
Abstract
Introduction
Maxillofacial reconstruction with a fibula-free flap is a complex process involving multiple steps. It is critical to estimate the exact length of the flap and surgical mandible margins to achieve optimal anatomical and functional results. 1
The fibula-free flap method described in 1975 by Taylor et al. is the conventional surgery method (CS), 2 based on surgeons’ experience calculating the flap cuts, number of fragments, and mandibular landmarks during surgery. However, the morphological differences between the maxillary and mandibular bone and the fibula flap fragment hinder the surgical procedure, compromising functional and aesthetic results. 3
Since technology improvements, there are currently methods such as Computer-Aided Design (CAD), Computer-Aided Manufacturing (CAM), and Additive Manufacturing (AM) to correctly process CT images and generate 3D printed models of mandible and fibula.4,5 Once the 3D model is designed; It is manufactured with a 3D printer, sterilized, and then brought into the operating room to improve precision, control, and length of surgical time compared to standard techniques.6,7 This type of technology provides a better understanding of the procedure, allowing it to be efficient and effective. It is necessary to objectively demonstrate the impact of this technology on surgical time and other secondary outcomes such as bleeding and hospital stay.
Virtual surgical planning has demonstrated a significant reduction in intraoperative time and aesthetic outcomes compared to the conventional technique. 5 Nevertheless, access to this form of surgical planning is difficult due to the infrastructure and software needed to achieve it.
This study aimed to explore a low-cost solution for virtual surgical planning/3D printed surgical guides in a training hospital, assessing the impact on intraoperative time and bleeding.
Material and Methods
Participants
We included in this retrospective study all the patients in our institution who underwent maxillofacial reconstruction surgery with fibula-free flap utilizing virtual surgical planning/3D printed guides from 2017 to 2020. We applied a survey to the surgeons involved in the surgical procedures. We also collected a control group using the traditional method from the same period.
Imaging Acquisition
Computed Tomography and Angiography
Maxillofacial bones and fibula CT images were acquired utilizing a General Electric CT99 Lightspeed VCT scanner, slice thickness of 1.25 mm, 120 kVp with standard reconstruction algorithm. We performed a CT angiography of the lower extremities to localize the perforator peroneal arteries for faster identification during the surgery.
Segmentation of Anatomical Structures
Segmentations were performed in 3D Slicer V4.8.0, V4.8.1, 4.10.0, 4.10.1, and 4.10.2. The “threshold” tool was initially utilized to achieve automatic segmentation of the bone structures, and then manually correction was applied slice by slice to obtain the 3D digital models of the upper maxilla and/or mandible according to the case. Furthermore, a 3D model of the fibula was also obtained in every case. All the 3D digital models were exported to STL files for virtual planning purposes (Figure 1).
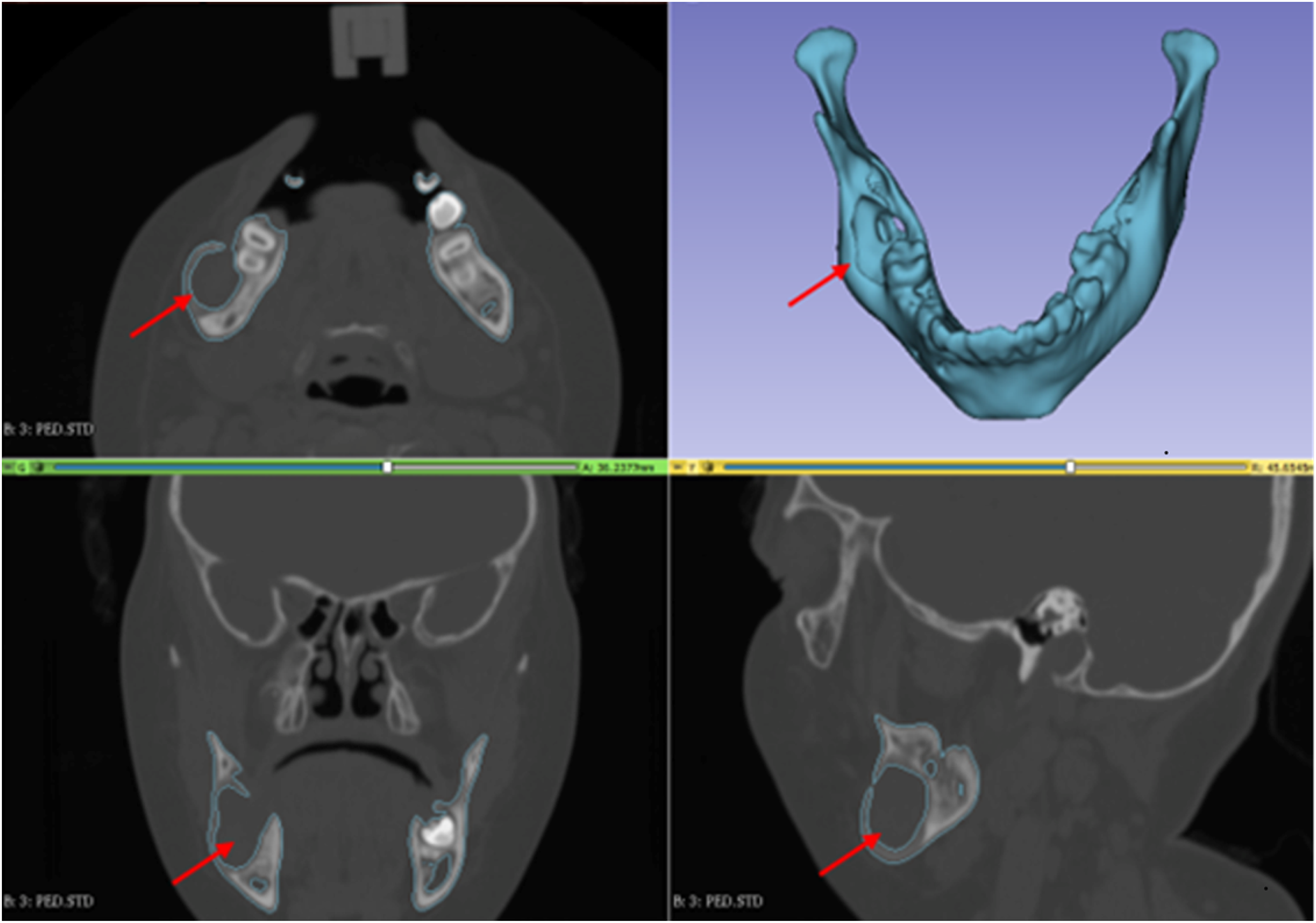
Screenshot showing the segmentation process using 3D slicer software of a patient with right mandible angle ameloblastoma (arrows).
