
Abstract
Introduction
Access to accurate population-level burden of disease data is important for understanding causes of morbidity and mortality. To date, there has not yet been a comprehensive cross-sectional analysis of the morbidity and mortality of plastic and reconstructive surgery related diseases in Canada. Given that disease burden can inform public health policy and direct research funding, understanding the burden of plastic surgery related diseases in Canada is a critical step in advancing patient care.
The Global Burden of Disease Study (GBD) is an international collaboration through the Institute for Health Metrics and Evaluation (IHME) that generates a systematic and internally consistent source of health information.1‐4 This effort enables quantification of comparative health loss categorized by disease pathology, demographics, geographic region, and time.3‐5 The goal of the IHME is to provide an impartial, evidence-based picture of global health trends to inform the work of policymakers, researchers, funding agencies, and to guide population-level health initiatives.
For the Global Burden of Disease Study 2019 (GBD 2019) 369 diseases, including 13 relevant to plastic surgery, were estimated.3,4,6 In this paper, we present a cross-sectional analysis of the Canadian GBD 2019 results on mortality, morbidity, incidence, prevalence, and economic cost for all 13 diseases related to plastic and reconstructive surgery.
Methods
The goal of the GBD study is to produce the highest quality epidemiologic data by ensuring transparent analytic strategies that include uncertainty distribution. Each update incorporates new studies and methodologies to further refine the available data thereby generating a “living database.” The GBD 2019 methodology has been extensively described in the original study publications.4,6‐9
We used GBD 2019 results to assess the morbidity, mortality, incidence, and prevalence of plastic and reconstructive surgery related diseases in Canada. Rates and numbers of deaths, incident cases and prevalence, years of life lost (YLLs), years lived with disability (YLDs), and disability-adjusted life years (DALYs) are generated for each disease and injury, with each metric reported by year, location, age group, and sex.4,10 The GBD world standard population is used as a reference for calculating age-standardized YLD, YLL, and DALY rates.4,11,12 The data is analyzed using a Bayesian meta-regression modelling tool to provide epidemiological estimates of YLLs, YLDs, and DALYs by combining other available parameters.2,4,10 The width of the uncertainty interval (UI) is calculated through Bayesian estimation methods to reflect data availability, sample size, and consistency of data across multiple sources.3,4,10
In this paper, incidence, prevalence, YLLs, YLDs, and DALYs, are reported here for both sexes combined and for all age groups in Canada, as rates per 100 000 and as counts. 95% UI are reported in square brackets for all estimates (except for totals) and includes all sources of uncertainty (ie, systematic biases, measurement error). GBD is conducted in accordance with the Guidelines for Accurate and Transparent Health Estimates Reporting.3,13,14
Data Sources
The GBD 2019 estimates cover the years 1990 to 2019 and are drawn from more than 90 000 data sources. Data collected for the GBD 2019 is collected from multiple relevant data sources for each disease including vital statistics, disease registries, health service use, and disease notifications—identified from a systematic and thorough review of published studies, searches of government and international organization websites, published reports, and primary data sources such as surveys and population-based registries.3,4,12,15‐17 For each iteration of GBD, the estimates for the whole time series are updated from the addition of new data and change in methods and based on an analytical framework. The GBD uses the International Classification of Diseases (ICD) for maximum comparability between diseases worldwide. For Canada, disease registries maintained by each province and data from the national census account for the majority of available data. Further information on Canadian data sources can be found online at the Global Health Data Exchange: http://ghdx.healthdata.org/geography/canada.
Classification of Plastic and Reconstructive Surgery Diseases
Data for 13 plastic surgery associated conditions were selected from the GBD 2019. These conditions were defined by the ninth and tenth revision codes of the ICD. 18 The conditions included were as follows: (1) breast cancer, (2) cellulitis, (3) decubitus ulcer, (4) pyoderma, (5) fire, heat and hot substances, (6) malignant skin melanoma, (7) squamous cell carcinoma, (8) basal cell carcinoma, (9) neoplasms of the lip and oral cavity, (10) neoplasms of the nasopharynx, (11) larynx cancer, (12) other pharynx cancer, and (13) orofacial clefts. The treatment of these conditions (especially breast cancer and melanoma) is not solely in the domain of plastic and reconstructive surgery, however, Canadian plastic surgeons contribute significantly to their management. Due to the limitations of the GBD classification it was not possible to select for traumas or upper extremity injuries/diseases—conditions for which plastic surgeons contribute significantly.
Definitions
The IHME defines incidence as the number of new cases of a given disease during a given period in a specific population whereas prevalence is the total number of cases of a given disease in a specific population at a designated time. Outcomes are reported here as both all-age and age-standardized values. Age-standardizing is a statistical technique which transforms the age characteristics of a specific population to match a reference population (ie, GBD 2019 World Standard Population), to allow comparisons with different age structures. All-age rates or counts do not have this correction done and so there are limitations to comparing these results to other populations or other points in time.
Cause of Death
The GBD study attributes cause of death to a single disease that initiated the ultimate cause of death with coding following ICD-10 principles. The GBD cause of death hierarchy is divided into 4 levels: Level 1 represents all-cause mortality, Level 2 represents cause-group mortality (ie renal disease), Level 3 represents cause-specific mortality, and Level 4 represents further specified diseases such as drug-resistant tuberculosis. 19 In this paper, we used Levels 3 and 4 to assess YLLs and mortality for applicable diseases.
Mortality and YLLs
All applicable diseases have age-specific mortality data. The GBD uses the Cause of Death Ensemble model 19 to predict age- and sex-specific mortality estimates by cause. Mortality-to-incidence ratios are used to transform registry incidence data to mortality estimates, in order to maximize data availability in locations with scarce mortality information. YLLs are calculated as a measure of cause-specific premature mortality. Given that the GBD attributes cause of death to a single disease, basal cell carcinoma does not have an attributable mortality rate.
Years Lived With Disability
GBD 2019 uses the Disease Modeling Meta-Regression 2.1 (DisMod-MR 2.1) to calculate prevalence for each disease while considering data on incidence, remission, mortality, and disease duration.4,9,20 Prevalence estimates gathered by the GBD are multiplied by disability weights to calculate cause-specific YLDs.4,9
Disability-Adjusted Life Years
Morbidity is assessed using DALYs which represents the sum of YLLs and YLDs; one DALY is equivalent to 1 year of healthy life lost due to premature mortality or disability.3,21 In the GBD, DALYs are the preferred metric used to compare disease burden across time and geography and between age and sex groups.
