization after operative management of cubital tunnel syndrome in adults.
Methods
Study Selection and Data Extraction
Two authors (ORO and MH; ORO and TE) independently examined titles and abstracts for potentially relevant studies. Studies that resulted in disagreement were also advanced to full-text screening. Full texts of studies that met the inclusion criteria based on participants’ age, procedure, and type of interventions (as highlighted below), were obtained; and the same authors independently screened the full text for inclusion. Randomized controlled trials (RCTs), quasi-randomized controlled trials, cohort studies, and case-control studies were included. Studies were included without date or language restrictions. Case-series were excluded from this review because they lack a comparison group. Consensus was achieved by team discussion or review by the senior author. Data extraction was carried out by one reviewer using a piloted data extraction form and were confirmed by another reviewer. After extraction, the outcome data were entered into Review Manager 5 software. 19 The PRISMA 2020 checklist was used to guide the reporting conduct of this systematic review which was registered on PROSPERO (CRD42020168494).
Type of Participants
We included adult patients (≥18 years of age) diagnosed with CuTS who underwent operative release regardless of surgical approach - including but not limited to in-situ decompression, ulnar nerve transposition, and medial epicondylectomy. We excluded studies with participants who had multiple compression syndromes ipsilaterally, unless separate data concerning the compression neuropathy at the elbow was presented.
Types of Interventions
The interventions being evaluated were early versus late mobilization. We defined early mobilization a priori as any intervention which encouraged active movement, active-assisted movement, or passive movement of the elbow joint within 72 hours of operation. All mobilization regimens (eg, intensity, personnel, and frequency) were included and documented. Late (or delayed) mobilization was defined as being immobilized until day four post-operation. All forms of immobilization that prevented patients from engaging in movement were considered.
Types of Outcome Measures
For this review, we selected common outcomes that are important to patients and their providers, 20 including: (1) return to work or activities of daily living, (2) grip strength, (3) pain (any validated scale), (4) adverse outcomes (including infection, dehiscence, joint contracture, or reoperation), (5) range of motion (flexion, extension, pronation and supination) and (6) quality of life (validated health-related quality of life scale).
Search Methods
We searched the following electronic databases for eligible studies:
Cochrane Central Register of Controlled Trials (CENTRAL) (searched 18 January 2023); MEDLINE including In-Process & Other Non-Indexed Citations (1946 to 18 January 2023); EMBASE (1974 to 18 January 2023); Physiotherapy Evidence Database (PEDro) (searched 18 January 2023) ClinicalTrials.gov (www.clinicaltrials.gov) (searched 18 January 2023) WHO International Clinical Trials Registry Platform (ICTRP) (www.who.int/ictrp/search/en/) (searched 18 January 2023);
The search strategies for CENTRAL, MEDLINE, EMBASE and PEDro can be found in Supplemental Digital Content 1A-D. There were no restrictions placed on publication date or language. We also searched the following clinical trial registries for ongoing studies:
Clinical experts were contacted, and reference lists were screened for ongoing and unpublished studies.
Assessment of Risk of Bias
Two reviewers (ORO and MH) independently assessed the risk of bias of each eligible reported outcome in an included RCT using the Cochrane Collaboration's Risk of Bias 2 tool. 21 The risk of bias in non-randomized studies was assessed using the ROBINS-I tool. 22
Measure of Treatment Effect and Data Synthesis
We presented mean differences with 95% confidence intervals for continuous data. When available, we extracted post-intervention values with standard deviations from each group. Summary estimates were calculated using inverse-variance random effects (DerSimonian-Laird). A narrative synthesis was conducted when meta-analysis was not possible or appropriate. We imputed missing data according to methods outlined in the Cochrane Handbook. 23
Assessment of Heterogeneity
Between study statistical heterogeneity was assessed using visual inspection of the forest plot, Chi2 test and the I2 statistic. We considered P < 0.1 as statistically significant for Chi2 test. I2 was interpreted as ‘might not be important’ (0% to 40%), ‘moderate’ (30% to 60%),'substantial’ (50% to 90%) or ‘considerable’ (75% to 100%). 23
Subgroup and Sensitivity Analysis
Subgroup analysis based on the operative technique used was planned. Additionally, we planned to carry out sensitivity analyses to explore the contribution of high-risk studies by removing studies considered high-risk of bias.
