
Abstract
Bilateral defects around the knee joint following fracture of the proximal tibia (Schatzker type V & VI) are difficult to reconstruct because of the unavailability of local tissue. A bicondylar proximal tibial fracture requires a bilateral approach and dual plates for fracture fixation. Because of extensive dissection during plating and extended zone of trauma, the suture lines occasionally dehisce resulting in soft tissue defects on both sides of the proximal tibia. Because of its bilateral nature, the defect requires 2 flaps. We are reporting 2 cases of suture dehiscence after fixation of bicondylar fracture of the proximal tibia which required reconstruction with bilateral gastrocnemius flaps. This reconstruction is a simple option that helps in providing stable coverage. The first case was followed up for a period of 5 years and the second case was followed up for a minimum period of 6 months. Both cases demonstrated well-healed flaps, united bone and no donor side morbidity. Bilateral gastrocnemius muscle flaps can be used simultaneously for 2 separate defects on both sides of the knee without significant donor site morbidly. This reconstructive option provides stable coverage, reduces the infection and promotes bony union thus helping in early ambulation.
Introduction
Bicondylar plateau fracture of the proximal tibia Schatzker type V and VI is a common injury following road traffic accidents. 1 Fixation of this fracture often requires a bilateral approach; one from the posteromedial side and another from the anterolateral side by dual plates. 2 Occasionally after fracture fixation, the suture lines dehisce resulting in soft tissue defects 3 exposing the implants which require coverage in the form of well-vascularized tissue which helps in bone healing, reduces the infection and provide stable and aesthetic cover. Because of bilateral defects, it requires 2 flaps that fulfil the criteria of reconstruction at these 2 separate sites. Also, because of extensive damage to the local tissues, local flaps are often unavailable. Free flaps in such a defect demand microsurgical expertise and set up and comparatively longer operative time, also a single flap is inadequate to cover both the defects situated at medial and lateral condyles, respectively, that are far away from each other.
Gastrocnemius muscle flaps are well-defined flaps to cover the defects around the knee. Either medial or lateral gastrocnemius muscles are often used to cover medial or lateral knee defects, respectively. Using both the bellies of muscle for 2 separate defects on both sides of the knee is less described in the literature. 4 This paper aims to assess the utility of using both the bellies of gastrocnemius which is a regional muscle flap option that can be used to cover the 2 defects that are far apart on both sides of the knee. Its easy harvest, well-defined vascularity and less donor site morbidity make it a simpler option for such defects.
Methodology
Case 1