Economic Analysis
Given that the economic health of a nation is correlated to the overall disease burden,22‐24 we assessed the economic cost of disease using DALY rates as described in prior publications.25,26 With increasing DALYs rates, a country's Gross National Income per capita decreases in a logarithmic fashion. 22 As such, the economic burden of disease can be approximated by accounting for the loss in Gross Domestic Product per capita due to disease-specific DALYs.27,28To quantify and compare the costs of adverse health end points, the monetary value of a DALY can be ascertained based on previous analysis.27,28 While no official consensus of the appropriate value of a DALY has been established, a conversion based on the Value of Life Year has also been suggested. 29 Different economic values of DALYs have been allocated per income country group level, as defined by the World Bank. 30 A cost per DALY was recently estimated as $50,000 for Canada as a whole and is likely to be similar across most provinces. 30 This value can be used to approximate total cost of a disease by multiplying age standardized DALY rates by the Canadian population of 38 million in 2019 according to census data. 31
Results
Prevalence and Incidence
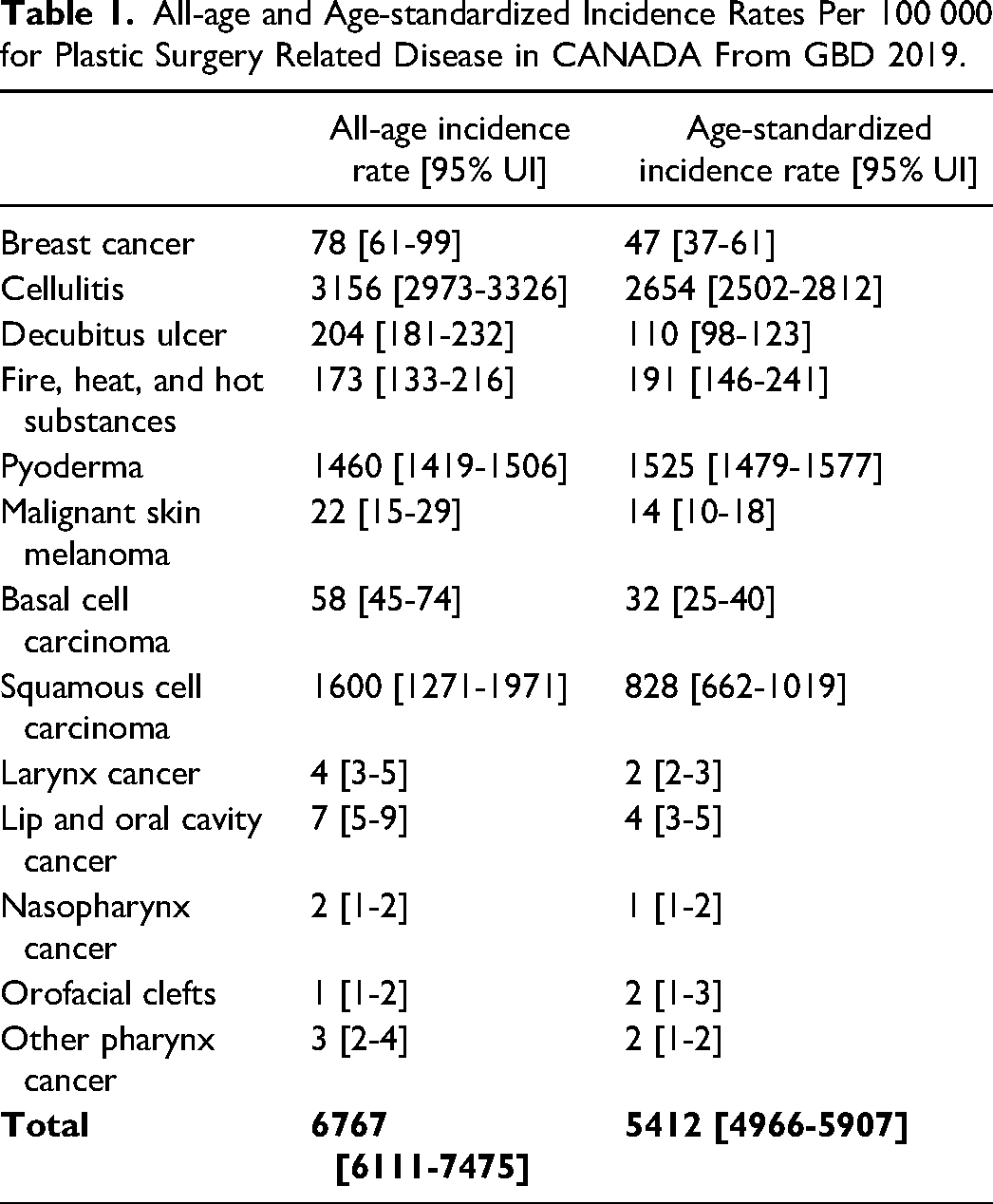
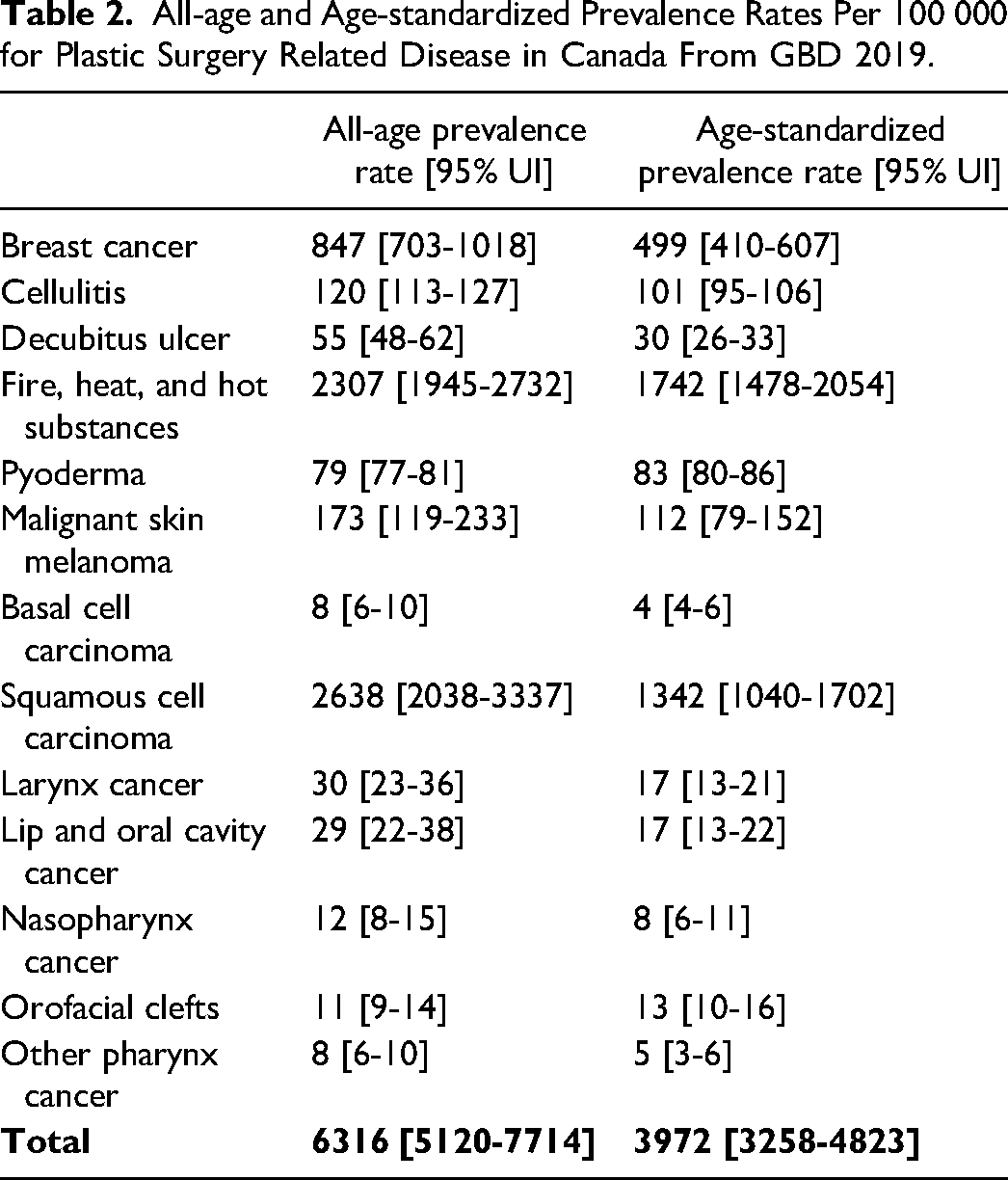
In 2019, plastic surgery related conditions in Canada had an overall age-standardized incidence rate of 5412 per 100 000 [95% UI 4966-5907] (Table 1), and an overall all-age standardized prevalence rate of 3972 per 100 000 [3258-4823] (Table 2). Cellulitis had the highest incidence with an age standardized rate of 2654 per 100 000 [2502-2812] followed by pyoderma (1525 per 100 000 [1479-1577]). Fire, heat, and other hot substances had the highest age-standardized prevalence rate (1742 per 100 000 [1478-2054]) with a relatively low age-standardized incidence