Virtual Surgical Planning
Mesh Correction and Reduction
The 3D digital models underwent a mesh correction and reduction of triangles comprising the 3D digital mesh using Autodesk Meshmixer 3.5.474.
Virtual Incisions Simulation and Surgical Guide Generation
According to the plan of the plastic surgeon in charge of the operation, we generated appropriate surgical guides to reproduce the planned incisions employing Solidworks 2017 (Dassault Systemes, United Kingdom) (Figures 2 and 3).
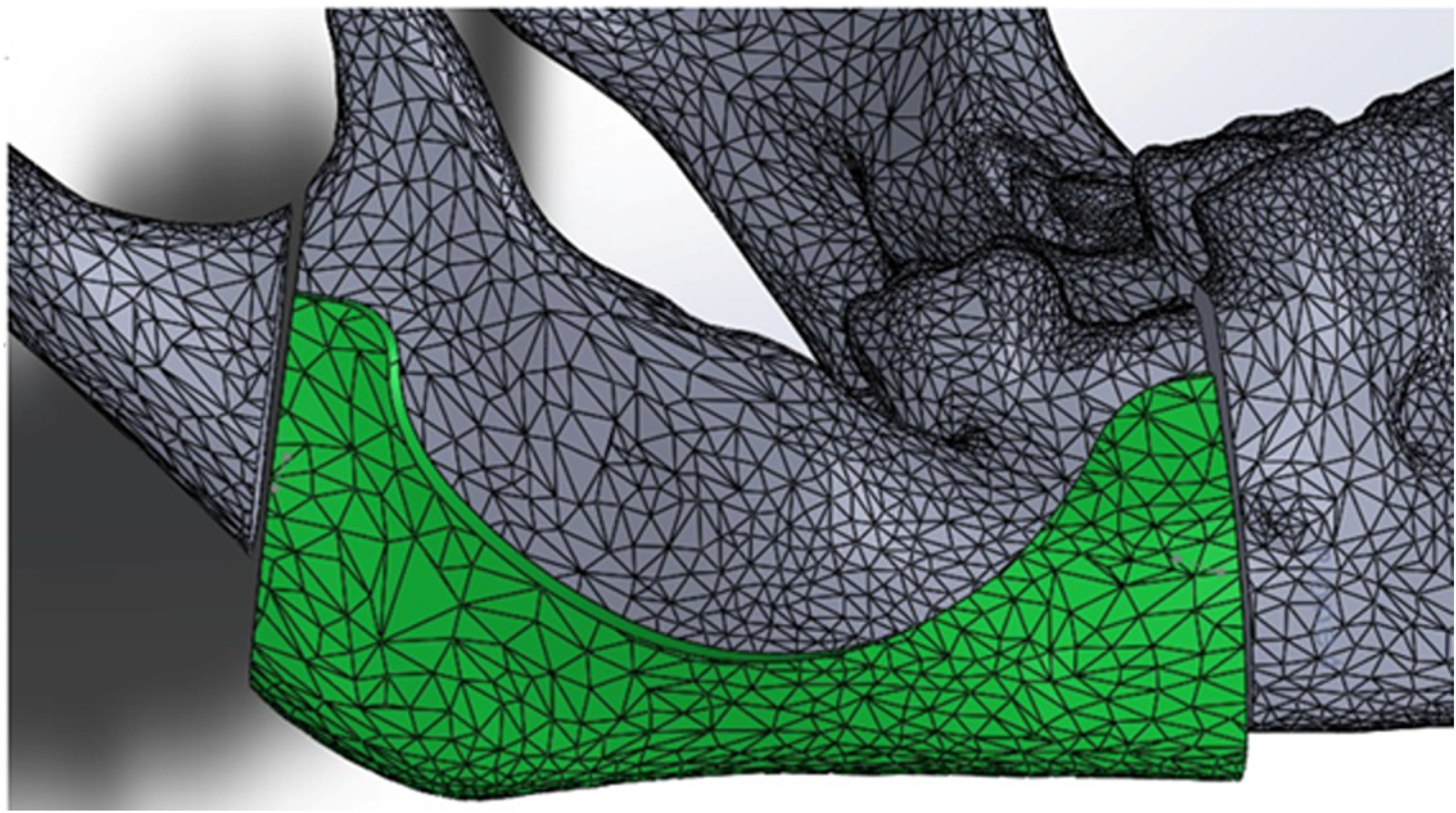
Screenshot showing the designing process for a customized surgical guide for the mandible utilizing Solidworks Software.
