
Abstract
Introduction
Distal radius fractures are one of the most common injuries of the hand and wrist, especially in sports-related trauma, motor vehicle accidents, and patients with osteoporosis.1–3 Due to temporary short-term disability, patients with these injuries may be unable to care for themselves and may require home health assistance or discharge to a post-acute care facility to optimize recovery and rehabilitation.4,5 These facilities include skilled nursing facilities, unskilled facilities, long-term acute care facilities, and inpatient rehabilitation centers. 6
As medical reform has incentivized decreases in hospital length of stay and readmission, there has been a dramatic rise in the No. of patients discharged to rehabilitation facilities.7,8 This has resulted in increased healthcare expenditures spent on post-acute care which has been identified as a possible area for cost control.8,9 In a large database study, 13.4% of patients across multiple surgical specialties were not discharged home. 10 Patients undergoing surgical repair of distal radius fractures also have higher complication rates and readmission rates than most hand surgery patients. 11
The objective of this study is to examine post-acute care utilization patterns in patients undergoing open reduction and internal fixation (ORIF) of distal radius fractures. We examine a large, national, multicenter database to identify risk factors that predispose patients who have undergone ORIF of distal radius fractures to discharge to post-acute care facilities and examine the impact of post-acute care facility utilization of value-driven outcomes. These findings may aid in patient decision-making and discharge planning, preventing delays in the transfer that can prolong hospital lengths of stay and increase costs.
Methods
This study was conducted using the American College of Surgeons National Surgical Quality Improvement Program® (NSQIP) database. Institutional review board exemption was obtained on the basis of de-identified patient information. ACS NSQIP uses a validated, risk-adjusted, outcomes-based approach to collect patient and surgical variables. The history and methods have been described previously.12,13
Study Design
NSQIP participant data files were obtained from 2011 through 2016. The database was queried for patients whose primary Current Procedural Terminology (CPT) code correlated with open treatment of distal radius fracture, 25607, 25608, or 25609. Exclusion criteria included concomitant traumatic injuries (ie spinal cord injury, brain injury, etc.), concurrent surgical repair of the lower extremity, unknown discharge information, and death during hospitalization.
Patient demographics collected were age, sex, race, and location prior to hospitalization. Comorbidities including either overweight or underweight body mass index (BMI), diabetes, smoking, hypertension, chronic obstructive pulmonary disorder (COPD), dyspnea, congestive heart failure (CHF), dialysis dependence, preoperative steroid use, bleeding disorders, and American Society of Anesthesiologists (ASA) classification. Perioperative and surgical factors collected were the type of anesthesia, fracture pattern (CPT code), emergency surgery, bilateral surgery, associated procedures (eg carpal tunnel release, scaphoid surgery, and ulnar styloid repair), wound classification, and complications prior to discharge.
Outcomes
Our primary outcome was postoperative discharge destination, either home or a post-acute care facility other than home. Patients were dichotomized by whether they were discharged home or to another destination listed in the NSQIP database including skilled care (eg transitional care unit, subacute hospital, and skilled nursing home), unskilled facility (eg nursing home, assisted living facility), facility in which they resided preoperatively, separate acute care (eg transfer to another hospital, long-term acute care facility), or rehabilitation facility. Secondary outcomes included unplanned readmission, unplanned reoperation, medical complications (eg pneumonia, myocardial infarction, kidney injury), and wound complications (eg dehiscence, bleeding, infection) occurring after discharge.
Statistical Analysis
All analyses were performed using SAS Version 9.4 (Cary, North Carolina, USA). Univariate associations were calculated using Fisher’s exact tests for categorical information and t-tests for continuous variables. A multivariable logistic regression model was created to identify associations with discharge to facilities other than home and to adjust for confounders. Patients were stratified into two age groups: younger than 65 and 65 or greater. BMI in kg/m2 was stratified based on weight classification (<20 underweight, 20-30, and > 30 overweight). For the univariate analysis, significance was set at P < .05. For the multivariable model, all covariates with P < .05 in the univariate analysis were included for multivariable regression, which took into account demographics, comorbidities, complications, and other perioperative and surgical variables. Odds ratios (ORs) with their associated 95% confidence intervals (CIs) and P values were reported from these models.