rate of 191 per 100 000 [146-241]. Breast cancer had an age-standardized incidence rate of 47 per 100 000 [37-61] and an age-standardized prevalence rate of 499 per 100 000 [410-607]. The age-standardized incidence rates of non-melanoma skin cancers combined (basal cell carcinoma: 32 per 100 000 [25-40] and squamous cell carcinoma: 828 per 100 000 [662-1019]) had approximately 60 times greater incidence than malignant melanoma (14 per 100 000 [10-18]).
All-age and Age-standardized Incidence Rates Per 100 000 for Plastic Surgery Related Disease in CANADA From GBD 2019.
All-age and Age-standardized Prevalence Rates Per 100 000 for Plastic Surgery Related Disease in Canada From GBD 2019.
Mortality and YLLs
In 2019, plastic surgery related conditions in Canada had an overall all-age death count of 11,411 [95% UI 9568-12,827] and an age-standardized death rate of 17 per 100 000 [14-19] (Table 3). All-age YLL count was 238,731 [206,951-266,194] and age-standardized YLL rate was 409 per 100 000 [357-457] (Table 4). Breast cancer overwhelmingly contributed to mortality with an age-standardized death rate of 10 per 100 000 [9-11]) and an age-standardized YLL rate of 233 per 100 000 [215-250]. Melanoma was the second largest contributor to mortality with an age-standardized death rate of 2 per 100 000 [1-2] and an age-standardized YLL rate of 53 per 100 000 [38-67]. Of note, melanoma and breast cancer are not solely treated by plastic surgery. Fire, heat, and hot substances, lip and oral cavity cancer, larynx cancer, and cutaneous squamous cell carcinoma also significantly contributed to mortality and YLL in 2019 (Tables 3 and 4). Orofacial clefts had the lowest age-standardized death rate (0 per 100 000 [0-0]) and YLL rate (0 per 100 000 [0-0]).
All-age Death Count and Age-standardized Death Rate Per 100 000 for Plastic Surgery Related Disease in Canada From GBD 2019.