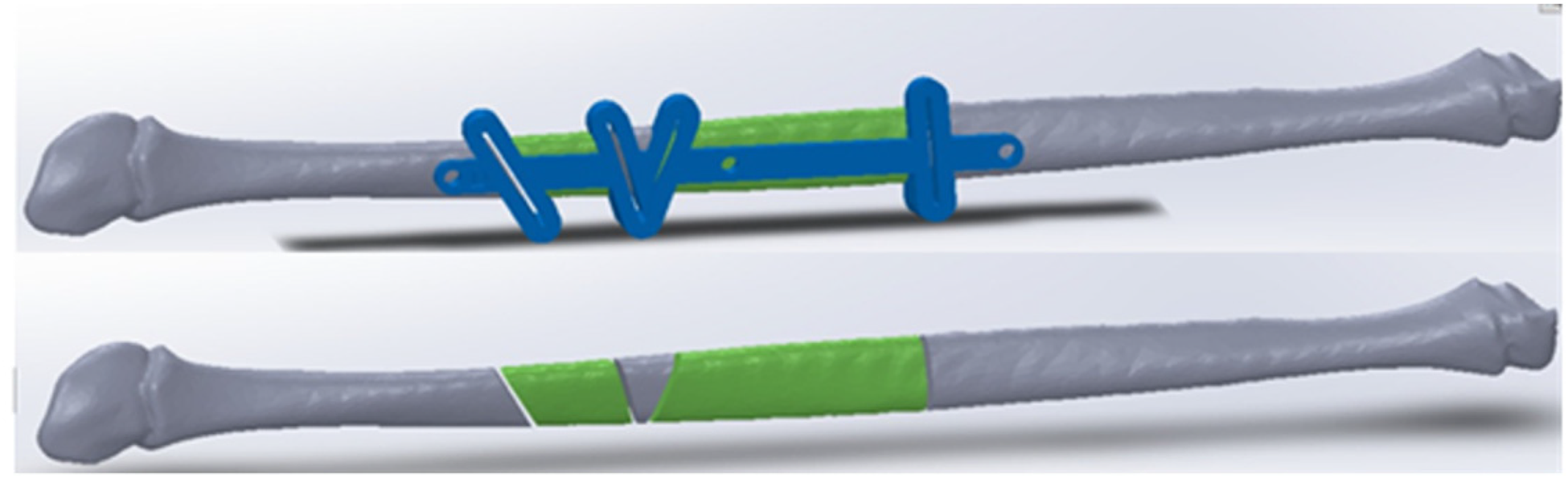
Screenshot showing the designing process for a customized surgical guide for the fibula utilizing Solidworks Software.
Then we reproduced a virtual simulation of the mandible with the proposed reconstruction using the surgical guides (Figure 4).
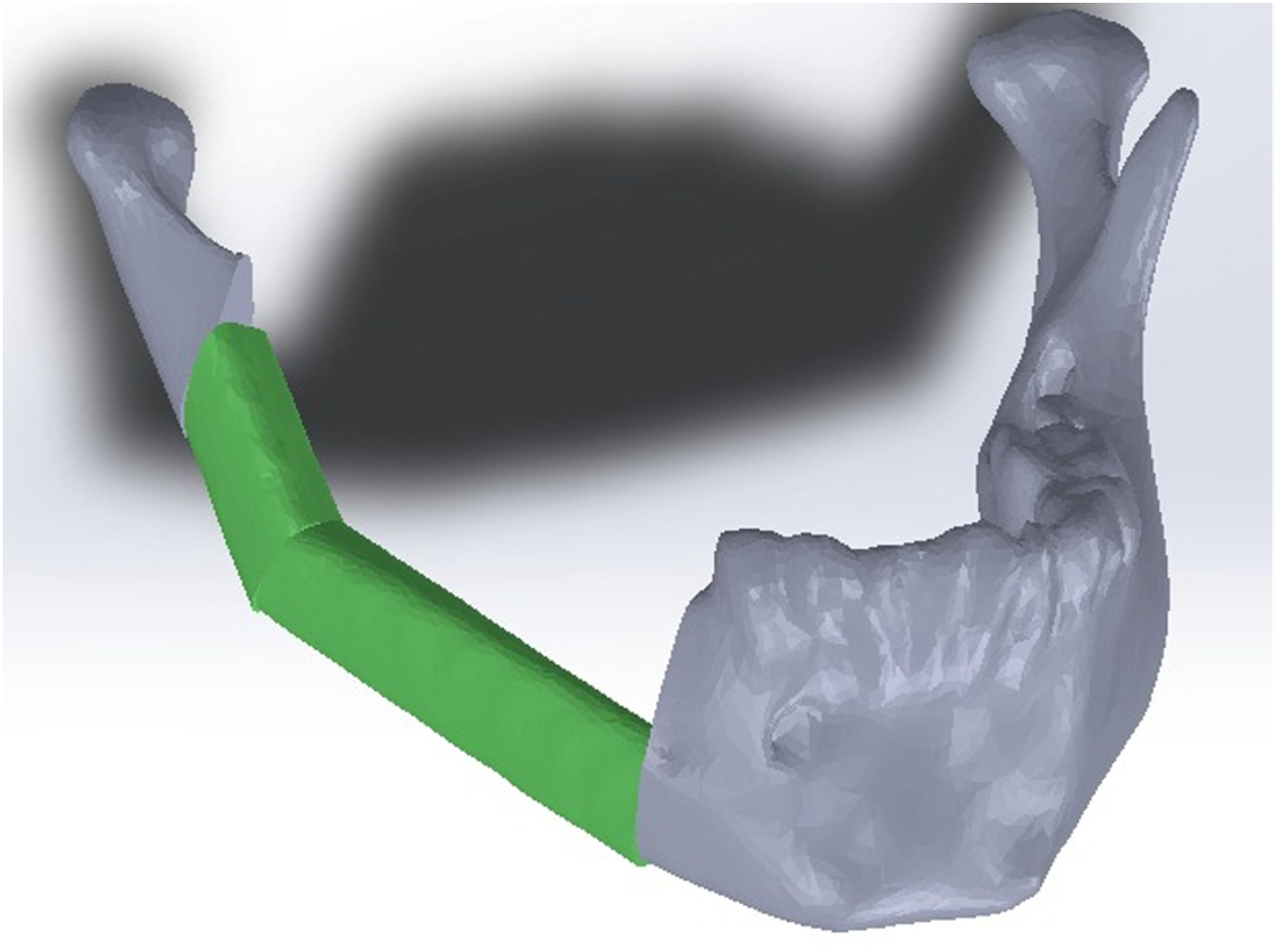
Screenshot showing the proposed reconstruction.