We are presenting a case of a 24-year-old male who had a road traffic accident (RTA) and sustained bicondylar proximal tibial plateau fracture Schatzker type VI. The patient was primarily treated by orthopaedic surgeons by dual plate fixation. In the postoperative period, the suture lines on both the sides of the knee dehisced and the patient were referred to us for soft tissue reconstruction (Figure 1a and b).
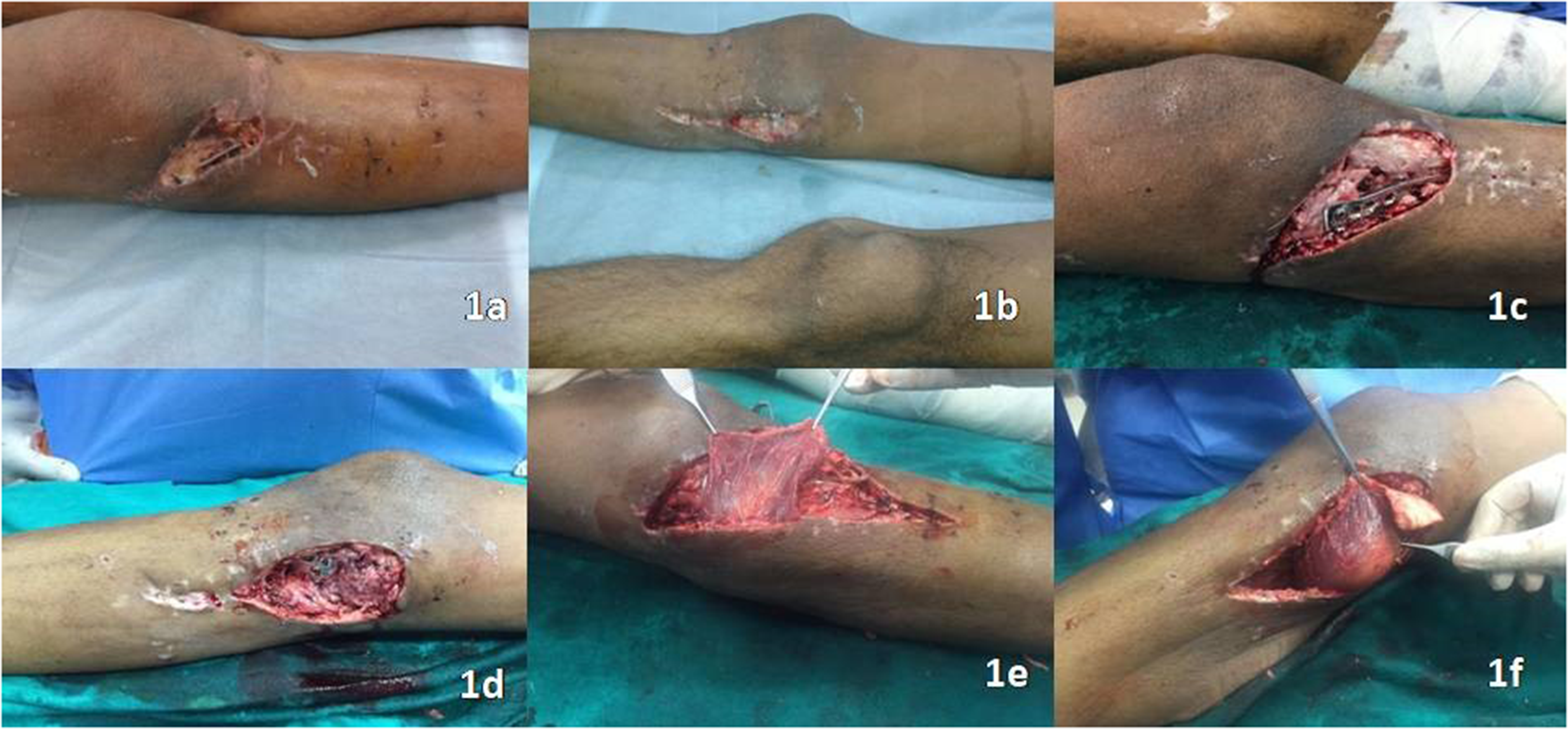
(a) Soft tissue defect with an exposed implant on the lateral aspect of the proximal tibia. (b) Soft tissue defect with an exposed implant on the medial aspect of the proximal tibia. (c) Defect recreated around 10 × 5 cm on the lateral aspect of the knee after debridement. (d) Defect recreated around 8 × 5 cm on the medial aspect of the knee after debridement. (e) Lateral gastrocnemius muscle over the lateral defect. (f) Medial gastrocnemius muscle over the medial defect.
The wound was debrided under spinal anaesthesia in the supine position and under tourniquet control. The recreated defects measured 10 × 5 cm on the lateral aspect and 8 × 5 cm on the medial aspect with the exposed implants (Figure 1c and d).
Challenges to reconstruct such defects were not only adequate coverage of implants on both sides of the knee but also to augment the bone healing, reducing the infection and providing stable cover. Seeing the unsuitability of local skin flaps from the zone of trauma due to previous trauma and dissection during plating, a regional flap in the form of bilateral gastrocnemius muscle flaps was considered.
The knee was flexed and marking for the midline was done in the mid posterior aspect by palpating 2 heads of the gastrocnemius muscle. The posterior midline incision was made and a short saphenous vein and sural nerve were identified and isolated. Both the muscle bellies were identified attached with a median raphe distally and the muscle was separated from the underlying soleus muscle by blunt dissection. A part of the tendinous portion was harvested along with the gastrocnemius muscle for the better anchorage of the flap to the defect. Now along the median raphe, both the bellies of gastrocnemius were separated by electro-cautery and dissected proximally with the inclusion of median and lateral sural artery pedicle, respectively. However, to increase the reach, the muscle can be dissected further proximally and the origin can be released, but it was not required in our case. Now both the muscle bellies were tunnelled beneath the skin to inset with the defects on both sides (Figure 1e and f). The tendinous part of the gastrocnemius muscle belly was anchored with the dermis at the recipient site during insetting of the muscle flap. This would allow effortless suturing, stable anchorage and also prevent cutting through the muscle when sutures are taken directly through the muscle fibres. The skin graft was applied over the muscle and was fixed by staples (Figure 2a and b). The donor area of the flap was closed primarily and the suction drain was kept for 2 to 3 days. An above-knee Plaster of Paris slab was applied for postoperative immobilization which was removed after 2 weeks. From the third week onwards, when skin graft settled, toe-touch weight-bearing and partial weight-bearing was started and continued for 2 to 3 months. Full weight-bearing was started after 10 to 12 weeks only.