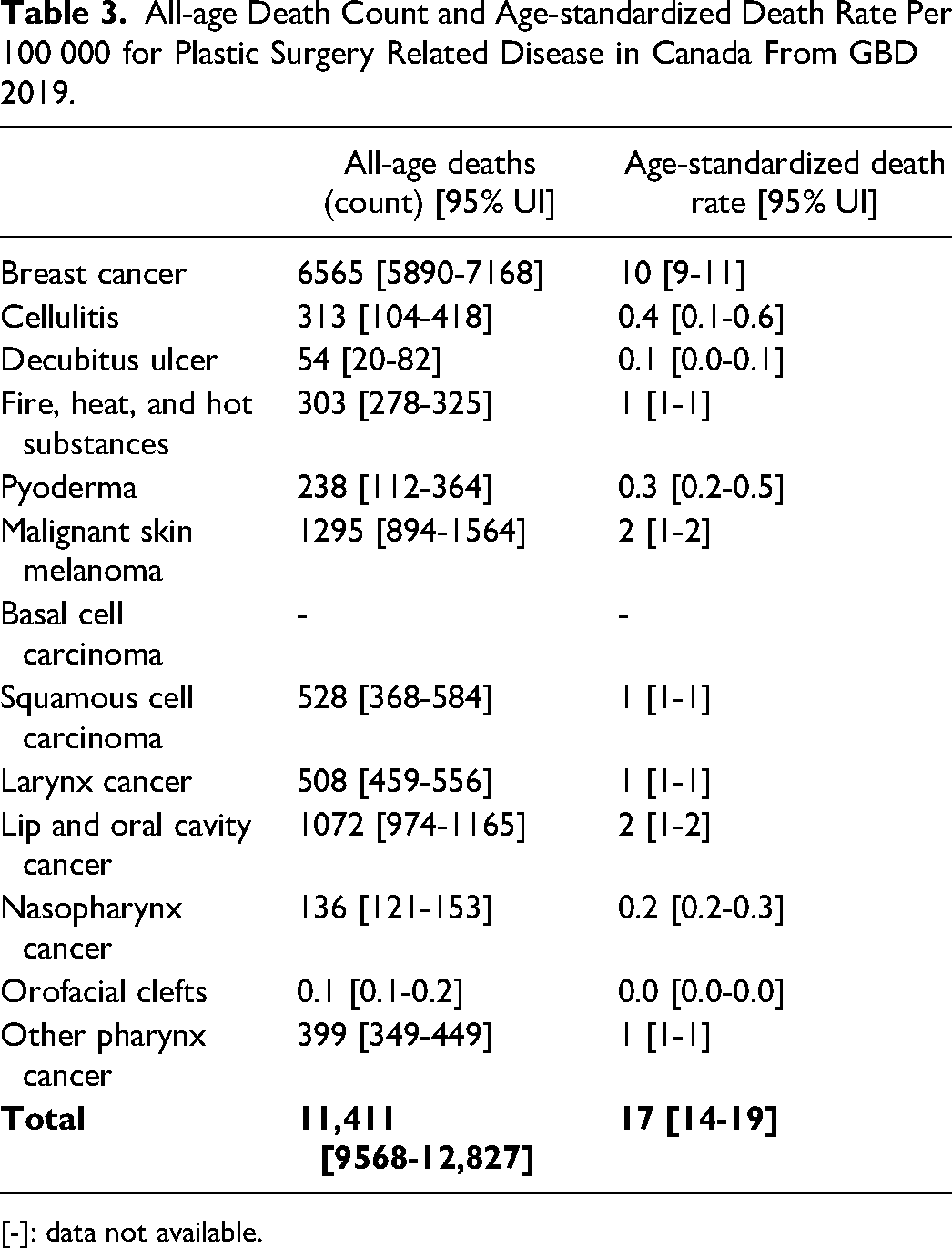
[-]: data not available.
All-age YLL Count and Age-standardized YLL Rate per 100 000 for Plastic Surgery Related Disease in Canada From GBD 2019.
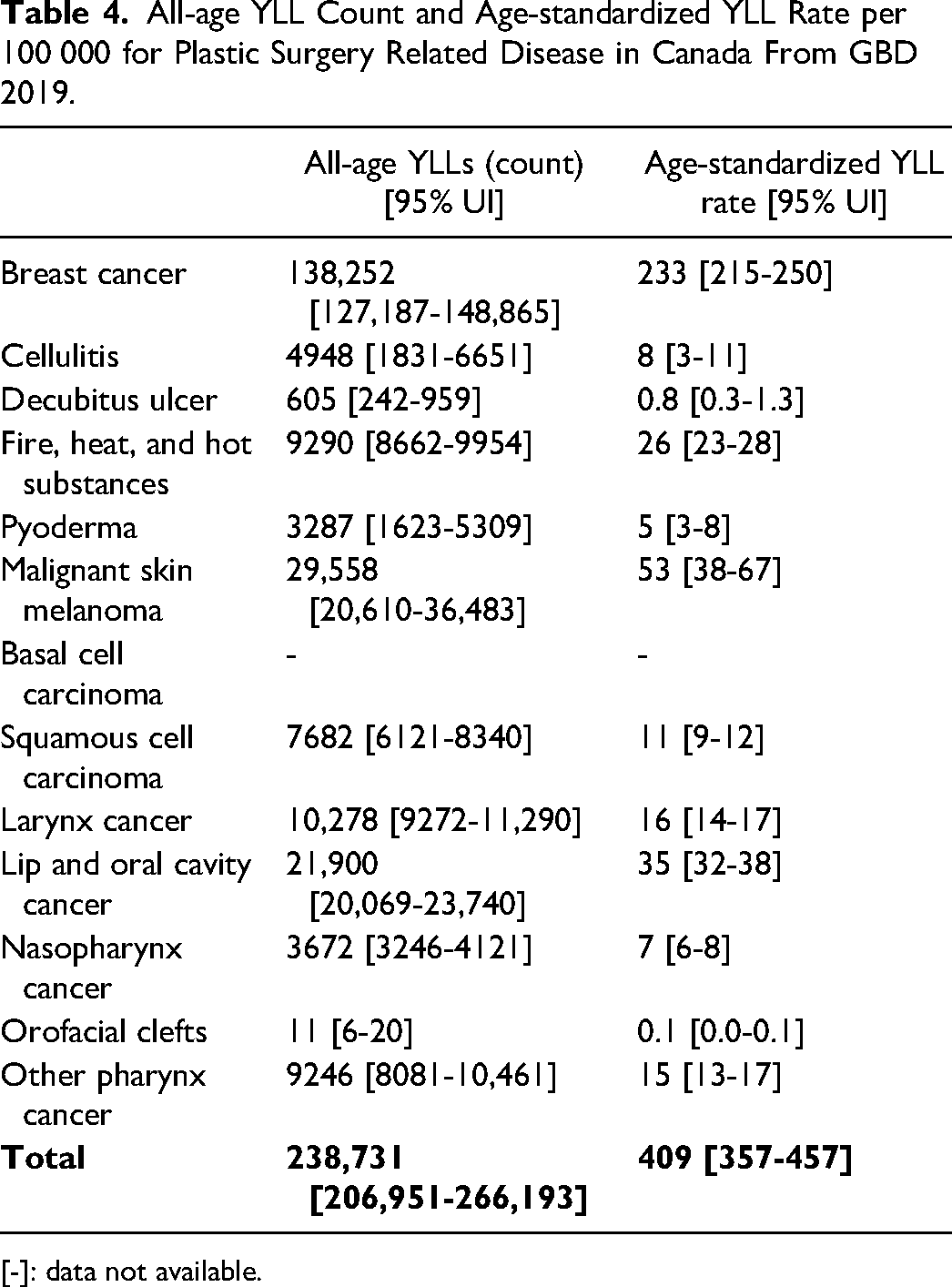
[-]: data not available.