3D Printing Process
We printed the anatomical models and the surgical guides of each case utilizing a Zortrax M200 (Zortrax, Poland) and the material Z-Ultra ABS (Zortrax, Poland) (Figure 5).
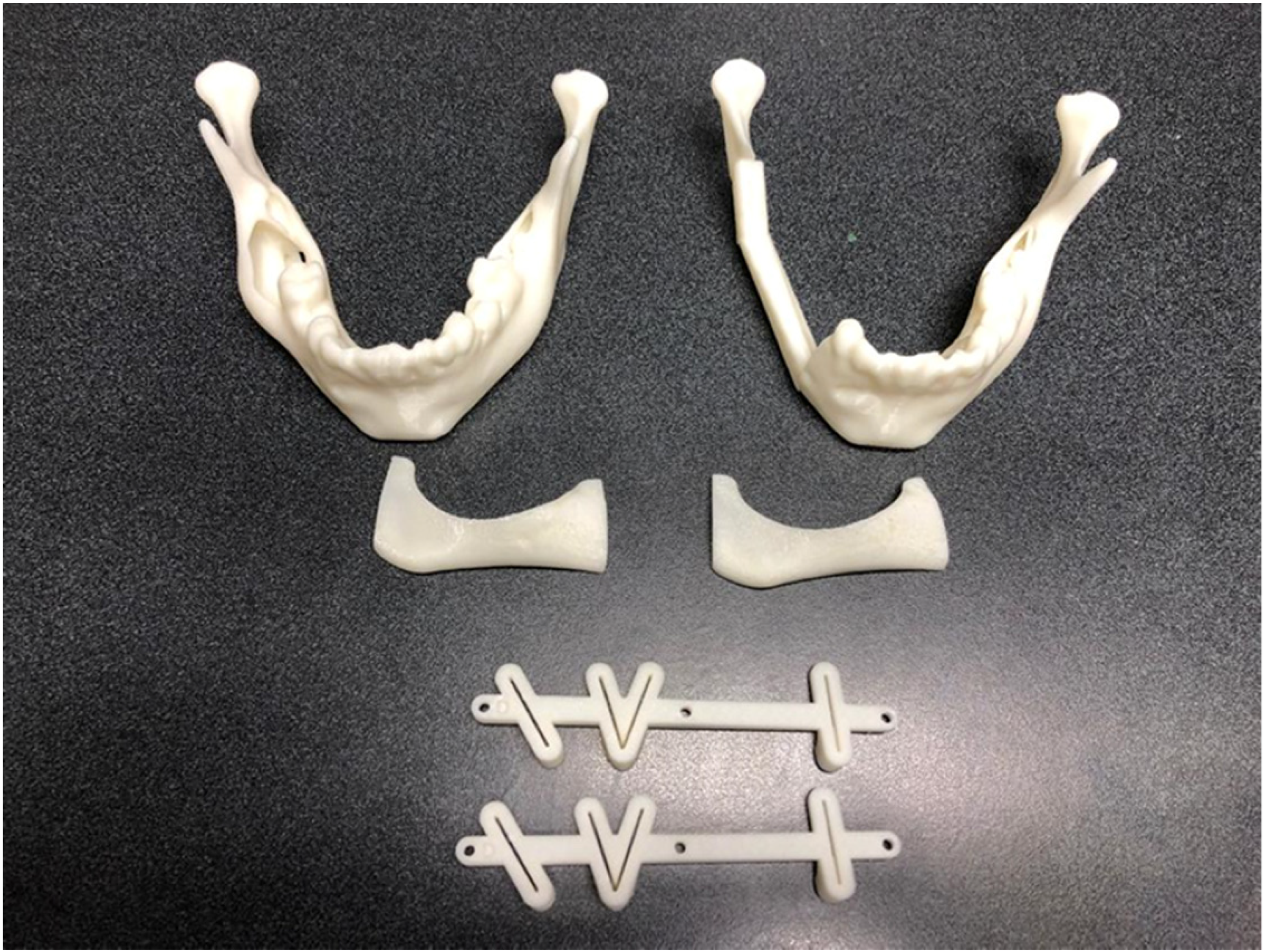
Picture showing the finalized 3D printed models and surgical guides ready for the sterilization process.
The titanium plates were pre-molded in all the cases to bypass this step during surgery.
Scarce technical support is required when using 3D printers and printing material of the same brand because the correct parameters are already defined.
Sterilization Process
We sterilized the anatomical models and the surgical guides using the hydrogen peroxide gas plasma. 8
Preparation Before Surgical Procedure
Before every surgical procedure, we accomplished two sessions of 20 minutes during the programed plastic surgery ground rounds to discuss the position of the surgical guides and any additional technical requirements. The whole process of VSP required an average of 1 week of work before surgery with a mean time of one hour per day.
Data Collection
We collected the following information from the clinical record:
Total time of the surgical procedure, bleeding during the surgery measured in mL, indication for the surgery, the length of hospital stay, and comorbidities.
Quality Assessment of the 3D Printing Models and Guides
All surgeons participating in the maxillofacial reconstruction surgery with fibula-free flap utilizing virtual planning/3D printed guides from 2017 to 2021 were submitted to an online survey delivered via Google forms. The survey included questions on surgeons’ preference for either doing the surgery utilizing the virtual planning/3D printed guides or by the traditional method and comparing the surgical time, confidence at the time of surgery, and the results of both surgical procedures.
We included 12 questions directed to the plastic surgeons and 10 to the otorhinolaryngologists.
We scored all the questions in the survey on a 5-point Likert scale (1: strongly disagree, 2: disagree, 3: neutral, 4: agree, 5: strongly agree).
Statistical Analysis
We utilized a T-test for assessing the differences between groups in operative time and bleeding. After the latter, we applied a linear regression adjusting by age, gender, bleeding, and comorbidities for bias reduction. We used linear regression to explore the correlation between bleeding volume and surgical time, taking a p-value<0.05 significant for all the tests.
We performed all the statistical analysis and graphics utilizing Stata 16 Software (StataCorp. 2019. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC.)