Methods for Certainty of Evidence
Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to summarize the quality of evidence by outcome as high, moderate, low, or very low. All outcomes included in this review are presented separately in a summary of findings table (Table 1). The results of RCTs and non-randomized studies are shown separately. The GRADE manual guided decisions around evidence certainty. 24 GRADEpro Guideline Development Tool was used to develop the summary of findings tables (GRADEpro GDT: GRADEpro Guideline Development Tool [Software]. McMaster University, 2015 (developed by Evidence Prime, Inc.). Available from gradepro.org).
Summary of Findings Table.
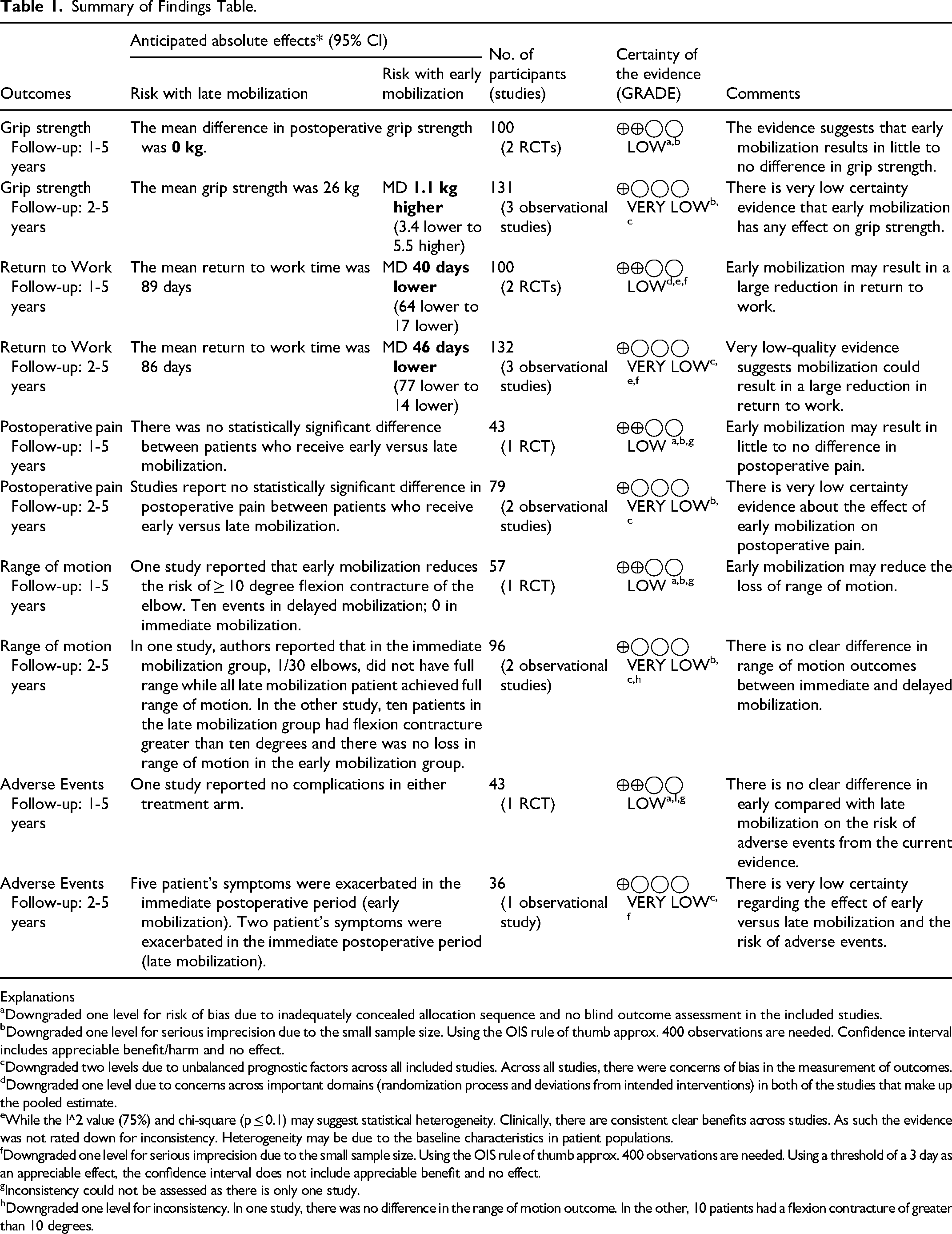
Explanations
Downgraded one level for risk of bias due to inadequately concealed allocation sequence and no blind outcome assessment in the included studies.
