
Abstract
Introduction
Laceration of the flexor tendons of the hand is often followed by retraction of the proximal stump into the tendinous sheath. Retrieval of the proximal stump may be traumatic both to the edges of the tendon and to the surrounding tendinous sheath. The former would require an additional trimming of the edges and an increase of tension over the repair. The latter may result in scar formation and impede the smooth gliding of the tendon within the sheath. This may result in either limited range of motion, a re-tear, or adhesion formations. 1 Retrieval of the tendon, therefore, should cause the least possible trauma to the tendon's edges and sheath.
The number of methods described in the literature is a testimony to the difficulty of this surgical maneuver. These include milking of the tendons by means of a reverse Esmarch bandage 2 and the use of rigid and flexible tendon retrievers 3 , hypodermic needles and skin hooks 4 , sutures 5 , steel wires 6 , suction catheters 7 , simple catheters,8–10 and feeding tubes.11,12
The purpose of this scoping review of all flexor tendon retrieval techniques is to describe the available surgical techniques and where available to present the best clinical evidence associated with each.
Methods
We reviewed all publications that appeared in the English literature since 1971. The search was performed in Medline and Web of Science. A combination of words “(retrieval OR retrieving OR edge) AND flexor” was used. We reviewed the abstracts to exclude all publications on basic science. After this initial screening, we checked the main text of each publication and excluded all of those that did not describe or compare tendon retrieval methods. Both authors screened and summarized the peer-reviewed manuscripts that were identified as being suitable for this review (Table 1). The number of study subjects, and advantages and disadvantages of each technique were recorded for each article. Detailed descriptions of each technique were qualitatively analyzed to divide the techniques into groups. This review was performed according to the PRISMA guidelines, but was not registered as a systematic review but rather a scoping review that employed a systematic approach to literature search.
- Summary of studies on flexor tendon retrieval techniques
Results
The literature search yielded a total of 841 publications. Details of the selection process are provided in Figure 1. The techniques were arranged into 8 distinct groups:
Blind grasping (n = 2). Suction (n = 1). Milking (n = 2). “Walking” the tendon antegrade with needles, hooks, or forceps through a proximal incision (n = 3). Endoscopic retrieval (n = 4). Delivering the proximal stump distally with 2 incision techniques.
Delivery of the proximal stump and attachment end-to-end to a guide catheter, tube, glove, or wire (n = 12). Side-to-side suturing of the guide catheter (without pulling the tendon out of the proximal incision) (n = 5). Seldinger catheter (n = 3). Aneurysmal needle (n = 1).
Study selection flowchart.
Blind Grasping
The forceps are introduced into the tendon sheath. The jaws of the forceps are closed or slightly opened upon introduction. The tip of the forceps is used as a probe and the jaws are open to grasp the tendon edge and pull distally.
The flexible forceps were suggested as being a technically superior solution to a 2-incision technique with a retrieval tube. 3 This was refuted by the findings of Taha and Kadry 13 who performed a prospective study to compare blind grasping (n = 50) to a 2-incision and feeding tube technique (n = 50). After a mean follow-up of 8 months, the 2-incision technique was statistically superior in all aspects, including shorter operative time (31.80 ± 3.79 vs 37.34 ± 5.74 min, respectively), faster return to work (15.40 ± 3.25 vs 19.34 ± 5.43 weeks), and lower complication rates (12% vs 26%).
Suction Catheter
Described by Pennington in 1977 7 , this technique includes irrigating the tendon sheath to remove any existing blood clot, followed by insertion of a flexible 14-16 gauge suction tube down the tendon sheath during which suctioning is turned off or clamped. When the suction tip hits the tendon, the suction is turned on and the tendon is pulled distally. The author described a 66% success rate with this technique and noted that the success rates were lower for retrieval of the thumb flexor pollicis longus (FPL) tendon compared to the other fingers flexor tendons (Figure 2).
A suction tube is inserted to the tendon sheath; suction is activated and the tendon is pulled distally.