Results
Between 2011 and 2016, a total of 13,093 patients underwent open repair of distal radius fractures. Of these patients, 12,001 had complete information for their discharge destination and were included in our analysis. Of these 12,001 patients, 73.1% identified as female (n = 8771), 26.9% as male (n = 3230), 74.5% as White (n = 8937), and 25.53% as another race or ethnicity (eg Native American or Alaska Native, Asian, Black or African American, Native Hawaiian or Pacific Islander, Hispanic or Latino, n = 3064). Of all patients, 3.24% (n = 389) were discharged to facilities other than home.
Associations between patient demographics, comorbidities, perioperative and surgical variables, and discharge destination are shown in Table 1. Univariate regression analysis revealed that patients discharged to home versus a post-acute care facility other than home varied significantly in age, sex, race, and ethnicity. Patients discharged to facilities were older by an average of 18 years (74.8 ± 12.4 years vs 56.3 ± 16.4 years, P < .001). Both female and White patients were more likely to undergo ORIF for distal radius fracture and require subsequent discharge to a facility. Patients who resided in nursing homes or were already admitted to a hospital prior to surgery and patients who had perioperative anemia or hypoalbuminemia were also more likely to discharge to facilities other than home. Comorbidities associated with discharge to facilities included underweight BMI, diabetes, hypertension, COPD, dyspnea, heart failure, preoperative steroid use, bleeding disorders, and ASA