Downgraded one level for serious imprecision due to the small sample size. Using the OIS rule of thumb approx. 400 observations are needed. Confidence interval includes appreciable benefit/harm and no effect.
Downgraded two levels due to unbalanced prognostic factors across all included studies. Across all studies, there were concerns of bias in the measurement of outcomes.
Downgraded one level due to concerns across important domains (randomization process and deviations from intended interventions) in both of the studies that make up the pooled estimate.
While the I^2 value (75%) and chi-square (p ≤ 0.1) may suggest statistical heterogeneity. Clinically, there are consistent clear benefits across studies. As such the evidence was not rated down for inconsistency. Heterogeneity may be due to the baseline characteristics in patient populations.
Downgraded one level for serious imprecision due to the small sample size. Using the OIS rule of thumb approx. 400 observations are needed. Using a threshold of a 3 day as an appreciable effect, the confidence interval does not include appreciable benefit and no effect.
Inconsistency could not be assessed as there is only one study.
Downgraded one level for inconsistency. In one study, there was no difference in the range of motion outcome. In the other, 10 patients had a flexion contracture of greater than 10 degrees.
Results
There were five studies identified that met the inclusion criteria. These included two RCTs,25,26 one prospective observational study, 27 and two retrospective observational studies.28,29 No additional records were found through other sources. Figure 1 highlights the results of the comprehensive literature search. For the outcomes, postoperative pain, range of motion, and adverse events, statistical synthesis of data from more than one study was not possible. Hence, we performed a narrative review of the eligible studies. The unit of analysis was an individual's elbow, and there were no studies that randomized each elbow to a different intervention.