Reverse Milking of the Forearm Muscles
After Kleinert et al 37 reported applying “antegrade sweeping external pressure” to the forearm to “milk” the tendon out of its channel, Rice and Yanni 14 improved the technique by using an Esmarch tourniquet. The Esmarch tourniquet was applied from the elbow towards the wrist after which the wrist was flexed (Figure 3) and effectively pushed the tendons distally. Goshgarian 2 reported the same technique with the use of an elastic bandage.
Reverse milking with an Esmarch as a method to apply pressure on the flexors tendons and “milk” the tendon out of its channel.
The main disadvantage of the technique is low success rate (61%). Advantages include low cost, and not compromising the tendon, flexor sheath or the blood supply as well as obviating the need for further incisions.
Push-Pull Techniques to Retrieve the Flexor Tendon
Several methods exist for “walking” the tendon distally from the proximal incision. They all entail a proximal incision over the A1 pulley, identification of the retracted tendon and pushing it distally. This technique is limited in the little finger where the flexor sheath over zone 2 is tight. Morris and Martin 4 described this technique with the use of a hypodermic needle and skin hooks. A proximal incision is performed, and the tendon is exposed. A hypodermic needle is then inserted into the tendon and pushes the tendon distally (Figure 4). For the “pulling” part of the technique, the authors recommended using skin hooks to pull the tendon distally (Figure 4 panel). This method is traumatic to the tendon and is only successful if the tendon is retracted short distances. Two recent studies15–17 described “walking” the tendon distally with the use of 2 forceps. Both found the technique to be quick and easy and recommended its use when multiple tendons are retracted. Khoo and Nikkhah 16 described their successful experience with push-pull techniques on 66 patients.