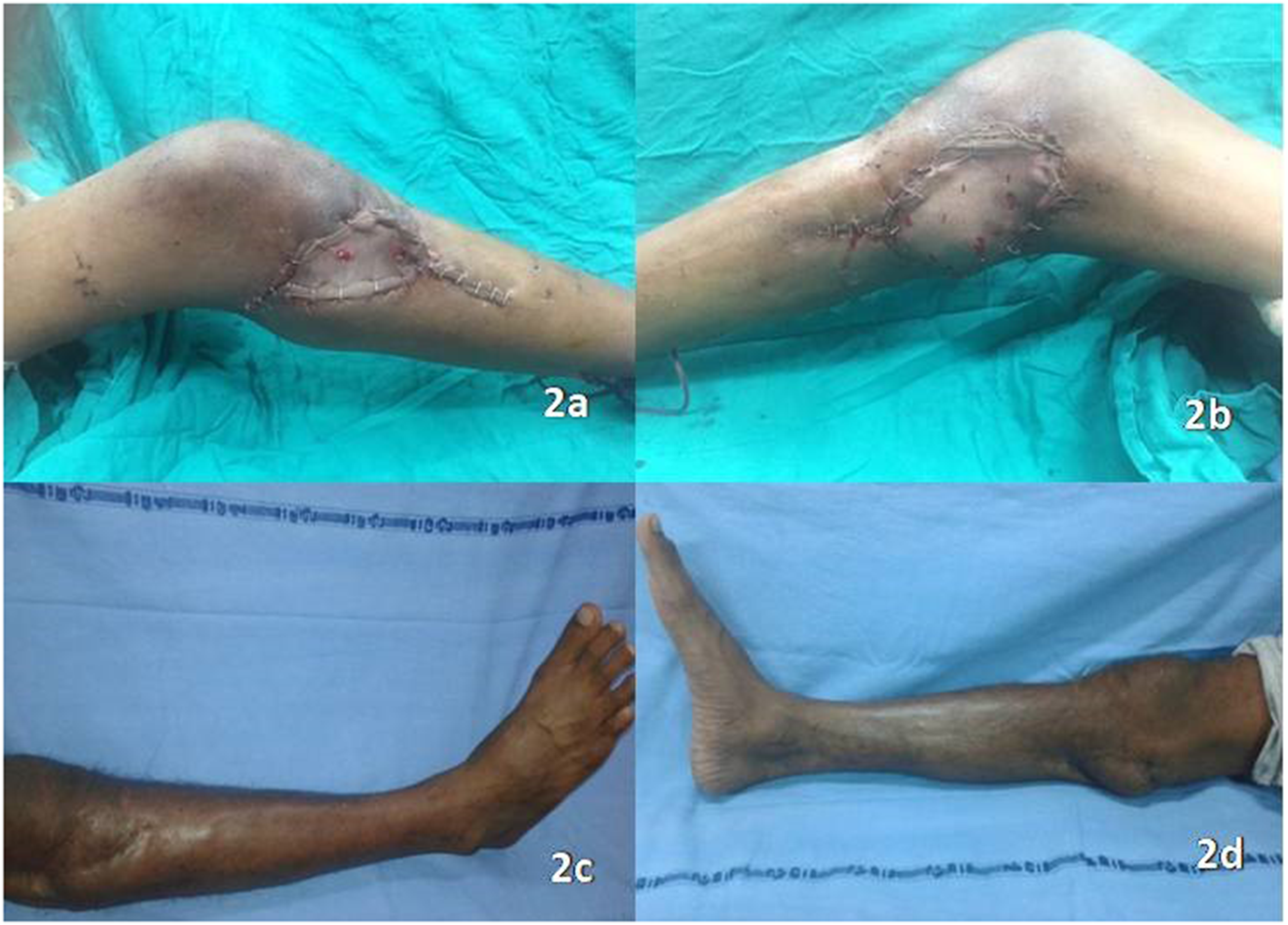
(a) Lateral gastrocnemius muscle covered with a split-thickness skin graft (STSG). (b) Medial gastrocnemius muscle covered with STSG. (c) Long-term outcome with a well-settled flap and STSG, lateral aspect. (d) Long-term outcome with a well-settled flap and STSG, medial aspect.