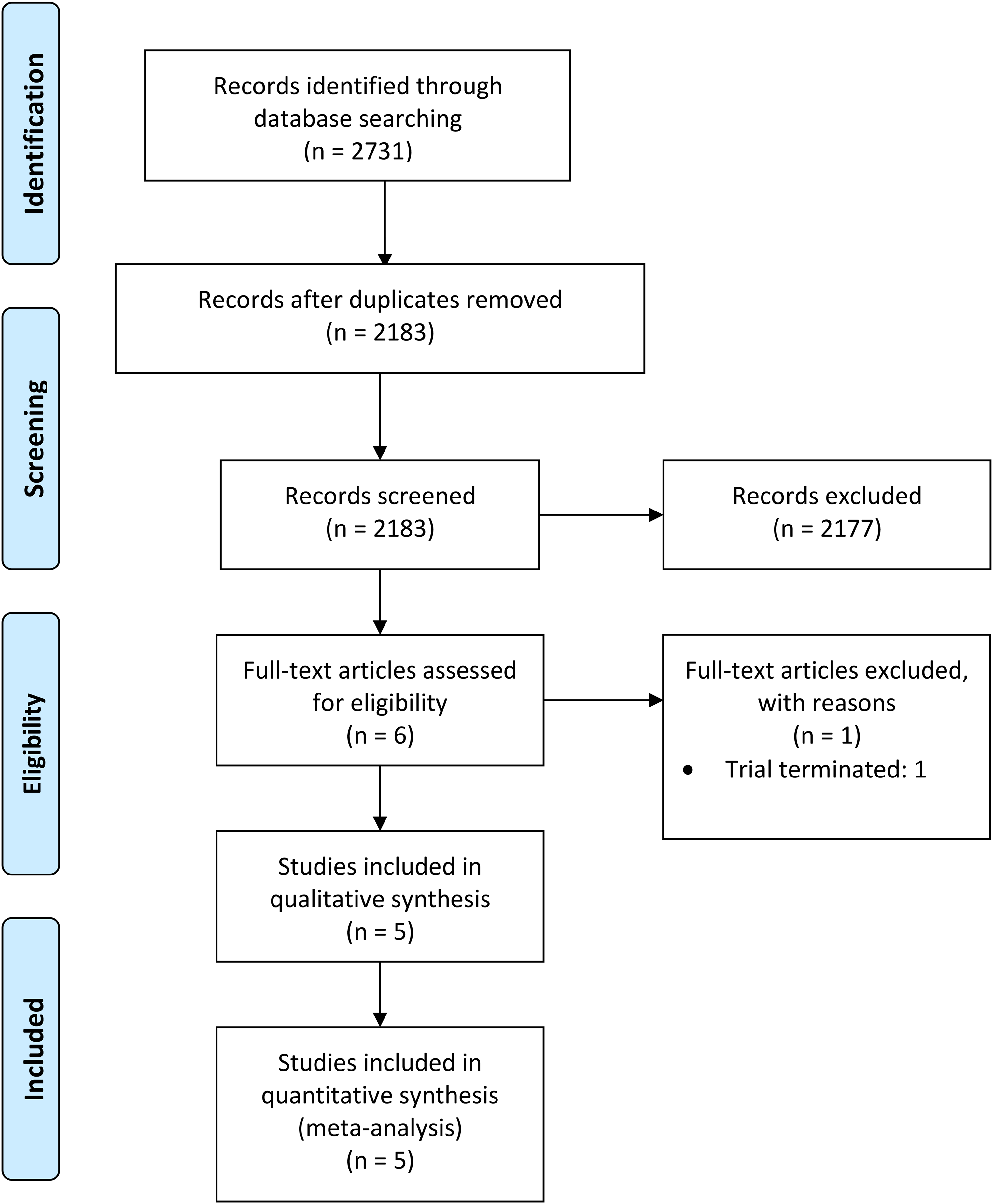
Study flow diagram.
Description of Studies
All the included studies were published over ten years prior to this systematic review (1993-2006).25–29 The majority of the trials25,27–29 (four of five) were conducted in the United States, and one 26 in China. All studies compared early mobilization (postoperative day zero to three) to delayed mobilization after cubital tunnel release surgery. In the RCTs,25,26 51 elbows were randomized into early mobilization and 49 elbows received delayed immobilization. In the observational studies (or Non-Randomized Studies of Interventions; NRSI),27–29 70 elbows underwent early mobilization and 62 patients received delayed mobilization. Study methodology details are described in Table 2. The definition of immediate immobilization differed between studies. Patients who underwent delayed mobilization of the elbow were immobilized for an average of two weeks (range: one to four weeks). Immobilization procedures included the use of a sling, plaster splints or casts. When reported, follow-up time varied from six months to five years. Regarding surgical approach, two studies26,29 reported performing a cubital tunnel release with medial epicondylectomy and three studies25,27,28 reported performing superficial anterior transposition of the ulnar nerve. While the rehabilitation exercises’ intensity and frequency were not fully reported in each trial, four of five studies described implementing active range of motion exercises postoperatively in both treatment arms.25,27–29 One trial 26 reported ‘mild and gradual strengthening’. The inclusion and exclusion criteria were consistent across studies; details for each study are presented in Supplemental Digital Content, Table 1.
Summary of the Data Provided by Each Study Regarding Measured Outcomes.
