
Abstract
Introduction:
Pelvic floor muscle (PFM) exercises are commonly prescribed to women with endometriosis-associated pelvic pain (EAPP) but the feasibility and effects of different PFM protocols remain unknown.
Objectives:
To evaluate the feasibility and acceptability of conducting a randomised controlled trial (RCT) comparing PFM contraction-plus-relaxation (PFMC + R) and PFM relaxation-only (PFMR) protocols combined with mindfulness in women with EAPP, and to explore changes in pelvic pain and PFM morphometry.
Methods:
An 8-week hybrid intervention of PFMC + R or PFMR with mindfulness was evaluated in a feasibility RCT. Primary outcomes were feasibility and acceptability; secondary outcomes were EAPP symptoms and PFM morphometry.
Results:
Of 95 participants assessed for eligibility, 45 were randomised to PFMC + R (n = 23) or PFMR (n = 22). The PFMC + R group had higher retention (86% vs 63%) and acceptability rates (82% vs 63%), and greater improvements in pelvic pain (mean difference (MD) = −2.80, 95% confidence interval (CI) −4.22, −1.45), dyspareunia (MD = −2.43, 95% CI: −3.90, −1.03), anorectal angle (MD = 3.61, 95% CI: 2.52, 9.48) and levator hiatus (MD = 0.34, 95% CI: 0.14, 0.63) at rest than the PFMR group.
Conclusion:
The PFMC + R protocol was more feasible and acceptable than the PFMR protocol and demonstrated greater improvements in EAPP symptoms and PFM morphometry. Larger studies are needed to verify these findings.
Trail Registration:
The Australian New Zealand Clinical Trials Registry, registration number: ACTRN12622001393741, trial registry URL).
Introduction
Endometriosis-associated pelvic pain (EAPP) is defined as persistent or recurrent pelvic pain in individuals diagnosed with endometriosis through laparoscopy. 1 Women with EAPP may report general pelvic pain, dysmenorrhoea, dyspareunia, dyschezia and dysuria. 2 Alterations in pelvic floor muscle (PFM) morphometry and increased PFM tone have been observed in women with endometriosis.3,4
PFM exercises are commonly prescribed by physiotherapists for women with EAPP to reduce pelvic pain and PFM tone.5,6 However, it is unknown which type of PFM protocol (i.e. PFM contraction-only, PFM relaxation-only (PFMR), or both PFM contraction-plus-relaxation (PFMC + R)) is more effective at reducing pelvic pain and PFM tone in women with EAPP. Due to the presence of pelvic pain, some authors recommend avoiding PFM contraction7–9 on the premise that PFM contraction may exacerbate local pain.10,11 Instead, PFMR (down-training) has been suggested for women with pelvic pain and increased PFM tone, emphasising avoidance of PFM contraction and a focus on relaxation.8,12,13 Although PFMR is commonly advised by clinicians, isolated PFMR has not been tested for clinical effectiveness to reduce PFM tone. There is also some evidence that performing PFMC + R might reduce PFM tone in participants with dyspareunia and pelvic pain.14,15 However, no study to date has compared the effects of different PFM protocols on pelvic pain intensity and PFM tone in women with EAPP. Studies which compare these PFM protocols are required to develop an effective management plan for women with EAPP.
There is growing evidence indicating that targeting the biopsychosocial aspects of pelvic pain requires multimodal approaches that include a physical component (e.g. PFM exercise) and a cognitive component (e.g. mindfulness).16,17 A recent randomised controlled trial (RCT) showed significant reductions in all EAPP symptoms in women with EAPP following a mindfulness intervention, compared to pharmacological and surgical treatments. 18 Therefore, adding mindfulness to PFM therapies could be feasible and beneficial in reducing EAPP symptoms. Attending face-to-face sessions has also been shown to be a potential barrier to successful participant recruitment. 19 Delivering physiotherapy sessions via digital communication technologies that is, telehealth represents an alternative option 20 but the feasibility and effectiveness of telehealth sessions in women with EAPP remains unknown. We therefore designed an intervention programme combining PFMC + R and PFMR with mindfulness using a hybrid mode of delivery (face-to-face and telehealth sessions). The primary aim was to investigate the feasibility and acceptability of this protocol in preparation for a full-scale RCT. The exploratory secondary aim was to examine changes in pelvic pain and PFM morphometry between the two groups at 8 weeks following the intervention. We hypothesised that the PFMC + R protocol with mindfulness, delivered in a hybrid format, would be a more feasible and acceptable intervention for improving pelvic pain symptoms and PFM tone in women with EAPP than the PFMR protocol.