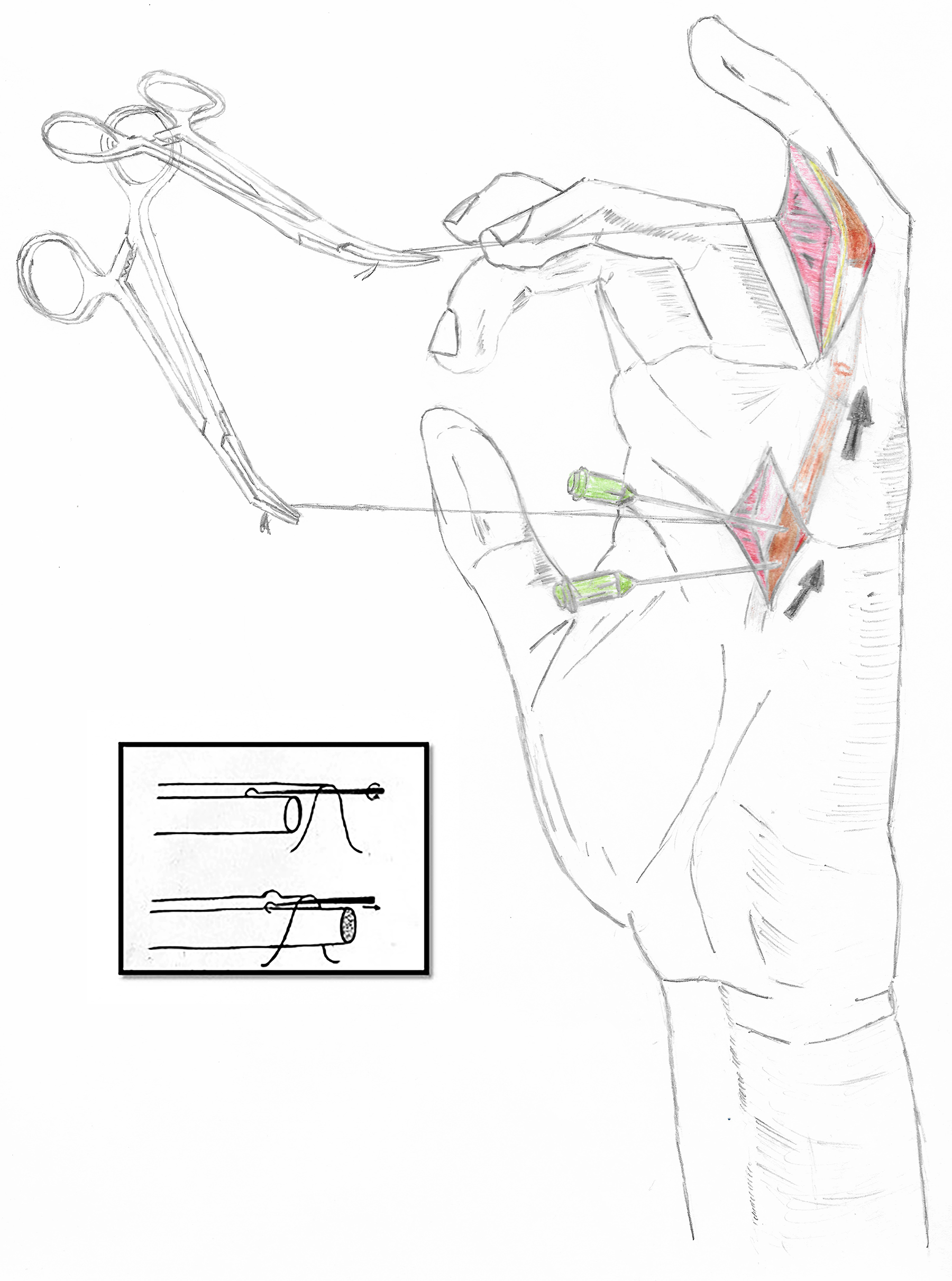
Pushing the tendon with hypodermic needles through the proximal incision. Panel: pulling the tendon distally with skin hooks.
Endoscope and mini grasper
Li et al 18 pioneered the endoscopic approach for retrieval of the flexor tendon through one incision. The authors utilized a 3.1 mm diameter flexible Olympus ureteroscope with a 1.2 mm instrumentation channel to retrieve the tendon. A Cook urologic forceps was passed through the instrumentation channel, and the endoscope was passed into the tendon sheath at the level of the laceration. Direct visualization of the cut end of the flexor tendon was easily achieved under continuous low-pressure irrigation with normal saline. The severed tendon end was grasped and pulled distally (Figure 5). Those authors reported successful tendon retrieval in 3 cadavers and 3 patients.
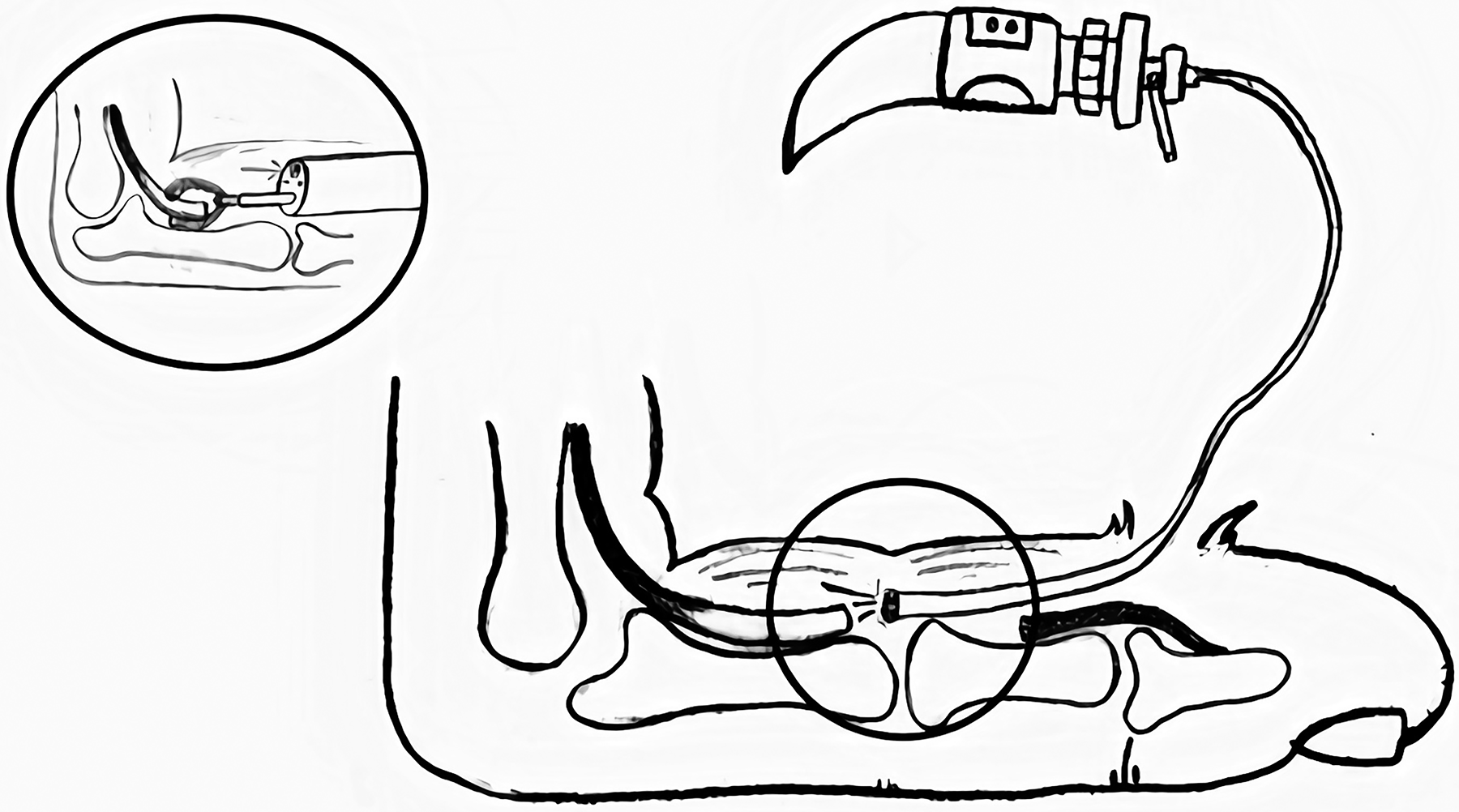
Endoscope is inserted into the tendon sheath to visualize the retracted tendon. Panel: a grasper is used through the working channel to retrieve the tendon.
Hill et al 19 utilized a smaller endoscopic system with smooth edges to demonstrate that retrieving the flexor tendon is feasible with minimal soft tissue manipulation. They reported successful retrieval of 32/34 (94% success) tendons in a cadaveric study. They used the flexible Intramed endoscope and either the alligator forceps or a modified “lasso” loop grasper for grasping. The authors reported more effective retrieval with the lasso loop grasper than the forceps.
Kucukguven at el. 20 provided clinical evidence of the superiority of the endoscope over blind retrieval of the tendon. In their randomized controlled study, they compared patients with flexor tendon laceration that were divided into 2 treatment groups, endoscopic retrieval with a 2.5 mm scope and retrieval by