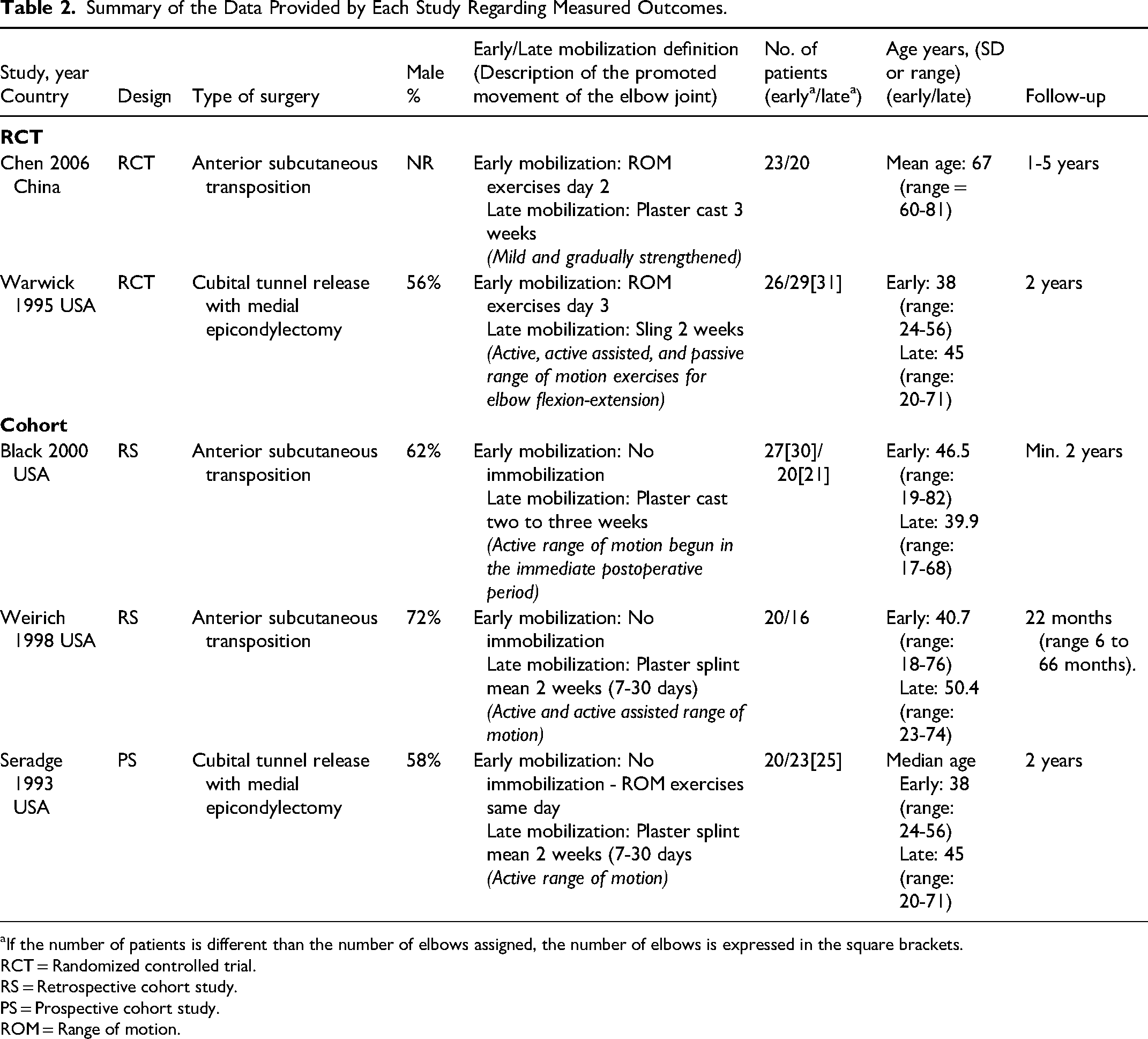
aIf the number of patients is different than the number of elbows assigned, the number of elbows is expressed in the square brackets.
RCT = Randomized controlled trial.
RS = Retrospective cohort study.
PS = Prospective cohort study.
ROM = Range of motion.
Risk of Bias
Risk of bias assessment of included studies is presented in Figure 2. Across the included studies, each outcome was at high-risk of bias for at least one domain. The investigators of the two RCTs failed to adequately describe their randomization process. Considering both studies’ size and overall quality, the randomization procedures was hypothesized to be inadequate. The risk of performance bias was concerning for the return to work outcome. There were very serious concerns of risk of bias in the three included observational trials due to confounding; secondary to imbalances of various baseline characteristics such as age, gender, and hand dominance. Detailed comments to support each decision are presented in Supplemental Digital Content, Table 2A–E.