Methods
Trial design
This feasibility RCT was reported according to the Consolidated Standards of Reporting Trials (CONSORT) Statement for reporting pilot and feasibility RCTs. 21 Ethics approval was obtained from Human Research Ethics Committee (ID: HREC/88754/MonH-2022-330436). This trial was registered with the Australian New Zealand Clinical Trials Registry prior to participant recruitment (registration number: ACTRN12622001393741).
Participants
Women were eligible to participate if they: (1) were aged 18–45 years, (2) had a confirmed diagnosis of endometriosis by laparoscopy or imaging, (3) were nulliparous or had not been pregnant beyond 12 weeks; (4) were pre-menopausal; (5) had a mean score ⩾ 4/10 on a self-reported numeric rating scale (NRS) for pelvic pain intensity (any of the following symptoms: general pelvic pain, dyspareunia, dyschezia or dysuria) at study entry; (6) had pelvic pain for a minimum of 3 months; (7) had access to internet and a laptop/mobile device with webcam; and (8) had sufficient English language skills to participate.
Women were excluded if they had received physiotherapy treatment for EAPP (more than two sessions within the previous 2 years), had a history of major gynaecological surgery (except if the surgery was for endometriosis), had neurological disorders, had active vaginal infection or intellectual/cognitive impairments.
Recruitment and consent
Patients were recruited from pelvic pain and gynaecology clinics in Melbourne, Australia and from study advertisements posted on social media. Potentially eligible patients from pelvic pain and gynaecology clinics were screened against the inclusion criteria, first by their clinicians and then by the research team. Participants recruited via social media were also screened by the research team and were required to provide medical documents from their physician confirming their endometriosis diagnosis. Eligible participants received a link to the participant information and consent form via Qualtrics software (Qualtrics, Provo, UT). Those who consented and completed the online questionnaire were enrolled in the study. Participating gynaecologists extracted data on endometriosis stage (using the revised American Society for Reproductive Medicine (rASRM) classification, 22 a staging system with four levels: minimal, mild, moderate and severe) and site of lesions (using the Enzian classification 22 ) from participants’ medical records, and provided imaging or surgical data where available. Participants recruited via social media were requested to provide details of staging, imaging or surgical findings from their physician.
Interventions
Participants underwent an 8-week intervention using a hybrid mode of delivery, combining face-to-face and telehealth sessions. All intervention sessions started with the same mindfulness component for both groups, using the ‘Insight Timer’ application, which provided a mindfulness programme for pelvic pain and endometriosis guided by physiotherapists. 23 This programme included deep breathing, body scan, stretching and progressive relaxation exercises. PFMC + R and PFMR components were reported according to the Modified Consensus on Exercise Reporting Template for Pelvic Floor Muscle Training (Table 1 and Appendix 1). 24
Pelvic floor muscle contraction-plus-relaxation and pelvic floor muscle relaxation-only components according to the Modified Consensus on Exercise Reporting Template for Pelvic Floor Muscle Training (CERT-PFMT).