classification greater than 2. Smokers were less likely to be discharged to facilities other than home. Operative variables associated with discharge to a facility other than home included emergency surgery, bilateral surgery, intra-articular comminuted fractures, and wound classification other than clean. Patients who suffered a complication prior to discharge were also significantly more likely to require discharge to a facility other than home.
Patient Demographic, Preoperative, and Intraoperative Characteristics Between Discharge Destination Groups (N = 12,001).
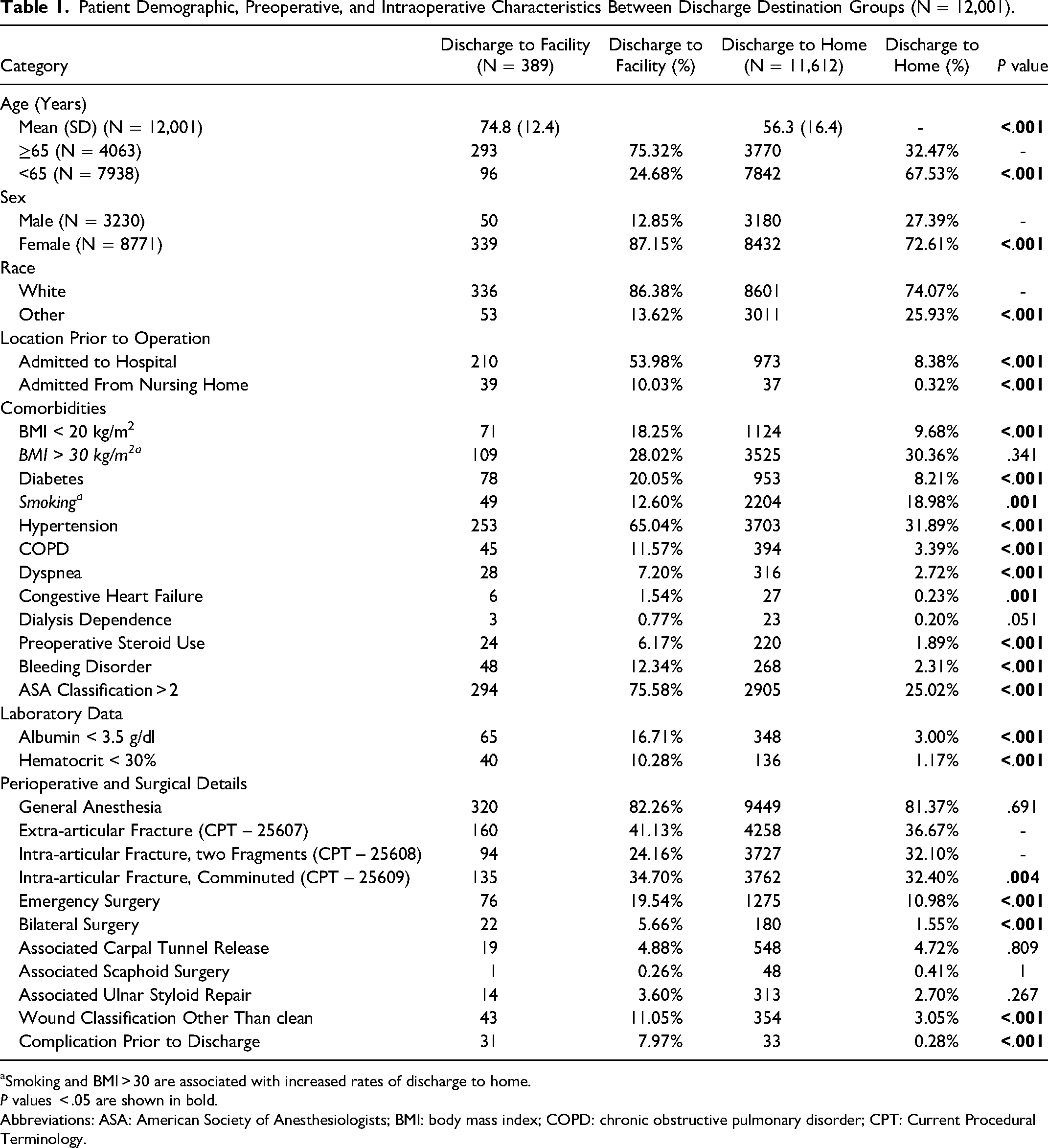
Smoking and BMI > 30 are associated with increased rates of discharge to home.
P values < .05 are shown in bold.
Abbreviations: ASA: American Society of Anesthesiologists; BMI: body mass index; COPD: chronic obstructive pulmonary disorder; CPT: Current Procedural Terminology.
On multivariate regression analysis, multiple risk factors were independently associated with discharge to a facility other than home after controlling for other variables (Table 2). Age greater than 65, White race, underweight BMI, preoperative steroid use, ASA classification > 2, admission from a nursing home or already admitted to the hospital, anemia, bilateral surgery, and complications prior to discharge were independently associated with higher odds of being discharged to a facility other than home. Smokers and patients with BMI greater than 30 were more likely to be discharged home than to other facilities.
Multivariate Analysis of Patients Undergoing Discharge to Post-Acute Care Facilities.