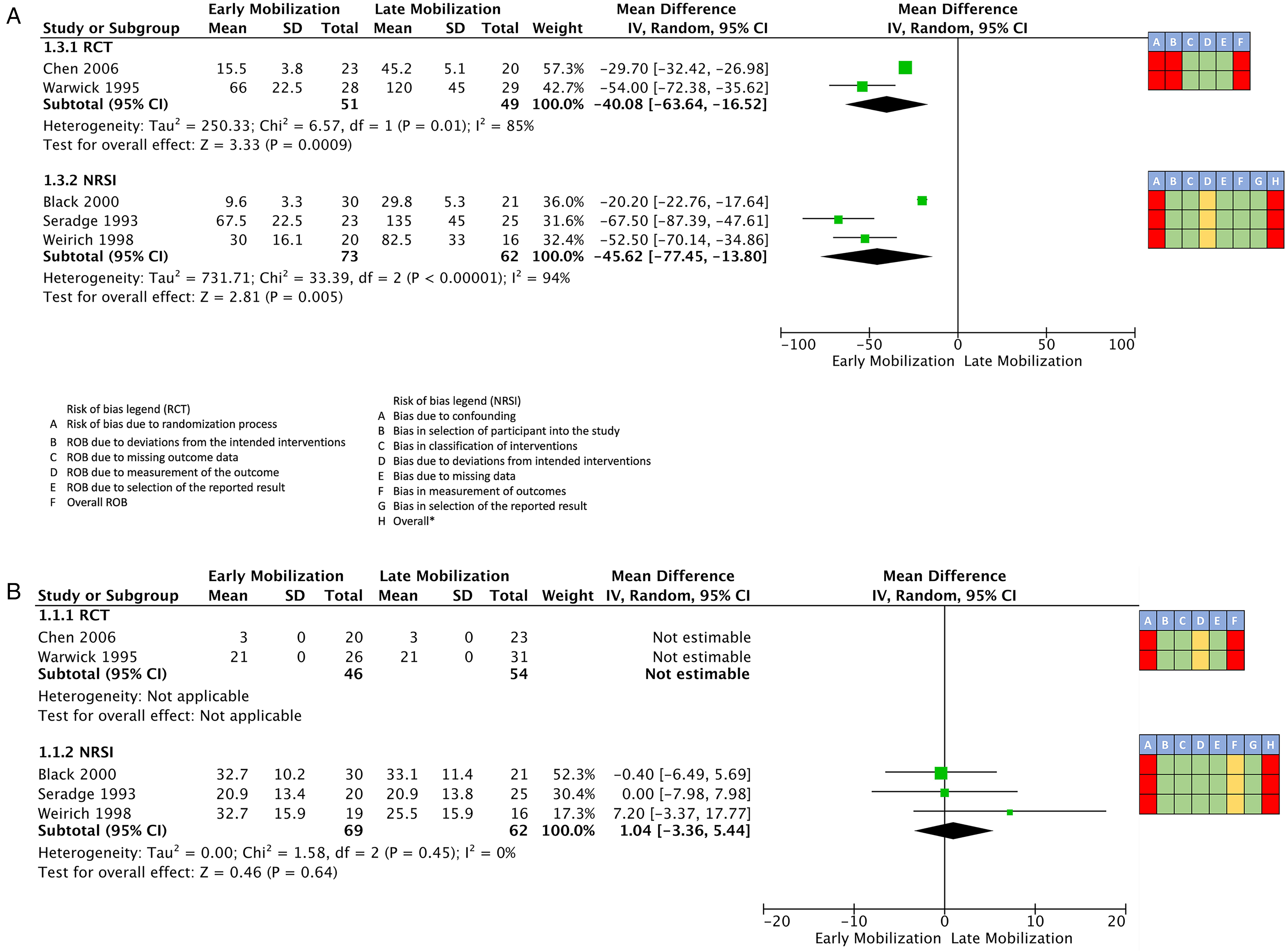
Forest plots of comparison of early mobilization versus late mobilization.
Effects of Interventions
The forest plots of the pooled outcomes are presented in Figure 2.
Return to work
Both randomized controlled trials reported data on the outcome: return to work (Figure 2A). The meta-analysis of the two RCTs (100 patients)25,26 showed immediate mobilization might result in a considerable reduction in return to work time over delayed immobilization (mean difference 40.1 days, 95% confidence interval [CI] 63.6-16.5 days earlier, I2 85%, low certainty). The pooled results of the three observational studies (131 patients) suggests that early mobilization could reduce the number of days to return to work (mean difference 45.6 days, 95% CI 77.4-13.8 days earlier, I2 = 94%, very low certainty).
Grip strength
Each of the included studies reported data on postoperative grip strength (Figure 2B). The two RCTs (100 patients)25,26 demonstrated a mean difference of zero kilograms in postoperative grip strength between the two interventions (low certainty). In the included observational studies, the mean difference in grip strength was 1.04 kilograms (MD 1.04 kg, 95% CI = -3.4 to 5.4 kg, I2 = 0%, very low certainty). RCT evidence was rated low certainty (downgraded once for risk of bias and once for imprecision). NRSI evidence was rated very low certainty (downgraded twice for risk of bias in multiple domains and once for imprecision). The evidence suggests that early mobilization may results in little to no difference in grip strength.