proximal incision. Although the groups were small (11 patients in each), there was a significant advantage to the endoscopic group with regard to length of surgery (58.2 ± 10.1 vs 73.6 ± 10.7 min), pain score at 1-2 weeks (2.5 ± 0.5 vs 3.0 ± 0.4), and total range of motion at 3-5 weeks (57.7 ± 16.6 vs 37.3 ± 12.5 degrees). Pain and range of motion were not statistically different after 8 weeks of follow-up.
More recently, Bednarz et al 21 reported their successful use of a disposable endoscope for retrieval of the FPL. Those authors used a large caliber 3.8 mm Abmu® aScope™ (Ambu A/S, Ballerup). Despite its large caliber, successful retrieval was still possible without the concern of high costs of sterilization of the Uretroscope.
In summary, the advantages of retrieving a flexor tendon with an endoscopic system are direct visibility of the severed tendon, less traumatic tendon retrieval both for the tendon and tendon sheath and shorter operative times. The disadvantages are its availability only in operating rooms where urological procedures are performed, cost and the learning curve of using this technique.
Delivering the Proximal Stump Distally With 2 Incision Techniques
One of the most commonly used methods of delivering the stump distally is exposing it through a proximal incision, usually over the A1 pulley, and delivering the stump distally using an array of techniques. Advantages of this technique include cost, relative atraumatic technique and familiarity of most hand surgeons with it. Disadvantages are additional OR time and an additional incision. Variations in this technique can be roughly divided into 2 groups: one involves complete retrieval of the proximal stump through the proximal incision and suturing it end-to-end to a tube or a wire, and the other involves maintaining the stump in place while attaching it to a tube side-to-side to “railroad” it distally.