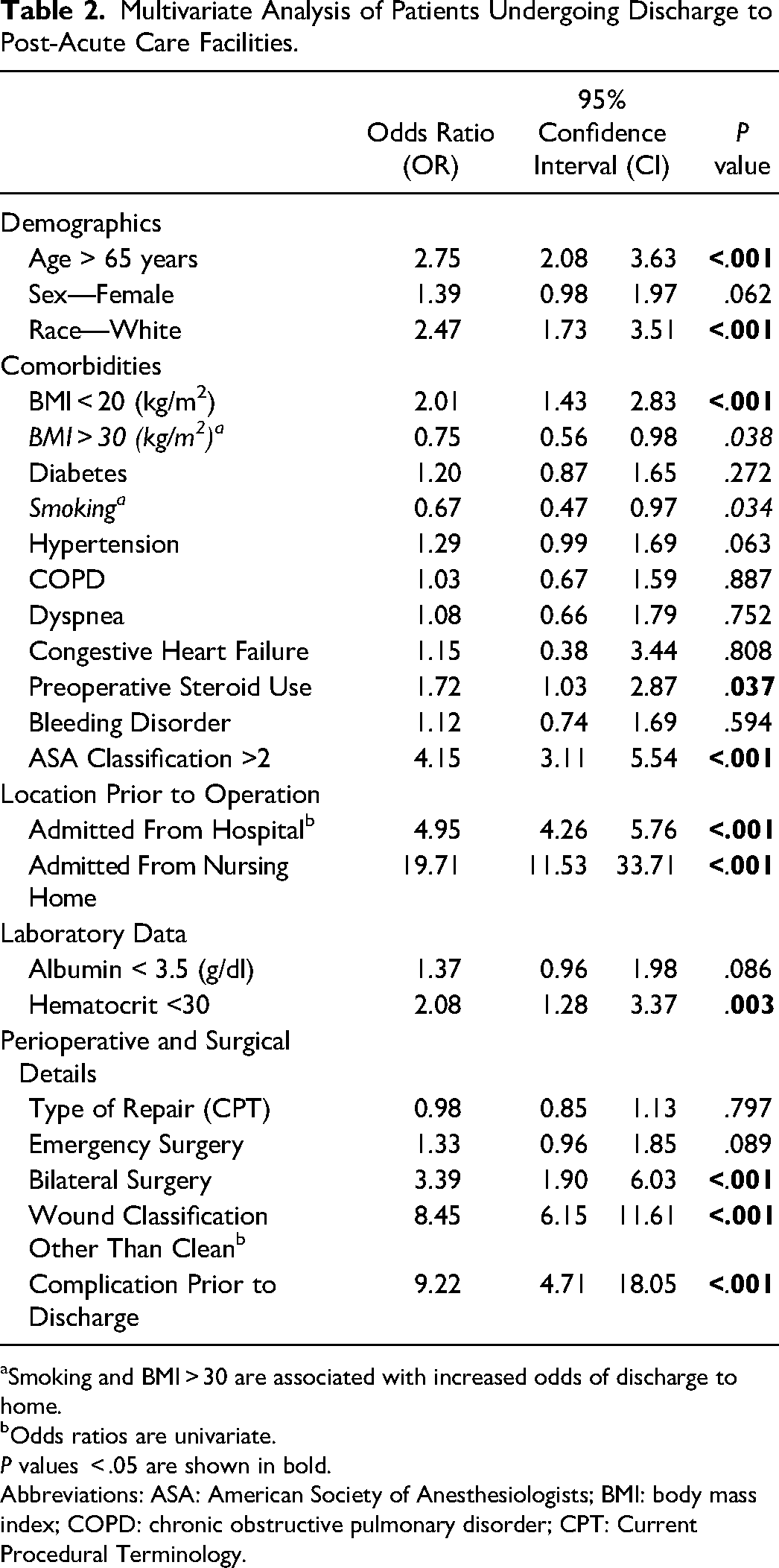
Smoking and BMI > 30 are associated with increased odds of discharge to home.
Odds ratios are univariate.
P values < .05 are shown in bold.
Abbreviations: ASA: American Society of Anesthesiologists; BMI: body mass index; COPD: chronic obstructive pulmonary disorder; CPT: Current Procedural Terminology.