Postoperative pain
Two observational studies (79 patients)27,28 and one RCT (43 patients) 25 reported summarized outcome data on postoperative pain. The visual analogue scale was used in two studies,25,27 and one study 28 used a standardized outcome questionnaire. There were no differences reported in pain between the early and delayed immobilization treatment groups in all three studies. The RCT evidence was rated low certainty, downgraded once for risk of bias and once for imprecision. The NRSI evidence was rated very low, downgraded two levels for risk of bias in several domains and one level for imprecision.
Range of motion
Three studies provided data on postoperative elbow range of motion. Warwick and Seradge 25 found that 13 of 31 elbows in the delayed mobilization group sustained flexion contractures greater than ten degrees (none of 26 elbows in the early mobilization group). In the included observational studies, Seradge et al 27 had no episodes of contractures of the 26 elbows in the early mobilization group and 10 of 25 elbows sustained flexion contractures greater than ten degrees in the delayed mobilization group. Black et al 29 reported that none of the 21 patients in the late mobilization group sustained decreased ROM, and 1 of 30 patients in the early mobilization group lost twenty degrees of terminal extension. The two observational studies were not pooled, as the endpoints used to define elbow contractures were different. RCT evidence was considered low certainty evidence, rated down once for risk of bias and once for imprecision. Observational evidence was assigned very-low certainty evidence, and was rated down twice for very serious risk of bias and once for imprecision. Thus, early mobilization may improve range of motion.
Adverse events
Two studies reported adverse outcome data. In their RCT investigation, Chen et al 26 (43 patients) reported no differences in abnormal wound bleeding, hematoma, and delayed wound healing between the intervention groups. In their observational study, Weirich et al 28 (36 patients) reported that 5 of 20 patients in the early mobilization group had symptom exacerbation with 2 of 16 in the delayed mobilization group, and there was no difference in operation failure requiring a subsequent ulnar nerve procedure. Low certainty RCT evidence (downgraded once for risk of bias and once for imprecision) suggests that immediate mobilization may results in little to no difference in adverse events. Evidence from the observational study was rated down twice for serious risk of bias in a few domains, and for imprecision, as it provides very low-certainty evidence about the effect of early mobilization on adverse events.
Sensitivity and subgroup analysis
We performed a sensitivity analysis for all pooled outcomes with missing data. Across all the analyses, there was no meaningful statistical or clinical difference in the pooled effect estimate irrespective of the imputed SD (Supplemental Digital Content, Figures 1 and 2). There were insufficient data to perform a subgroup analysis based on the operative technique, or to investigate heterogeneity statistically. There were also insufficient high-quality studies to conduct a sensitivity analysis removing the high-risk of bias studies.
Discussion
Summary of Main Results
There were five studies - two RCTs and three observational studies - investigating early mobilization effectiveness compared to late mobilization after cubital tunnel release surgery. RCT and observational evidence suggest that early mobilization may reduce the number of days required for patients to return to work and may also reduce the incidence of decreased range of motion in the elbow. Moreover, our results, albeit having a low certainty of evidence, demonstrated that patients who were mobilized for shorter periods, or had no immobilization, had no difference in postoperative pain scores. In addition, there was no difference in adverse events between the two groups. The results of the meta-analysis suggests that the practice of prolonged immobilization does not appear to improve postoperative pain, incidence of adverse events, or recovery time. Furthermore, studies suggest that prolonged immobilization results in unnecessary loss of work productivity for patients and society. Our study highlights that splinting longer than 72 hours may not provide any clinical benefit.
This study has demonstrated that splinting leads to significant delays, with an average increase of 40 days in the timing of return to work. The exact reason for the observed impact of splinting on return to work is challenging to elucidate. It is possible that there were additional factors related to immobilization that were not adequately addressed in the studies. Patients who underwent immobilization may have experienced delays in returning to work due to stiffness or other complications associated with splinting. Moreover, the studies exhibited significant heterogeneity within the same intervention (early mobilization), resulting in a wide range of return-to-work durations - spanning from 16 to 66 days. Although there is unexplained heterogeneity among the sampled patients, it is consistent across multiple studies that splinting has a statistically and clinically meaningful adverse effect on return to work, suggesting that it is likely to be detrimental in this context.