In long-term follow up (5 years), the flap and skin graft settled well with the donor site healed primarily (Figure 2c and d). The underlying bone united (with an average bone union time of 6 months) and the patient restored normal ambulation (Video). In the postoperative period, patients did not complain of any gait disturbances or plantarflexion weakness (Medical Research Council (MRC) grading 5/5).
Case 2
A 42-year-old male with a history of RTA was diagnosed with fracture right proximal tibia type V, grade II liver injury and grade IV renal injury. A knee spanning external fixator was applied initially in view of renal injury. Open reduction and internal fixation of the tibia were done with 2 holes posteromedial plate and 3 holes anterolateral plate a week later. Subsequently patient developed suture line dehiscence with exposed instrumentation medially and laterally in the proximal leg (Figure 3a and b). The bilateral defects needed a stable cover, so it was decided to perform a bilateral gastrocnemius muscle flap.

(a) Soft tissue defect with an exposed implant on the lateral aspect of the proximal tibia. (b) Soft tissue defect with an exposed implant on the medial aspect of the proximal tibia. (c) Lateral gastrocnemius muscle over the lateral defect. (d) Medial gastrocnemius muscle over the medial defect. (e) Lateral gastrocnemius muscle covered with STSG. (f) Medial gastrocnemius muscle covered with STSG.
The bilateral gastrocnemius muscle flap was performed with the same technique as described in case 1 with the same postoperative physiotherapy protocol (Figure 3c–f)
The flap was healthy in the postoperative period, patient developed suture line dehiscence due to underlying infection which was managed conservatively with intravenous antibiotics and wound irrigation. At 6 months follow up patient presented with bilaterally healthy muscle flaps and well-settled skin graft (Figure 4a and b) and with MRC grading 5/5 for muscles of both dorsi/plantarflexion.
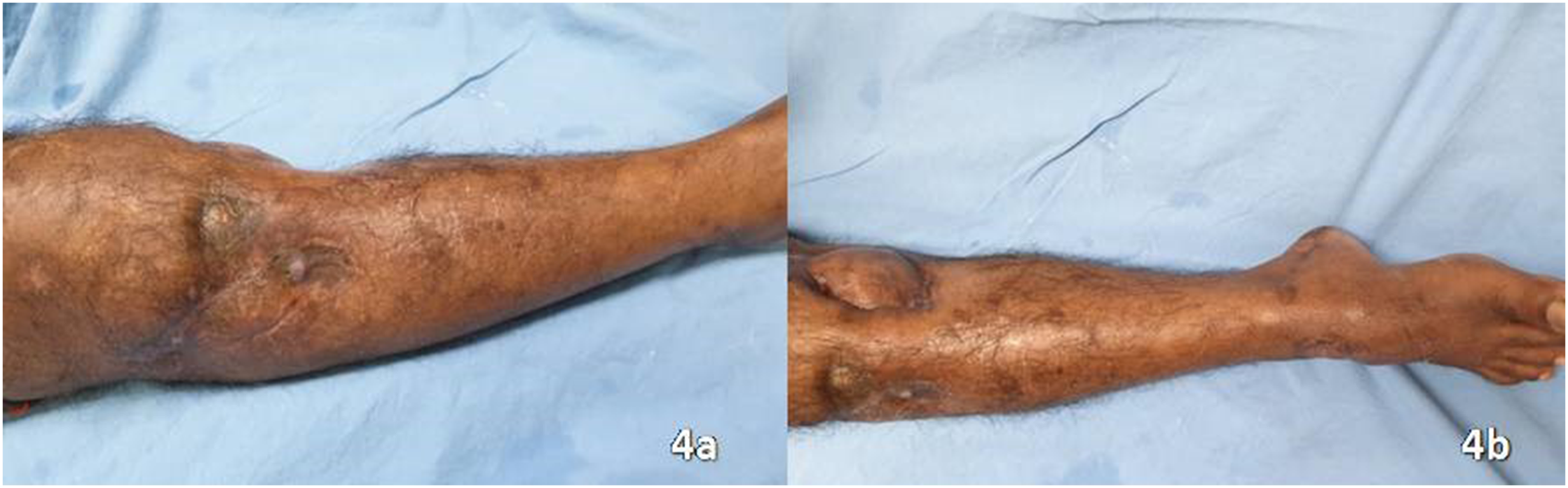
(a) Long-term outcome with a well-settled flap and split-thickness skin graft (STSG), lateral aspect. (b) Long-term outcome with a well-settled flap and STSG, medial aspect.