Results
Patients and Postoperative Data
This study included 13 patients that underwent maxillofacial reconstruction surgery, 8/13 (61.53%) utilizing virtual planning (VP) and 3D printed surgical guides (SG) that we called the VP/SG group, and 5/13 (38.46%) underwent conventional surgery (CS) called CS group. Gender distribution was 9/13 (69.23%) women and 4/13 (30.76%) men with a mean age of 44.5 ± 19.5 years.
Four out of the eight (50%) patients in the VP/SG group presented comorbidities, of which 2 of them presented diabetes and hypertension, another presented diabetes and smoking, and the other was smoking. On the other hand, 3/5 (60%) patients in the CS group presented comorbidities, of which 2 of them presented smoking and the other one diabetes. Patients’ characteristics are shown in Table 1.
Demographic and clinical characteristics of patients.
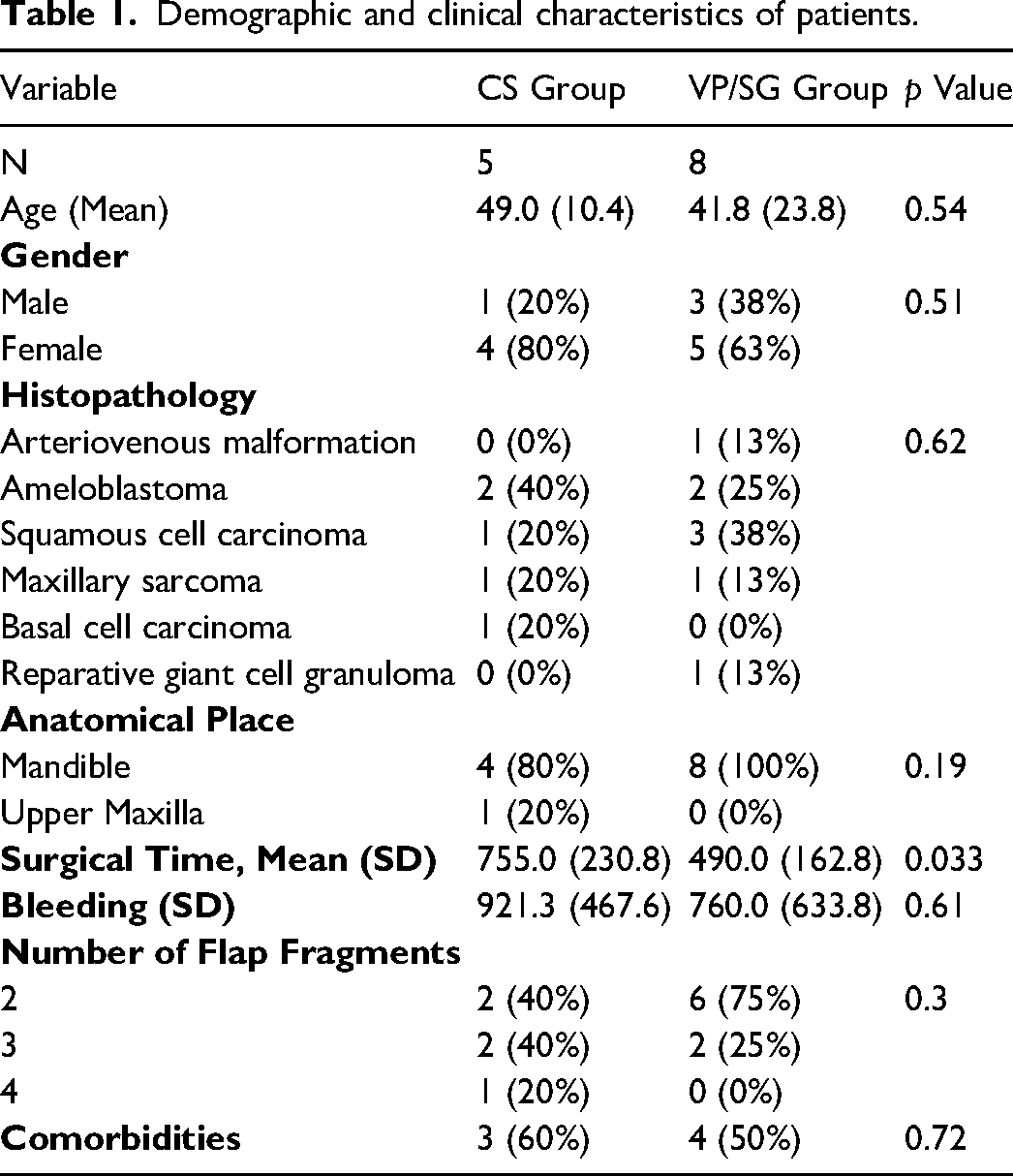
The average printing time (surgical-guides and mandibular anatomical models) was 13.72 ± .69 hours. The mean surgical time in the VP/SG group was 8.16 ± 2.7, compared to the CS group 12.5 ± 3.8, showing a 4.34 hours difference with statistical significance (p = 0.033). Patients from the CS group had a higher bleeding volume of 921 ± 467.6 mL VS 760 ± 633.8 mL in the VP/SG group without reaching statistical (p = 0.61).
We did not find significant differences between groups in the following variables: age, sex, histopathology, anatomical place, and comorbidities. We present a comparative table of both groups in Table 1.
We performed multivariate analysis for assessing the difference in surgical time between groups adjusting by age, gender, bleeding, and comorbidities finding an independent correlation between using VP/SG and reduced surgical time p = 0.021 (Table 2). A second multivariate analysis to find a correlation between bleeding and surgical time showed an increment of 14 seconds per milliliter of bleeding p = 0.044 (Table 3).
Multivariable linear regression of surgical time.

Multivariable linear regression of surgical time and bleeding.