Techniques in Which the Tendon is Extracted Through the Proximal Incision
One of the first descriptions of this technique was by Kilgore et al 22 in 1971. They described the performance of a proximal incision and the retrieval of the tendon through that incision. A feeding tube connected to a syringe is then passed distally to proximally while filling the tendon sheath with normal saline for easier passage. Finally, at the proximal incision, the tendon is sutured to a feeding tube and then pulled distally. The authors rated the technique as being atraumatic and foolproof in over 5 years of experience.
Many improvements and tricks were added to this technique over the years to allow smoother passage of the tendon through the sheet:
Cutting a tube off an intravenous infusion set in the shape of a shark nose (Figure 6). The tendon is threaded through the tube and is engulfed by it to create a less bulky interface
23
. Aksu et al
24
reported a very similar technique with suturing of the proximal tendon to a silastic tube that was cut in 2 halves to engulf the tendon. Wharton et al
25
also reported a similar technique that employed a 12G silastic urinary catheter. They experienced success with this technique in over 20 cases. The use of a red rubber catheter inserted into the sheath as described by Abouzahr
8
. The proximal end of the tendon is sutured with a half Kessler knot. A Keith needle is then inserted into the catheter about 10 cm from its proximal end, after which the threads are passed through the catheter. The tendon stump is inserted into the funnel-shaped edge of the red rubber catheter and delivered distally. An additional advantage of this technique is the protection of the tendon edge when it is placed into the funnel-shaped catheter. The use of a glove to engulf the tendon for smooth passage in the sheath as described by Thornton and Miller