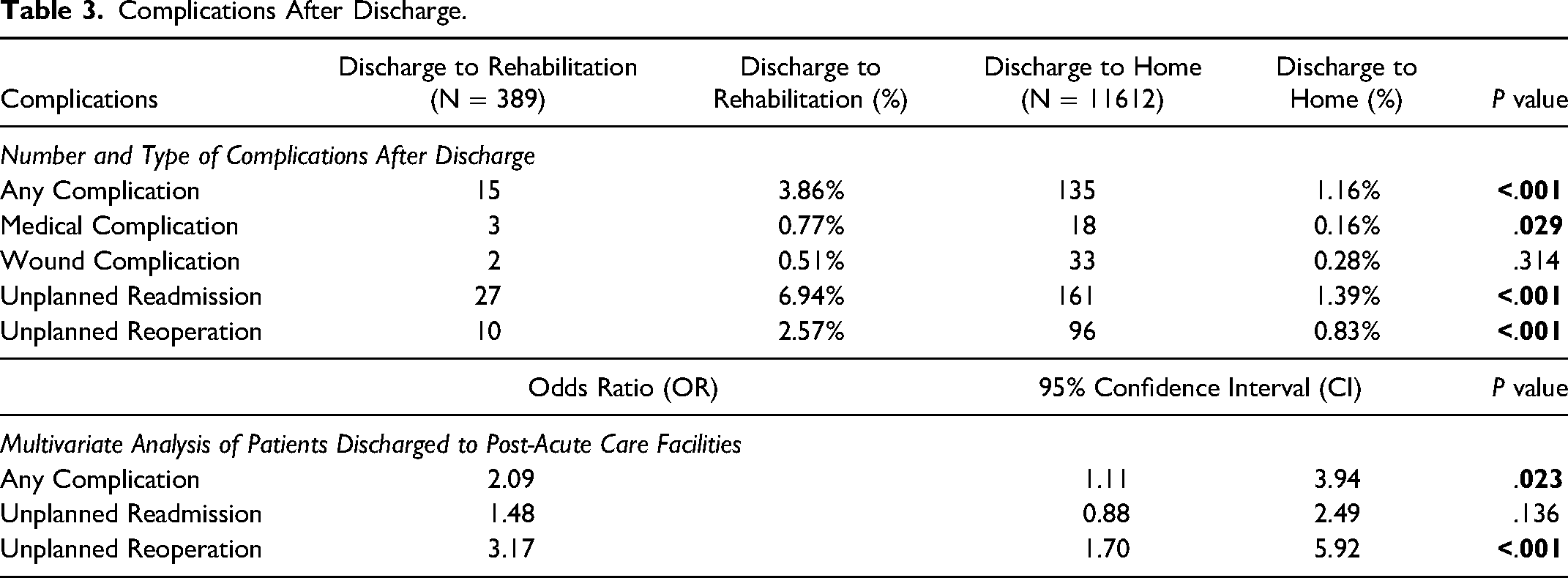
After patients were discharged from the hospital, univariate regression analysis showed that patients at post-acute care facilities were more likely to suffer unplanned readmissions, unplanned reoperations, and medical complications than patients who were discharged home (Table 3). On multivariate analysis, patients at facilities other than home were more likely to develop all complications (OR: 2.09, 95% CI: 1.11-3.94) and require unplanned reoperation (OR: 3.17, 95% CI: 1.70-5.92), but unplanned readmissions were not significantly more likely (OR: 1.48, 95% CI: 0.88-2.49).
Complications After Discharge.
Discussion
The primary goals of this study were to identify risk factors that predispose patients undergoing ORIF for distal radius fracture to discharge to a post-acute care facility and to examine how discharge to a post-acute care facility affects value-driven outcomes. This study is the first to examine variables associated with patient discharge to facilities other than home after ORIF of distal radius fractures. Through our multivariate analysis controlling for demographic variables, comorbidities, and operative factors, we identified several factors which were independently associated with increased risk of discharge to a facility other than home. These include age greater than 65, White race, underweight BMI, preoperative steroid use, ASA classification > 2, admission from a nursing home or already hospitalized, perioperative anemia, bilateral surgery, wound classification other than clean, and complications prior to discharge. Several patient variables that were significant in univariate analysis were not shown to be significant when controlling for other variables. These included female sex, diabetes, hypertension, COPD, CHF, bleeding disorders, hypoalbuminemia, and type of repair (CPT code).
Distal radius fractures requiring ORIF were most common in White females aged 65 and older. Increased distal radius fracture risk in this demographic has been attributed to a greater risk of osteoporosis. 14 While female sex is associated with both an increased risk of fracture and discharge to post-acute care facility with univariate analysis, our multivariate analysis revealed that female sex was not independently associated with a higher risk of discharge to a post-acute care facility. Patients over 65 years of age had almost three times greater odds of being discharged to a facility other than home. This correlation likely has multiple contributing factors including increased comorbidities, decreased functional status, and decreased physiologic reserve.15–17 Elderly patients have not been found to have increased complication rates, but they do have an increased need for post-acute care.18,19 Across multiple specialties, advanced age is often the strongest predictor of discharge to post-acute care facilities and should be strongly considered as soon as discharge planning is initiated.20–22 Functional status and ASA classification greater than 2 have been shown to be associated with increased early complications,18,19 and our study confirms them as significant factors influencing discharge location.