The average cost for the complete surgical planning and 3D printed guides was 914.44 ± 46.39USD. This calculation includes the Computed tomography of the lower extremities and skull, materials, and 3D printing time. The radiologist and engineer compensations are not included in the cost calculation as they are part of their daily activities. The cost of the 3D printer used in this work rounds 2000 USD, plus an appropriate custom-made PC of 1700 USD.
Likert Scale
A total of 8 surgeons answered the online survey, 5/8 (62.5%) were plastic surgeons, and 3/8 (37.5%) were otorhinolaryngologists.
Four out of the five (80%) plastic surgeons felt more confident performing the surgery utilizing the 3D printed guides/virtual planning, 1/5 (20%) were neutral. One out of the three (33.3%) otorhinolaryngologists felt more confident using the 3D printed guides/virtual planning, and 2/3 (66.7%) felt neutral about it.
All the plastic surgeons 5/5 (100%) and 2/3 (66.7%) of the otorhinolaryngologists agreed that the surgical time was less utilizing the 3D printed guides/virtual planning against the traditional method.
Four out of the five (80%) plastic surgeons were satisfied with how the surgical guides adapted to the fibula bone, and 1/5 (20%) was neutral.
Two out of three (66.7%) otorhinolaryngologists were satisfied with how the surgical guides adapted to the mandibular bone, and 1/3 (33.3%) was neutral.
All the surgeons (otorhinolaryngologists and plastic surgeons) preferred to perform the procedure utilizing the 3D printed guides/virtual planning, and they all agreed that they would always use them when available. Eight out of the eight (100%) would recommend the 3D printed guides/virtual planning to their colleagues and their patients.
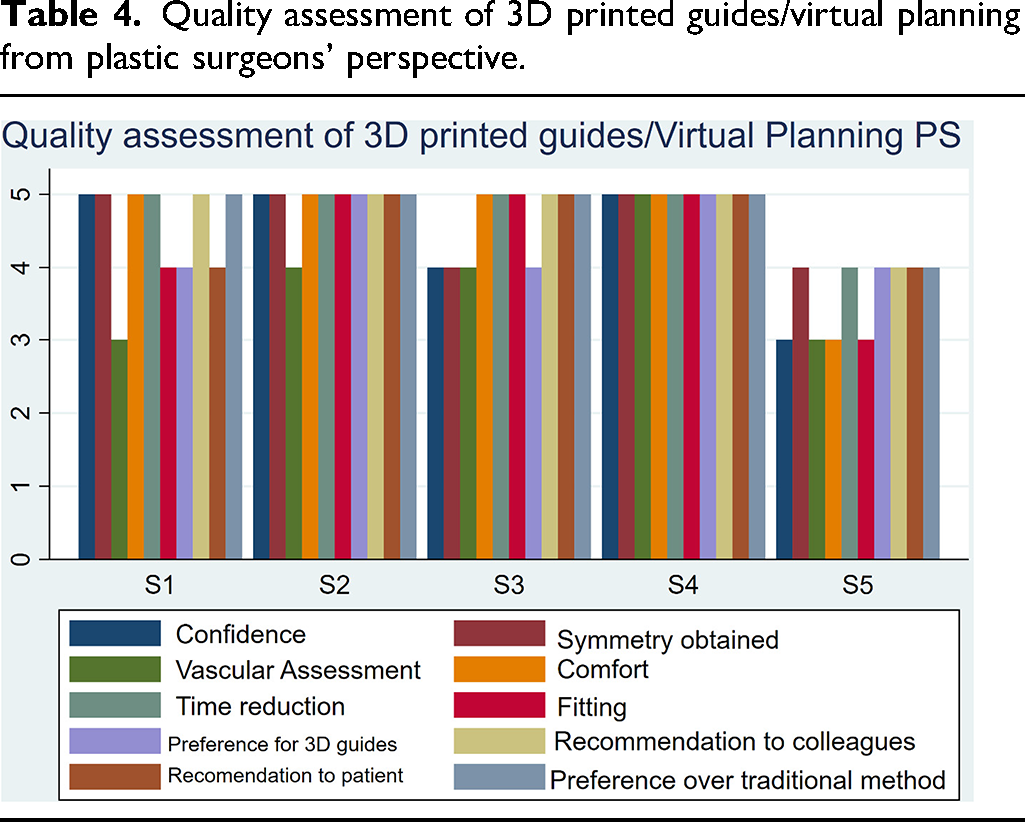
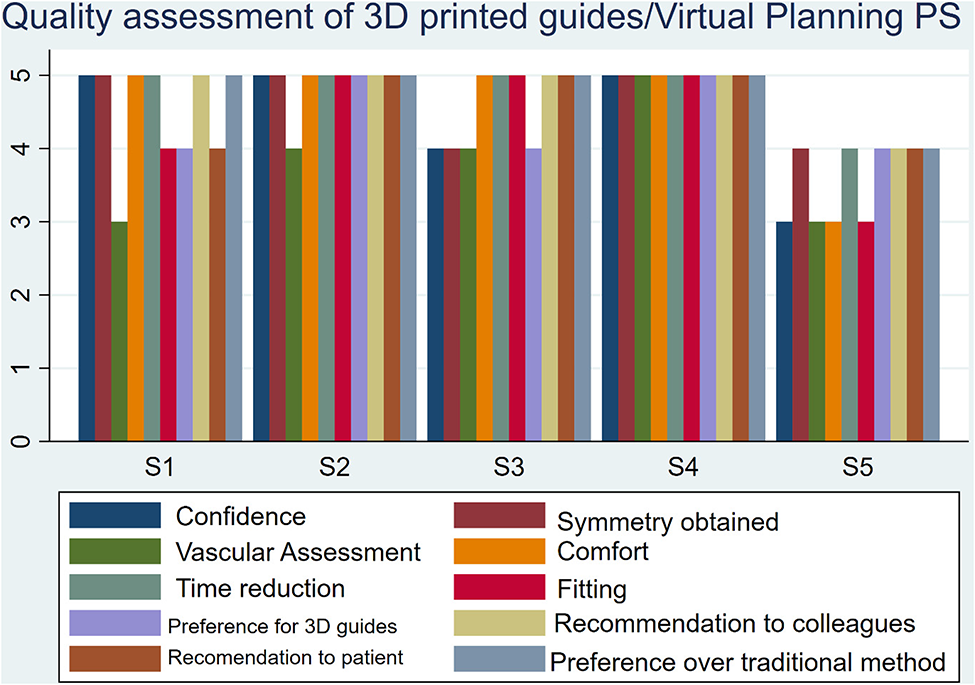
For the plastic surgeon group, the average score was: 4.40 for confidence level, 3.80 for vascular assessment, 4.80 for time reduction, 4.40 for 3D guides preference, 4.60 for recommendation to the patient, 4.60 for symmetry obtained, 4.60 for comfort, 4.40 for fitting, 4.80 for recommendation to colleagues, and 4.80 for preference over the traditional method.