In addition, to the authors' knowledge, there are no previous, published, systematic reviews comparing early to late mobilization after cubital tunnel surgery. However, the literature around carpal tunnel decompression shows that there is no beneficial effect from post-operative immobilization after decompression when compared to early mobilization.12,13 Furthermore, Harding et al 15 presented a systematic review comparing early versus delayed elbow mobilization after elbow fracture in adults, finding minimal differences in pain and range of motion, which is similar to our study. However, their review did not identify studies that reported return to work or grip strength outcomes.
Overall Completeness, Applicability, and Quality of Evidence
The included studies in our analyses exclusively assessed early versus late mobilization in patients who had ulnar nerve decompression. The inclusion criteria across the five studies were consistent, with all studies evaluating cubital tunnel release surgery patients. The postoperative immobilization approaches using plaster splints and casts for immobilization were consistent with standard clinical practices. The postoperative rehabilitation program was not reported in detail, but the majority (four of five25,27–29) of the studies were consistent in reporting that patients underwent active range of motion exercises postoperatively. Based on these observations, the results of the review can be generalized to the real-world clinical setting. This review's objective was to assess the effect of early versus delayed mobilization after cubital tunnel release, irrespective of surgical approach. In our systematic review, two of three main approaches were used. Although we conducted a comprehensive systematic review, we found a notable gap in the investigation of in situ decompression or decompression with anterior interosseous nerve transfer. As a result, the generalizability of our findings is not directly applicable to these specific patient populations. Given the limited efficacy of immobilization in cases involving more traumatic methods of ulnar nerve decompression, it is unlikely that prolonged immobilization would be effective following in situ decompression. The optimal rehabilitation of the upper extremity following nerve transfer remains a topic of ongoing debate.
Potential Biases in the Review Process
Due to publication dates, we did not attempt to contact study authors regarding missing study data or information concerning to potential risk of bias. The risk of publication bias was reduced by attaining translation of studies not published in English and search trial registries. The mean and standard deviation were estimated from the median values and the IQR for grip strength in one study 29 and return to work in two studies.25,27 Additionally, in two studies (Seradge et al, 27 grip strength; and Weirichet et al, 28 return to work), insufficient data allowed for the estimation of standard deviation directly from the study. As such, it was inputted using the pooled variance of the other studies. RCT data could not be pooled for grip strength because there was insufficient data to impute the SD estimates. Each estimation involved making assumptions about the underlying statistics.
Implications for Practice
Early mobilization may improve outcomes in patients undergoing cubital tunnel release surgery compared to delayed mobilization, as indicated by the earlier return to work. There is low and very low-certainty evidence to suggest little to no effect on the rate of adverse events and postoperative pain.
Implications for Research
Considering cubital tunnel is the second most common entrapment neuropathy, there is an urgent need for randomized trials with adequate randomization procedures. A multicenter study would be essential to replicate both surgical and rehabilitation practices’ heterogeneity to determine which intervention results in better outcomes related to function, pain, and adverse events. In the future, reliable and validated upper extremity quality of life measures should be used to identify which intervention results in superior patient-reported outcomes. Future research should also consider the cost-effectiveness of early mobilization from a societal perspective.
Supplemental Material
sj-docx-1-psg-10.1177_22925503231201631 - Supplemental material for Immediate Versus Delayed Mobilization After Cubital Tunnel Release Surgery: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-psg-10.1177_22925503231201631 for Immediate Versus Delayed Mobilization After Cubital Tunnel Release Surgery: A Systematic Review and Meta-analysis by Oluwatobi R. Olaiya, Minh Huynh, Tega Ebeye, Lucas Gallo, Lawrence Mbuagbaw and Matthew McRae in Plastic Surgery
Footnotes
Author Contributions
ORO developed the research question and protocol, conducted data analysis, drafted the manuscript, and assisted with the review and editing. MH and TE reviewed articles and assisted with editing. LG, LM and MR provided guidance with regards to data analysis, writing and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
This article did not directly utilize human or animal subjects.
Informed Consent
This article did not directly utilize human subjects.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.