Years Lived with Disability
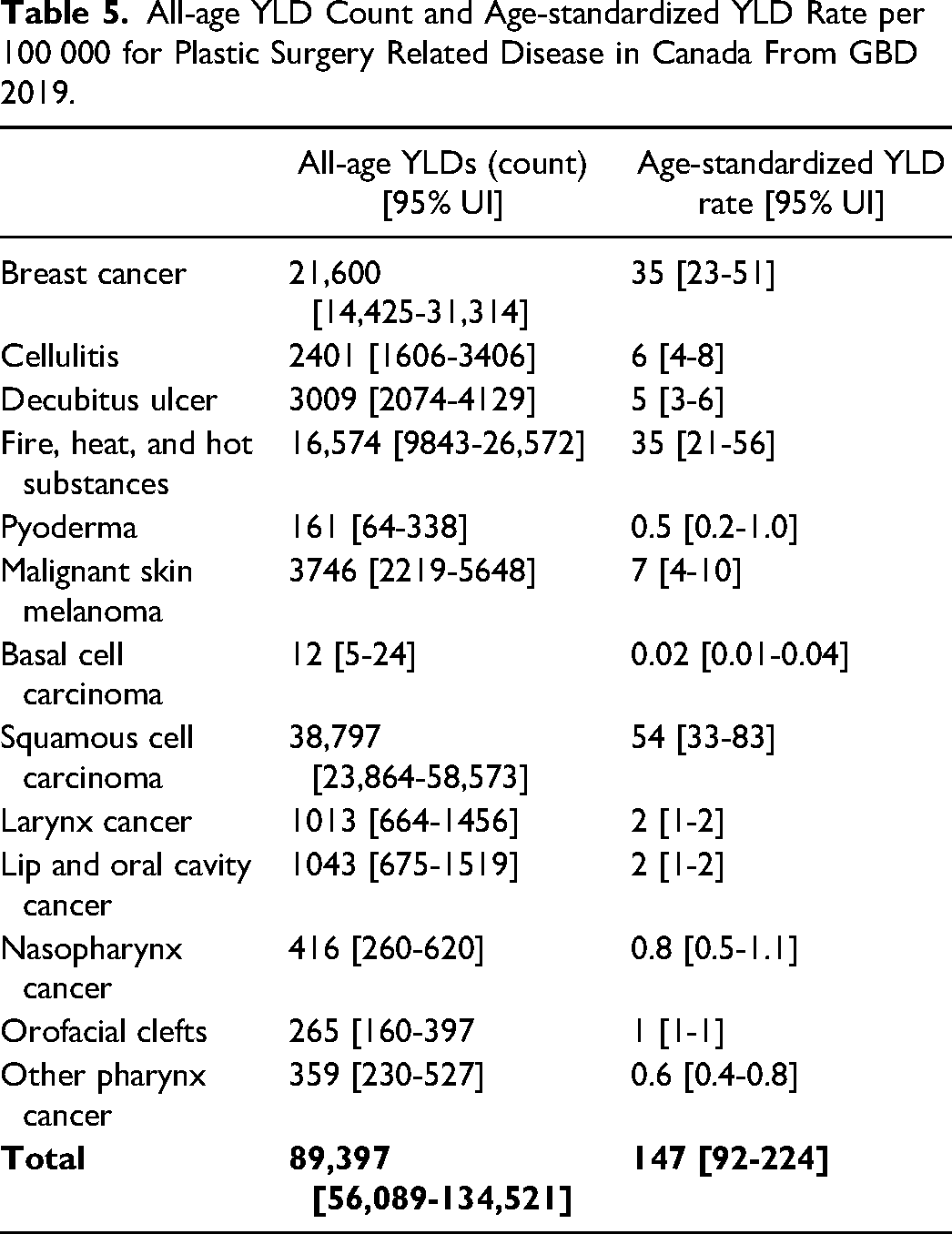
In 2019 in Canada, plastic surgery related conditions were responsible for an overall all-age YLD count of 89,397 [95% UI 56,089-134,521] with an age-standardized YLD rate of 147 per 100 000 [92-224] (Table 5). Squamous cell carcinoma had the highest age-standardized YLD rate (54 per 100 000 [33-83]) followed by fire, heat, and hot substances (35 per 100 000 [21-56]) and breast cancer (35 per 100 000 [23-51]).
All-age YLD Count and Age-standardized YLD Rate per 100 000 for Plastic Surgery Related Disease in Canada From GBD 2019.