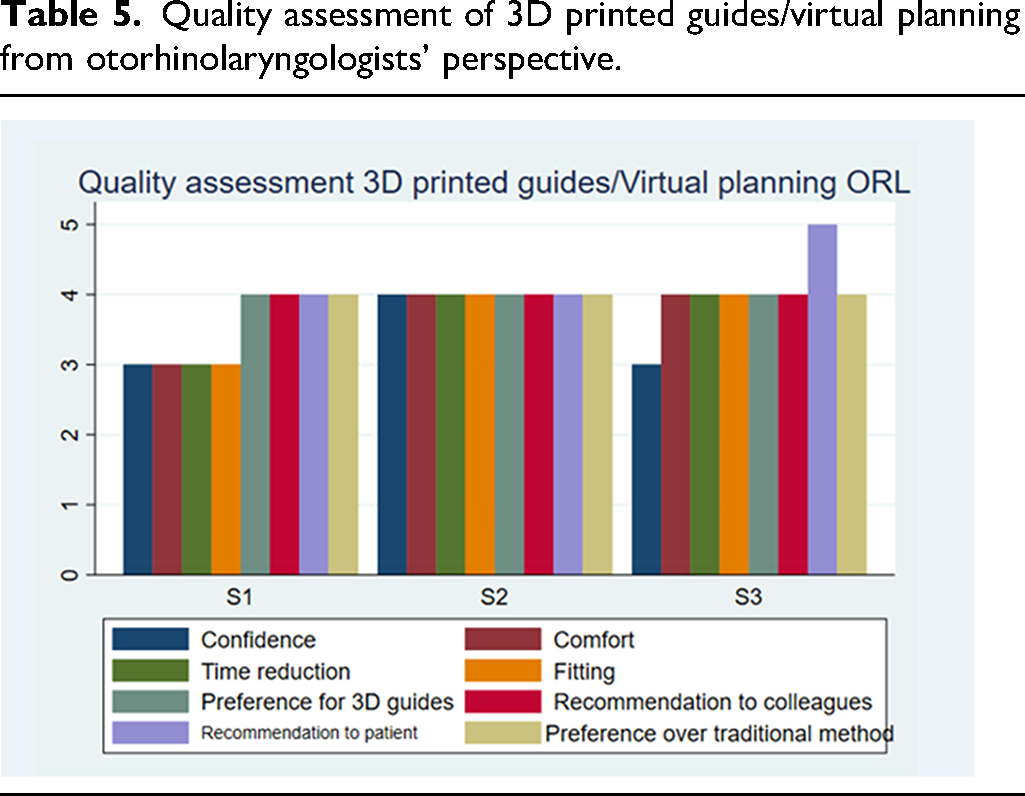
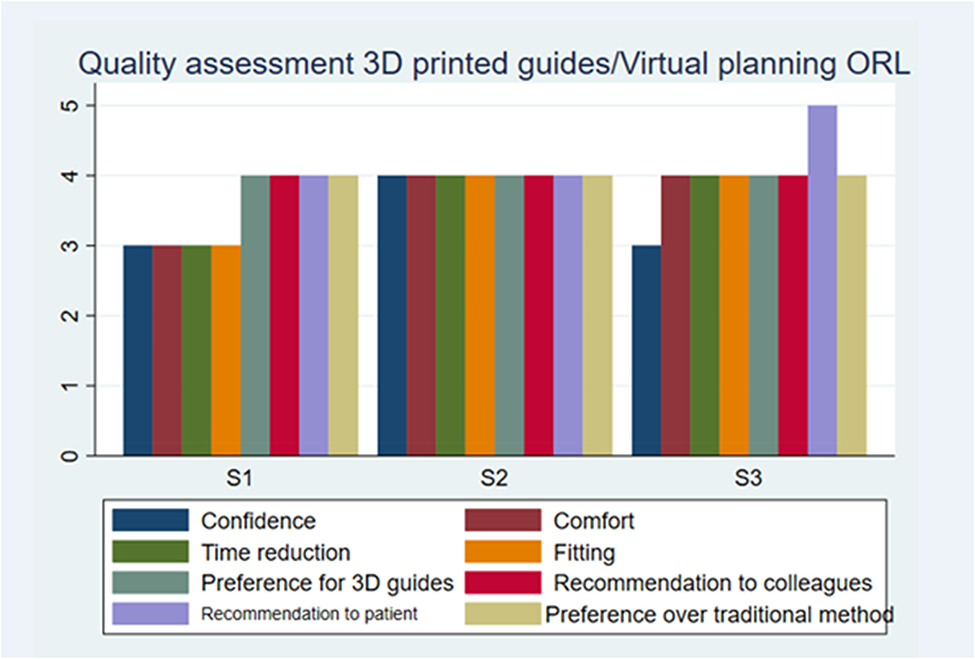
For the otorhinolaryngologist group, the average score was: 3.33 for confidence level, 3.66 for time reduction, 4.00 for 3D guides preference, 4.33 for recommendation to the patient, 3.66 for comfort, 3.66 for fitting, 4.00 for recommendation to colleagues, 4.00 for preference over the traditional method.