26
. They reported successful retrieval in 8 out of 10 patients, but noted that this technique bears the risk of leaving glove fragment in the tendon sheath. Suturing of the proximal stump with a Kessler knot as described by Bhatti and Adeshola
27
. After completion of the suturing, the needle is straightened and a plastic cannula is inserted from distal to proximal. The straight needle is then inserted into the cannula and pulled distally along with the tendon. Ozturk et al
28
reported a similar technique with success and no complications in 21 cases. Suturing of the proximal stump with a feeding tube as described by Ho and Schnall
29
who used a #8 French feeding tube. The sutures that had been placed in the proximal tendon are passed through the lumen of the tube and retrieved through the distal incision. The tendon is pulled to become flush with the cut end of the tube, after which the entire construct is pulled distally and the tendon is retrieved. Iwuagwu and Gupta
6
described another simple, atraumatic technique that utilizes steel wires, which are readily available in the OR. The steel wire is twisted to create a loop at the end. The loop is passed from distal to proximal, the sutures from the tendon are threaded through the loop of the steel wire and the tendon is then pulled distally (Figure 7). Other authors30,31 modified this technique and used dental wires.
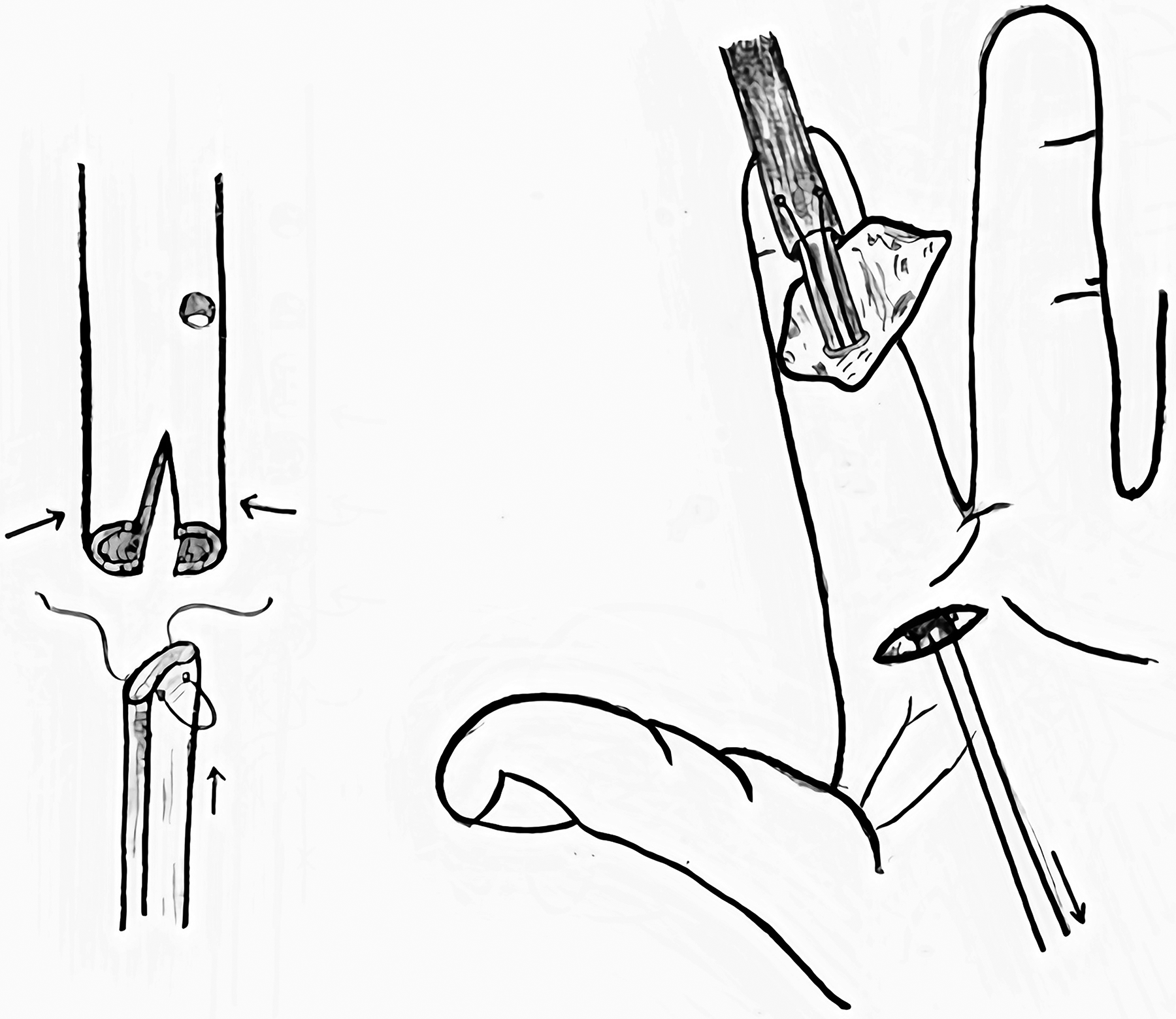
The shark nose technique to create a smooth interface between the end-to-end tendon-tube connection (right panel), pulling the tendon distally with a 2-incision technique (left panel).
Using steel wires for retrieval of the flexor tendon through a 2-incision technique. The wires are twisted to create a loop at the end through which the sutures are passed.
Techniques in Which the Tendon is Sutured side-to-side with the Delivery Device