Disability-Adjusted Life Years
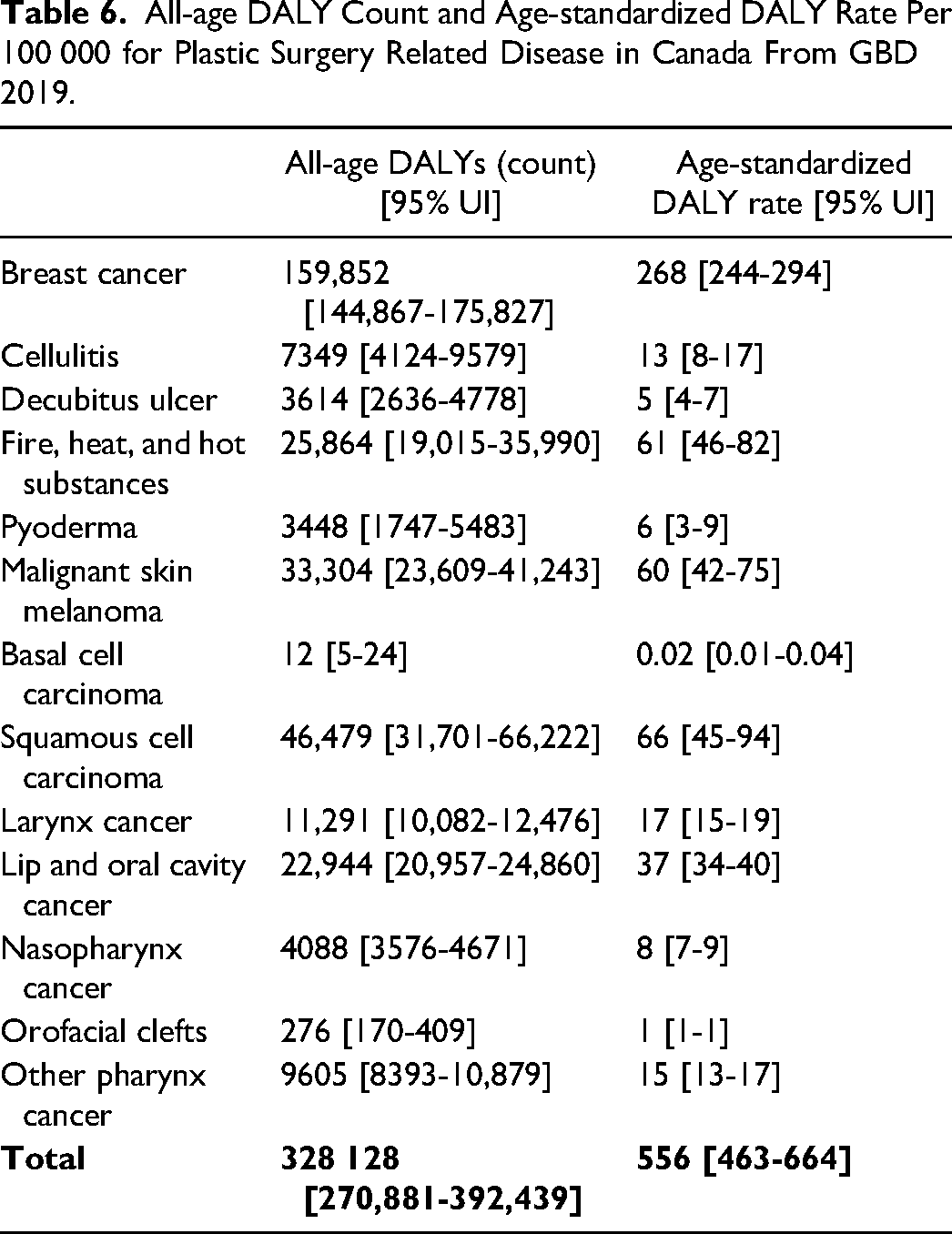
In 2019 in Canada, plastic surgery related conditions were responsible for an overall all-age DALY count of 328 128 [95% UI 270,881-392,439] with an age-standardized DALY rate of 556 per 100 000 [463-664] (Table 6). Breast cancer was responsible for the highest age-standardized DALY rate (268 per 100 000 [244-294]), followed by squamous cell carcinoma (66 per 100 000 [45-94]), fire, heat, and hot substances (61 per 100 000 [46-82]) and malignant skin melanoma (60 per 100 000 [42-75]). Diseases with lower age-standardized DALY rates include basal cell carcinoma (0.02 per 100 000 [0.01-0.04]), orofacial clefts (1 per 100 000 [1-1]), pyoderma (6 per 100 000 [3-9]), and decubitus ulcer (5 per 100 000 [4-7]). Figure 1 illustrates age-separated DALY rates per 100 000, illustrating the relatively higher proportion of DALY's due to the burden from fire, heat, and hot substances injury in ages 0-24, and the subsequent increase in DALY rate of other diseases including breast cancer, skin cancers, and fire, heat, and hot substances injuries.
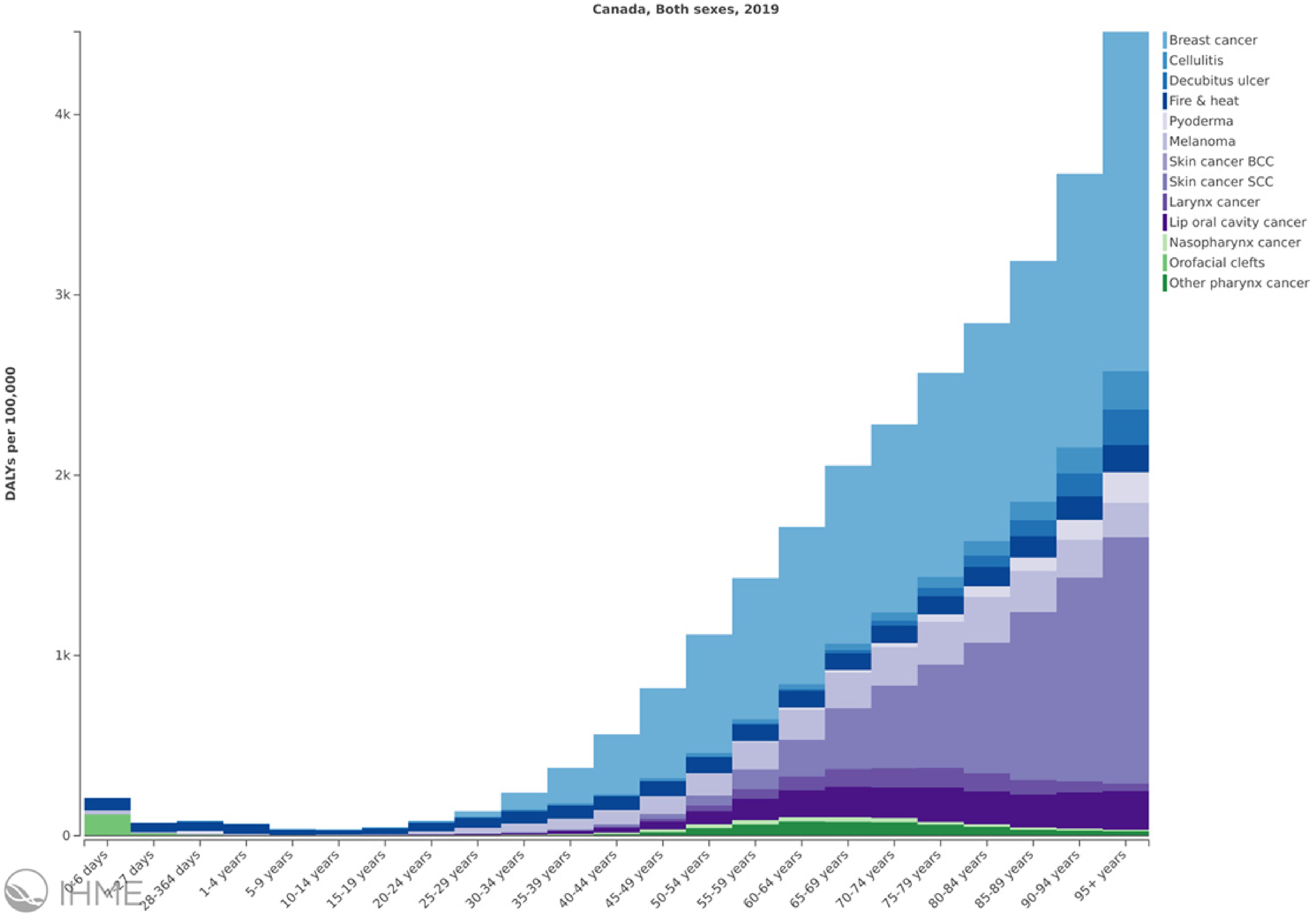
Age separated DALY rates per 100 000 for plastic surgery related disease in Canada from GBD 2019.