A couple of questions were answered only by the plastic surgeons. Five out of five (100%) were satisfied with the symmetry obtained. Three out of five (60%) were pleased with the localization of the peroneal arteries using tomography and Doppler ultrasound. Tables 4 and 5 summarize the results of the survey.
Quality assessment of 3D printed guides/virtual planning from plastic surgeons’ perspective.
Quality assessment of 3D printed guides/virtual planning from otorhinolaryngologists’ perspective.
Comments of the surgeons were as follows: “Innovative, avant-garde, completely satisfied with its use and results.”, “Excellent work tool. Definitely”, “All excellent, keep up the good work!”, “It is adequate.”
To obtain sufficient experience to perform the complete VSP, the team went through a 4-month training period, simulating, and validating each step in hospitalized patients but without reaching the application in the operating room. The lessons learned were that coordination between surgical teams and accurate communication are essential to obtain the desired results. Scarce technical support is required when using 3D printers and printing material of the same brand because the correct parameters are already defined.
Discussion
The use of vascularized bone flaps has become the gold standard for mandibular reconstruction.9–11 The fibula flap is the workhorse for mandibular reconstruction due to its thickness, length, and bone uniformity, providing an adequate alveolar ridge ideal for dental implants.12–14 However, some challenges are accompanying this procedure, such as the difficulty to obtain an accurate shape of the vascularized bone flap to obtain facial symmetry, preserve the function, and minimize the operative time.
Conventional techniques for mandibular reconstruction rely on the surgeons’ experience and lack of quantitative analysis. Virtual surgical planning utilizing computer-aided design has changed the paradigm of bony reconstruction techniques in recent years, reducing operating time and improving facial symmetry.7,15,16
In this study, we found that VP/SG reduces the operative time during maxillo-facial reconstruction surgery. Furthermore, the intervention group had fewer bleeding volumes, although it was not significant. It is one of the few studies bringing a cost-effective solution reducing operating time with in-house VP/surgical guides.17,18
Some authors reported a significant reduction in operating time in previous studies using virtual planning and 3D-printed surgical guides ranging from 24 to 84 minutes.12,15,19 A recent systematic review and meta-analysis demonstrated that a virtual planning method access shorter ischemic time, reconstructive time, total operative time, and length of stay versus the traditional method. 3 In our study, there was a mean reduction of 240 minutes. The fact that the participants were residents in training might explain the higher reduction in time observed. Elegbede et al. found that utilizing a surgical guide impacts the operative time more strongly in someone without experience than in someone who masters the technique. 20
We adjusted the analysis by age and comorbidities of the patients to employ a linear regression. Therefore, reducing possible bias and demonstrating that the surgical guides/virtual planning remained significant and independent.
We found a positive correlation between the bleeding volume and the surgical time. We observed an increment of 14 seconds per milliliter of blood loss. Although, the small sample size and broad standard errors obtained in our study prevent us from making solid conclusions. Nevertheless, it is intuitive that adequate hemostatic technique is essential to avoid prolonged surgical time.
Additionally, we determined the average cost for the complete surgical planning and 3D printed guides. This cost-effective solution has been described in some other studies with comparable results in terms of reducing operative time.17,21,22 However, they only propose it as a cost-effective solution, or only describe material costs, and do not describe the average cost for the complete procedure.
It has been reported that VP/3D printed guides done with an in-house design are significantly lower. L. Ritschl et al. calculated the median costs per case for in-house design and printing at EUR 14.30 (4.50-25.30). 17 In contrast, our study shows the average cost for the complete surgical planning and 3D printed guides was 914.44 ± 46.39USD. This represents an excellent cost-benefit ratio.
There are some limitations in our work: first, it was a retrospective study. Second, we included few participants in the control group because this surgery was performed seldom before utilizing the surgical guides. Moreover, we had limited access to the database because our institution deletes it every five years.
Another limitation could be that the residents in training used the guides with the potential overestimation of time reduction due to less experience.
We believe we have strengths in our study. On the one hand, we adjusted the analysis by age and comorbidities of the patients employing a linear regression, reducing possible bias, and demonstrating that the magnitude of the surgical guides/virtual planning effect remained significant and independent. On the other hand, we also emphasize we managed to apply advanced surgical planning effectively with a low budget and provided comprehensive steps of the process so other institutions can replicate our results. Furthermore, we carried out a qualitative assessment of the process using a Likert Scale in the form of a questionnaire evaluating the parameters of satisfaction and confidence when using the surgical guides. The latter is paramount since the benefit of the VP/SG goes beyond the operating room by adding confidence in the surgeon to perform better during the procedure and get aesthetic results. In conclusion, virtual planning and 3D printed surgical guides have the potential to reduce operation time in maxillofacial reconstruction. We believe that utilizing this technology for mandibular reconstruction improves the reconstruction quality and adds confidence to the surgeon and patient.
Footnotes
Acknowledgments
We would like to thank the assistance of Eduardo Hernandez Rangel, MD, Rafael Lopez Barron, Eng, Antonio Sanchez Uresti, MD, and Barbara Aimee Gonzalez Vazquez, MD in this research project. We certify that this work is original and has not been submitted to any other journal or presented in any conference meeting. The study was approved by the Ethics Committee and Research Committee of the Facultad de Medicina from the Universidad Autónoma de Nuevo León (UANL) and the Hospital Universitario "Dr José Eleuterio González” registration number (RA20-00006). A.N.G., A.A.N., G.E., M.M.G, W.J.R. disclosed no relevant relationships.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Author Contributions
Guarantors of the integrity of the entire study, A.N.G., A.A.N.; study concepts/study design or data acquisition or data analysis/interpretation, A.N.G., A.A.N., W.J.R., G.E., M.M.G; final approval of the manuscript, A.N.G., A.A.N., W.J.R., G.E., M.M.G; literature research, A.N.G., A.A.N., W.J.R., G.E., M.M.G; statistical analysis, A.N.G., A.A.N.; and manuscript editing, A.N.G., A.A.N., W.J.R.