Discussion
Bicondylar fracture of the proximal tibia is not an uncommon injury after high-velocity trauma of RTA. For placement of plates to fix the fracture it often requires 2 incisions which may dehisce depending upon the amount of dissection during plating or extensive soft tissue damage following RTA even in closed fracture and thus resulting in oblique defect extending from lateral to the anterior aspect of the proximal leg.
Several authors have found the deep infection rate of 8.06-8.4% in the complications associated with internal fixation of high-energy bicondylar tibial plateau fractures utilizing a 2-incision technique.3,5 Those patients subsequently developed wound dehiscence with discharge resulting in soft tissue defect. 3 Gastrocnemius muscle flap is a well-described entity for knee defects. 6 Being a muscle flap with good vascularity, it helps in reducing the infection and is often recommended when fracture healing has to be augmented. However, one of our cases developed soft tissue infection in the postoperative period which subsided with dressing and antibiotics. Hari and colleagues 4 first time described such a defect as Harlequin defect and reported 3 cases using bilateral gastrocnemius muscle flap with a mean duration of follow up of 10 months. They found bony union in all cases with a mean union time of 6 months and no soft tissue complications. The limitations of a single head or total gastrocnemius muscle flap are the inability to cover multiple separate wounds in the same area around the knee. 7 Thus using 2 flaps is often required.
Wei 8 has documented using pedicled medial and lateral gastrocnemius muscle flap for large medial anterior and lateral aspect of the upper tibia with well-settled flap and graft area.
Using free flaps for such defects will require 2 flaps with a minimum of 4 vascular anastomoses. This is because the 2 defects are situated at 2 condyles of the tibia and are far away from each other. It mandates microvascular expertise and instrumentation with prolonged anaesthesia and surgical time. Reconstructing such 2 defects by a single free flap has not been reported in the literature.
Whereas bilateral gastrocnemius muscle in the form of regional muscle flap can be performed with less operative time, without microsurgical experience and at a low resource set-up.
Cross leg flap is another reliable option but that is too cumbersome for the patients. Agarwal et al. 7 in their cadaveric study have described splitting each belly of gastrocnemius muscle thus allowing coverage of multiple wounds around the knee. Splitting the medial muscle belly proximally up to 2.3 cm and lateral belly up to 3.21 cm is safe without damaging the blood supply. Still using it clinically for defects that are on either side of the knee is not documented. Also, using it clinically may require meticulous dissection and also segmental blood supply for lateral gastrocnemius is not constant and thus not advocated splitting without doing preoperative colour Doppler.
Cavadas 9 in 1998 reported a split medial gastrocnemius muscle flap, but its feasibility to reach the other defect at lateral condyle is not reported in the existing literature. In comparison using each head for each defect appears to be an easy, simple and reliable option.
Peroneal neuropathy is a recognized complication following lateral gastrocnemius flaps with the incidence reported between 4.5% and 19% in the literature, neuropathy may be due to direct injury, infection, intraoperative traction injury or compression.10,11 In both of our cases, patients were able to adequately dorsiflex the foot. Postoperatively MRC grading was 5/5 for muscles of dorsi/plantarflexion of the foot.
Conclusion
A bilateral gastrocnemius muscle flap is an easy, reliable option for bilateral defects around the knee joint that can be performed by a reconstructive surgeon with limited experience at any set-up. Timely intervention using both medial and lateral gastrocnemius muscle flaps for reconstruction helps in coverage of exposed implants in proximal bicondylar tibial fracture Schatzker type V & VI and thus reduces infection and promotes bone healing for early ambulation without much donor site morbidity.
Supplemental Material
Footnotes
Authors’ Note
Informed consent was obtained from all individual participants included in the study for publishing their cases and photographs.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.