All-age DALY Count and Age-standardized DALY Rate Per 100 000 for Plastic Surgery Related Disease in Canada From GBD 2019.
Economic Analysis
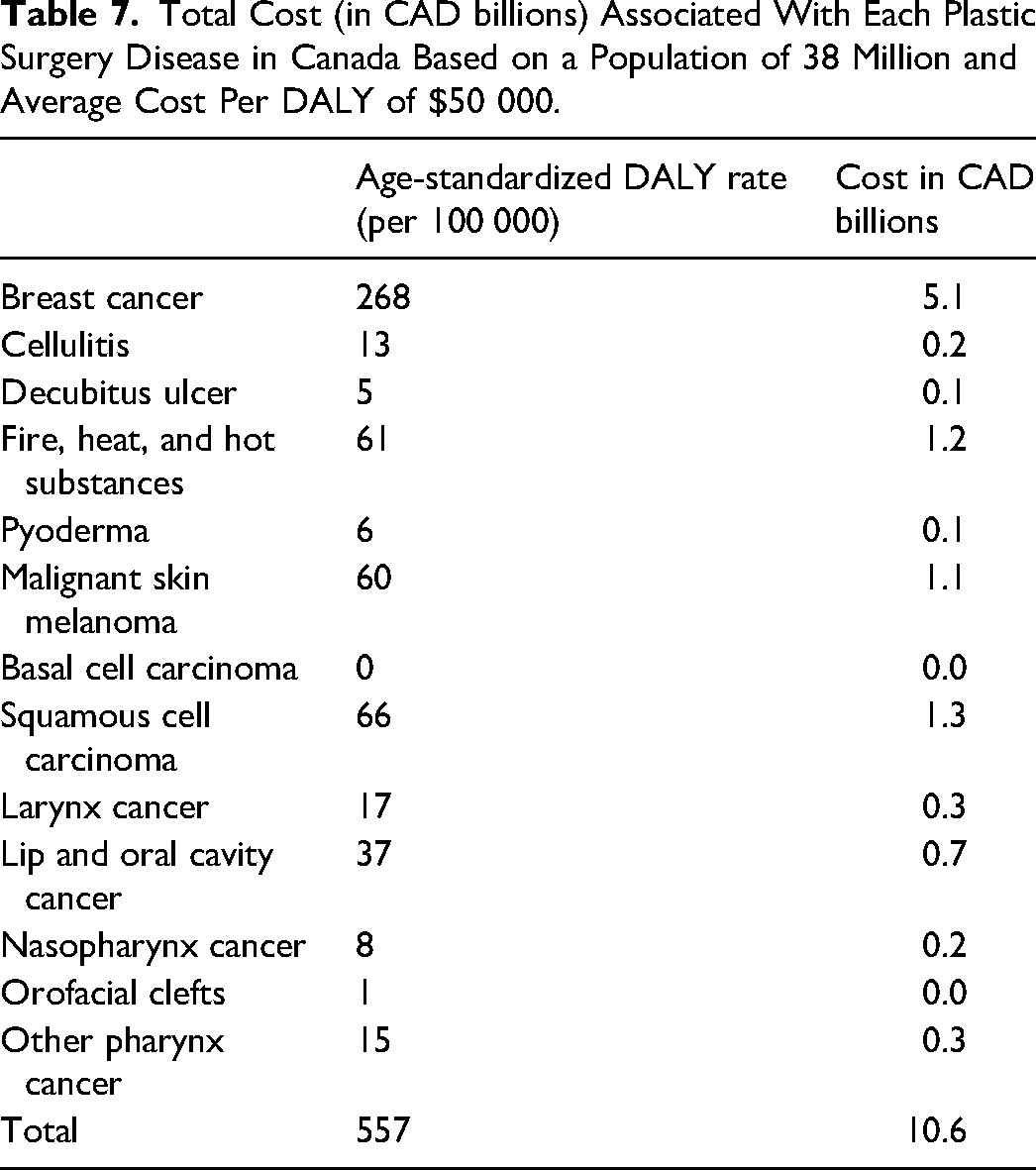
In Canada in 2019, the age-standardized economic burden of included plastic surgery related diseases was $10.6 billion (
Total Cost (in CAD billions) Associated With Each Plastic Surgery Disease in Canada Based on a Population of 38 Million and Average Cost Per DALY of $50 000.