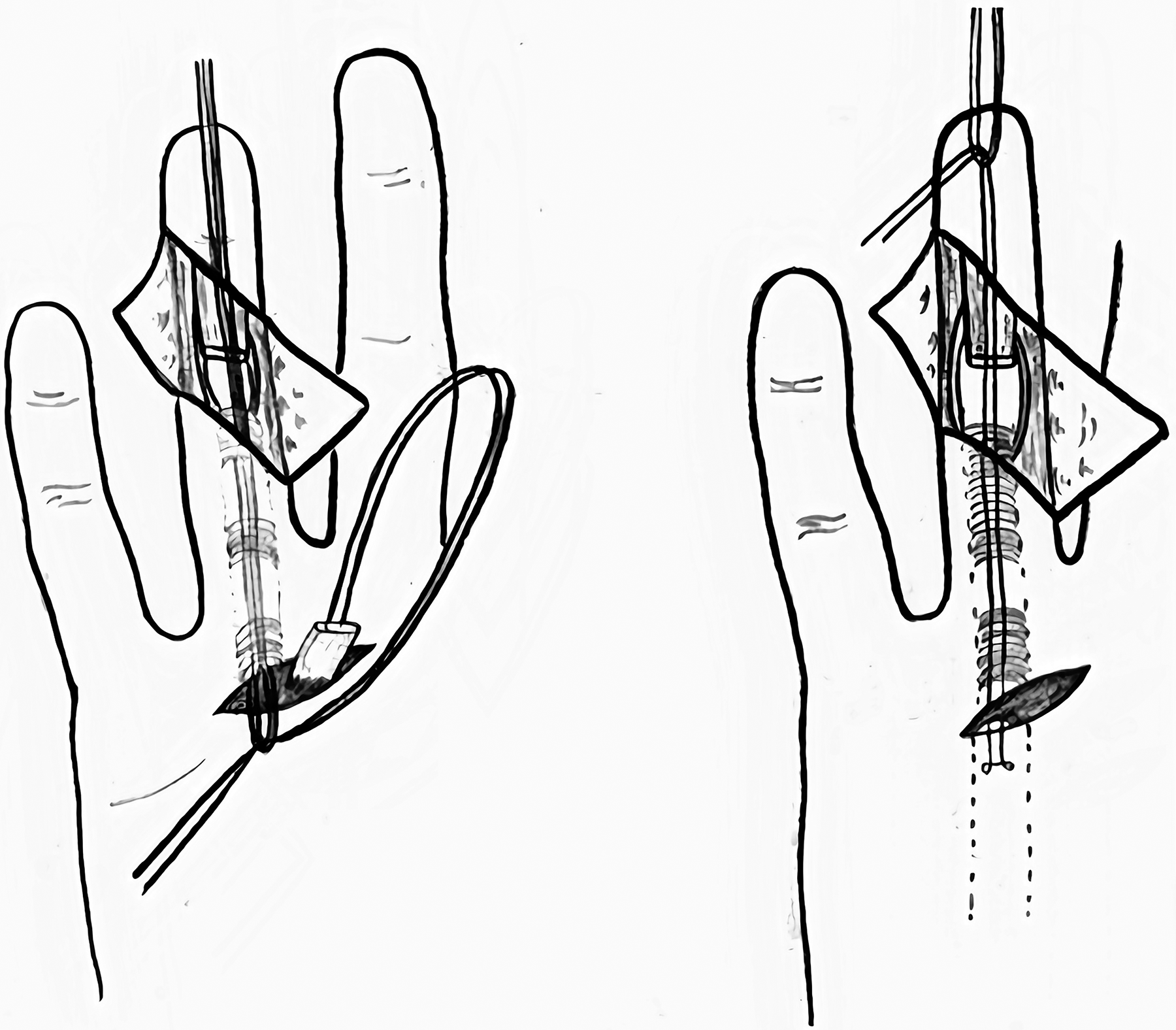
Sourmelis and McGrouther 10 described a technique in which the proximal stump is not removed from the sheath and retracted through the proximal incision. A pediatric suction cannula is inserted alongside the flexor tendons from the proximal to the distal incision and sutured side-to-side with the tendon and then delivered distally (stages 1 and 2). Once the proximal tendon end is delivered to the tenorrhaphy site, a core suture is placed (stage 3) and the tendon is then allowed to retract back into the sheath so that the side-to-side suture between the tube and tendon is positioned at the proximal sheath entry. The suture is then divided, and the tube is removed (stage 4). According to those authors, this allows a more atraumatic technique by not interrupting the vincula.
Sourmelis's technique is widely quoted and modified by others. Two studies11,33 described a slight modification where a loop release knot was used instead of a simple knot between the side-to-side tendon-tube suture, allowing the knot to be released by simply pulling on it, thus precluding the need for stage 4.
Karbalaeikhani and Yavari 34 used a long loop of nylon suture to connect the proximal stump that was left in situ to the feeding tube. The tube is delivered distally, pulling on the tendon and retrieving it distally as well. This technique also precludes the need for Sourmelis’ stage 4.
Wong and McGrouther 32 described some refinements of Sourmelis’ technique that were developed over the 26 years since it was originally described. The modifications involved inserting the catheter in either an antegrade or a retrograde direction, and not suturing the tendon to the tube but snaring it instead, whereupon the tube and suture can remain in situ to act as a “no touch” retractor until the repair is finished, thus limiting the need for proximal wound extension.