During the informed consent process, surgeons and patients often have discrepancies in what aspects of care they think are important. Patients and their families are more concerned with the long-term quality of life and functional or esthetic outcomes rather than technical surgical details.23,24 Discharge destination after surgery is one of the factors likely to influence these concerns and is often ignored during the informed consent process. 25 By discussing a patient's risk factors with them, healthcare providers can identify patients who will have higher post-acute care needs, make shared decisions about next steps, and arrange for more efficient and cost-effective transfers.
Some of the most targeted areas for cost reduction in healthcare are reducing complications, hospital lengths of stay, and readmission rates. 26 Post-acute care facilities are gaining popularity as they allow more complex patients to be safely discharged from the hospital prior to a full recovery with potentially more cost-effective care, but these facilities must also improve patient outcomes to add value to the healthcare system. As healthcare providers, the benefits of discharge to post-acute care facilities must be carefully considered to select the appropriate patients and avoid overutilization and unnecessary costs.7–9 The overall rate of discharge to a post-acute care facility was 3.24% in our dataset compared to 13.4% of patients reported across multiple surgical specialties in a large database study. 10 Our analysis showed that complications and unplanned operations after discharge were significantly more common among patients who were discharged to post-acute care facilities than to home. These patients had reduced health at baseline, comorbidities, more complex surgical reconstructions, and hospital courses, all likely contributing to an increased rate of complications and unplanned reoperations. Discharge to a post-acute care facility did not significantly reduce the risk of developing complications after discharge, prevent the need for unplanned reoperations, or influence the rate of hospital readmissions compared to discharge to home. It is unclear how many more patients would have developed complications or required an unplanned reoperation if they had been discharged home, where they might be less likely to recognize early signs of a complication that would require surgery.
There are several limitations of this study. As with all large database studies, it can be prone to coding errors and misclassifications. The NSQIP database does not collect data on home health care, which likely results in an underestimate of post-acute care services. Our dataset did not specify which type of nonhome facility patients were discharged to (eg skilled, unskilled, separate acute care, or rehabilitation facility) which also likely influences the risk of developing postoperative complications and the need for readmission or reoperation. Additionally, as a national database, NSQIP does not allow for institutional data to be extracted, the location disparities and disparities in urban and rural settings are not able to be assessed as they have shown to play a role in post-acute care utilization.27,28 Patient support systems, social situation, insurance, and socioeconomic status factors may also affect postoperative discharge destination and were not assessed due to limitations of the database. Lastly, as NSQIP only assesses those who underwent surgery, we are not able to determine the utilization of post-acute care resources for those distal radius fractures treated non-operatively. Despite the above limitations, we believe this study offers important insight into the utilization of post-acute care after ORIF of distal radius fractures. Further studies are needed to explore differences in complications of high-risk patients discharged to home compared to those discharged to post-acute care facilities, and differences in complications by the type of post-acute care facility utilized.
Conclusion
While a small minority of patients require discharge to post-acute care facilities after ORIF of distal radius fractures, these patients are at the most risk for complications and overutilization of healthcare resources. An understanding of the risk factors that predict discharge to a post-acute care facility and the subsequent outcomes for those patients compared to patients who were discharged to home is required to appropriately inform patients, manage expectations, and facilitate efficient and safe transfers. Among patients undergoing ORIF for distal radius fracture, discharge to post-acute care facilities appears to be reserved for appropriate patients, but does not make a significant difference in key value-driven outcomes and may be an area for further cost reduction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Ethical Approval
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008 (5). Informed consent was obtained from all patients for being included in the study.