Discussion
This study presents a comprehensive, cross-sectional analysis on the burden and economic cost of 13 plastic and reconstructive surgery related diseases in Canada for the year 2019. In Canada as of 2019, plastic surgery related diseases are responsible for an overall age-standardized cost of greater than $10 billion Canadian dollars (CAD) and represent 3% of all-age DALYs in Canada. This places plastic surgery related diseases 14th among all-cause, all-age DALYs in Canada, behind disease groups such as neoplasms, cardiovascular disease, and substance use disorders, and ahead of disease groups such as transport injuries, maternal and neonatal disorders, and respiratory infections and tuberculosis. Plastic surgery related diseases are the 16th leading cause of age-standardized DALY rates in Canada in 2019, behind transport injuries and digestive diseases and ahead of sense organ diseases and respiratory infections and tuberculosis. Of the plastic surgery related diseases included in this analysis, breast cancer was responsible for the largest burden of disease and had the highest mortality rates, with an associated cost of $5.1 billion CAD—representing approximately half of the $10.6 billion CAD total cost of plastic surgery related diseases in Canada in 2019.
With regards to YLLs, Canadians lost a cumulative 238,731 years of life due to plastic surgery conditions; equivalent to 409 years of life per 100 000 people in 2019. In terms of years spent in disability, plastic surgery conditions resulted in 89,397 years spent in disability (147 years lived in disability per 100 000 Canadians). When totaled together in cumulative as DALYs, there were 328 128 years were lost to disability or to mortality, or 556 years per 100 000 Canadians, due to plastic surgery related conditions in 2019.
Cellulitis has the highest disease incidence, representing a significant source of morbidity with an aging population. Skin and soft tissue infections occurring in the setting of trauma, peripheral vascular disease, and immunocompromised states such as diabetes which are highly incident likely explains this. Increasingly refractory infections due to antibiotic resistance (MRSA infections for example) and the healthcare systems difficulty in addressing more chronic condition could contribute to the higher incidence.
Non-melanoma skin cancers combined had 60 times greater incidence than melanoma, likely due to a combination of sun exposure and Canada's aging population. Sun exposure is a greater risk factor for keratinocyte carcinoma than it is for melanoma. Even though melanoma occurred less frequently, it was the second largest contributor to mortality behind to breast cancer.
Fire, heat, and other substances were the most prevalent diseases, explained by good survivability and presence throughout an individual's life. Burns most commonly occur in younger individuals, with the highest incidence of burns being in males aged 45-54. 32 Burn survivors can live long lives with reduced disability as shown by highest YLDs but relatively small contribution to overall DALYs in plastic surgery related conditions.
The Canadian Institute for Health Information reported that healthcare spending was expected to reach $242 billion, or 11.5% of Canada's gross domestic in 2017. 33 Physicians accounted for approximately 15% of Canadian health care spending, with a total cost of approximately $36 billion. 34 There were a total of 627 practicing plastic surgeons in Canada who billed a minimum of $60 000 in provincial billing fees in 2017-2018. 35 Their average yearly billing was $391 425, equating to a total annual billing of $245 million compared the $10.6 billion CAD total cost of plastic surgery related diseases in Canada in 2019. 35 Therefore, every dollar that plastic surgeons bill the government addresses $43 of the burden of disease for the conditions assessed in this paper. It is difficult to make generalizable conclusions from this analysis, as there are many other conditions that plastic surgeons treat that are not discussed in this paper, and many other health disciplines that contribute to treating these conditions. In particular, the inability to include traumatic injuries based on the limitations of the GBD codes, especially upper and lower extremity and facial trauma is an important limitation to the economic benefit that plastic surgeons provide. Conversely, cellulitis and pyoderma are included in our analysis, but may infrequently require surgical care. This study provides a preliminary analysis of the benefit in providing plastic surgery services in Canada that needs to be followed with a comprehensive economic analysis examining direct, indirect, and future costs.
Government-funded plastic and reconstructive surgery is generally focused on treating hand injuries and diseases, breast cancer deformity, craniofacial injuries and diseases, skin cancer, burn injuries, and a variety of other reconstructive problems. The current evidence from GBD 2019 indicates that breast cancer, skin cancer, and burn injuries are a large cause of morbidity and mortality, justifying the current focus on treating and investigating these highly morbid diseases. These findings can help make evidence-based decisions regarding which diseases would benefit from increased funding in order to reduce disability and social and economic burden of disease. Future in-depth economic analyses should be used to advocate for increased funding and greater access to operating room and minor procedure time for the highly burdensome diseases such as burns and breast, head and neck, and skin cancers.
This study fills a gap in the literature on the morbidity and mortality of Canadian-specific plastic surgery related diseases. The most important limitation for our study is that the total DALYs and costs for included diseases are not solely in the domain of plastic and reconstructive surgery. For example, management of breast cancer and melanoma are shared by surgical, medical, and radiation oncology, family medicine, nursing staff, and other allied health. Furthermore, GBD 2019 data did not include several common plastic surgery conditions such as hand conditions (carpal tunnel syndrome, Dupuytren's disease, traumatic injuries to the hand, upper extremity nerve palsies), traumatic craniofacial and lower extremity reconstruction, and breast reduction surgery.
In the economic analysis, a universal CAD$50,000 per DALY value was attributed regardless of provincial differences that exist. This was done as GBD 2019 does not subcategorize by province. The costs calculated for provision of care are not comprehensive in this study. The physician's payments do not consider hospital costs, ancillary providers fee, and equipment that should be included in a full economic analysis. Furthermore, better characterization of indirect costs faced by patients beyond DALYs should also be considered. As the GBD constantly evolves, there will be changes in data collection and data analytical methods may come to influence the present results.36,37
Conclusion
Plastic surgeons address a large morbidity and cost of disease faced by patients in Canada. The major contributors to the burden of disease include breast cancer, melanoma, and traumatic injury due to thermal burns. Plastic surgeon payments in Canada totaled $245 million in 2016 while the GBD data shows an all-age burden of disease cost of approximately $10.6 billion for the 13 conditions examined by this study in 2019. These findings when combined with total healthcare spending per sector could provide evidence for deciding which conditions may benefit from increased spending to leverage economic gain from reducing disability. These results can be used to direct primary and secondary prevention strategies, healthcare expenditure, resource allocation and to advocate for improved funding for plastic surgery related diseases in the context of increasing healthcare demands.
Footnotes
Authors’ Note
This article does not contain any studies with human or animal subjects and did therefore not require REB approval.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.