Seldinger Catheter and Other Methods of Tendon Sheath Dilatation
The Seldinger technique is employed when the feeding tube fails to be threaded through the tight flexor sheath. Once a Sledinger thin wire is passed either ante- or retrogradely through the flexor sheath, a catheter can easily be fed over the wire. The wire is then removed, leaving the catheter in situ. The tendon can then be stitched to the catheter and delivered into the wound.9,35
Kamath and Bhardwaj 36 used a stainless steel wire (20-24 gauge) that was folded onto itself as a method to retrieve the tendon. The folded wire was introduced to the tendon sheath from distal to proximal and the core sutures that had been made in the proximal stump were threaded through the fabricated eye and pulled distally. Those authors described changing the size of the eye as a method to dilate the flexor sheath. They summarized this method as being a simple, inexpensive, and relatively atraumatic tendon retrieval technique that has stood the test of time in both primary and secondary surgical repairs and reconstructions of flexor tendons in over 10 years of clinical experience.
Aneurismal Needle
This technique was described for the retrieval of tendons over a short distance. A core suture is passed through the proximal end of the tendon. An aneurismal needle (a curved, blunt needle with an eye in the end) is then passed under the tendon sheath and the sutures are passed through the needle and delivered distally, followed by delivery of the tendon. Alternatively, Hettiaratchy and Titley 5 suggested used Lister's “windowing” 38 of the pulleys technique to increase the distance which involves several small incision in the pulleys and stepwise retraction of the tendon distally.
Discussion
Retraction of the flexor tendon into the tendon sheath is a frustrating problem in flexor tendon surgery. In this paper, we summarized all flexor tendon retrieval techniques that have been published in the hand surgery literature during the past 50 years. Our search revealed that only 2 papers compared techniques in a scientifically sound manner.13,20
Methods for retrieving the tendon can largely be divided into single and double incision techniques. Taha et al. 13 have recently reported superior results of tendon guidance by silicone rods compared to blind grasping with regard to recovery time, complication rates, and even operative times. He concluded that at the expense of another incision, a less traumatic repair can be performed.
Endoscopic retrieval of the tendon stump was introduced in the 1990s but had not been adopted into clinical practice. A recent comparative trial 20 demonstrated that endoscopic retrieval is clinically superior to blindly grasping the tendon, in terms of operative time, range of motion and pain scores. The possibility of direct visualization and atraumatic technique led the authors to propose a new treatment algorithm that included the use of an endoscope before attempting a proximal incision.
More of the publications focused upon use of flexible guides for traveling the proximal stump through the tendon sheath. We consider that the exact material from which the guides are made, that is, silicone or rubber catheter, rubber glove, or dental wire, makes less difference than the issue of complete excision of the tendon outside the skin versus attachment of the guide to the tendon while the latter remains inside the tendon sheath. Complete extraction of the tendon through the proximal wound would severe the remaining attachments between the sheath and the tendon, thereby further jeopardizing the scarce blood supply to the tendon. 39 Pennington cautioned that such “…bare tendon, ‘railroaded’ back into the sheath, is then little better than a tendon graft”. 7 While we found many variations of both of the groups, we found no clinical trial to compare them.
The limitation of this study is the lack of quantitative evidence of the effect of each technique on patient outcomes. Additionally, the discussion of advantages and disadvantages of each technique in the publications was highly subjective. Due to the low quality of evidence, a systematic review could not be produced.
In conclusion, after reviewing the literature for solutions to flexor tendon retraction, it is evident that a definitive solution remains elusive. Based upon our analysis when the tendon has withdrawn into the palm, it can be expected to be found at the A1 pulley level. If milking of the tendon fails to deliver it to the incision, when available, endoscopic retrieval should be utilized. If endoscopic retrieval is not available then the best clinical practice is to perform a second incision at the level of the A1 pulley and not blindly trying to retrieve the tendon. Further studies that include randomization and clinical outcomes on larger numbers of patients are needed to determine the best therapeutic management.
Footnotes
Author Contributions
Assaf Kadar: conceptualization, methodology, investigation, writing-reviewing and editing. Shanny Gur: investigation, drawing. Haggai Schermann: investigation, validation, writing—original draft preparation. Sorin D. Iordache: supervision, validation, writing-reviewing and editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.