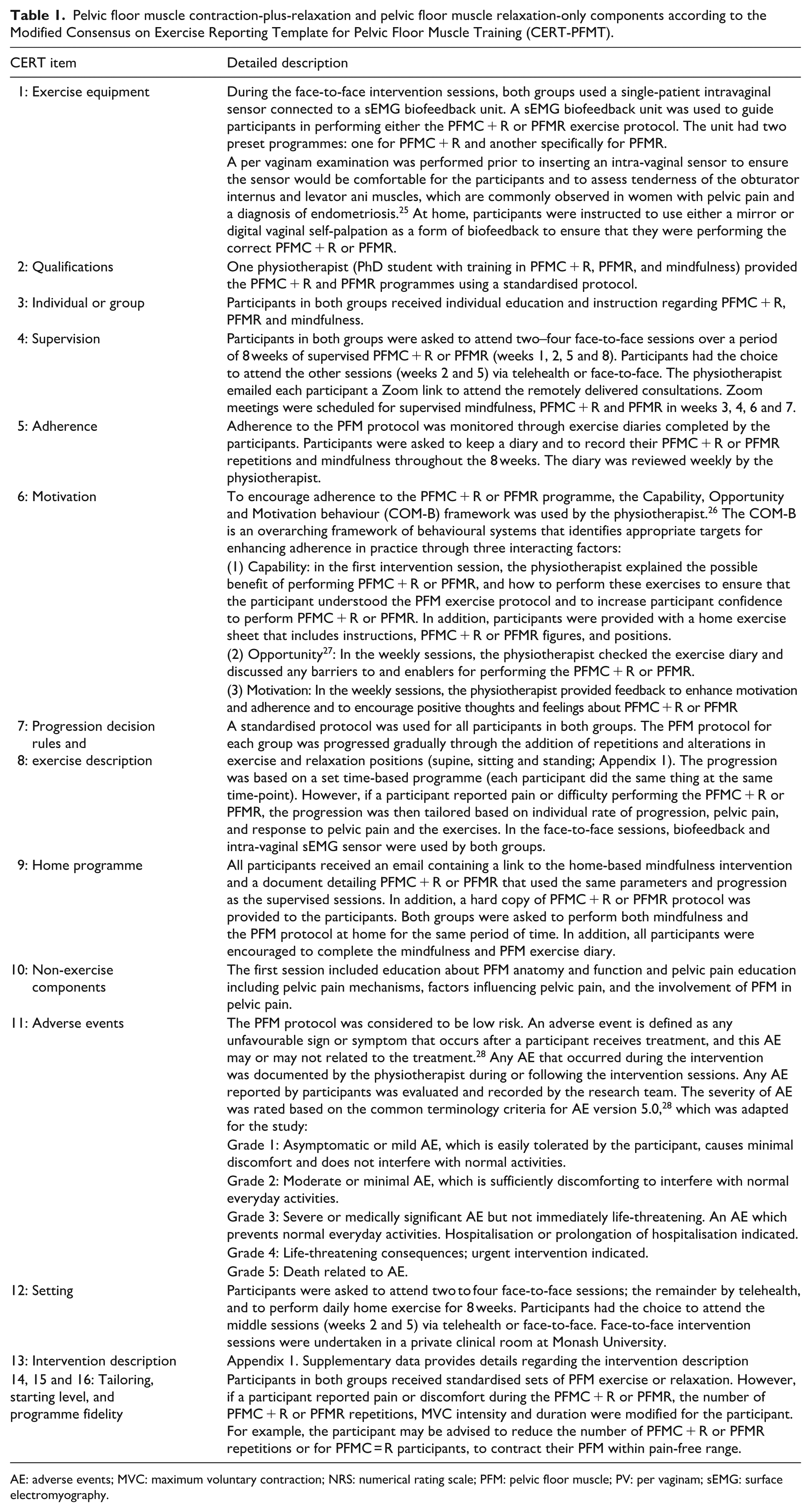
AE: adverse events; MVC: maximum voluntary contraction; NRS: numerical rating scale; PFM: pelvic floor muscle; PV: per vaginam; sEMG: surface electromyography.
Outcomes
Feasibility outcomes
Feasibility measures included retention (primary outcome), recruitment, dropout, attendance, adherence to PFM and mindfulness protocols (supervised sessions and at home), as well as adverse events (AEs), acceptability and satisfaction (Appendix 2). Details of AEs related to the interventions were reported to the physiotherapist either during or following the intervention sessions. Acceptability and satisfaction of the intervention were assessed following the final intervention session using a 5-point Likert scale ranging from ‘1 = completely acceptable/very satisfied’ to ‘5 = completely unacceptable/very dissatisfied’ (Appendix 2).
Outcomes of pelvic pain and related symptoms
Patient-reported pelvic pain was measured at baseline and after completion of the intervention (Appendix 3) and collected via the secure Qualtrics survey platform. Pain questionnaires, derived from the World Endometriosis Research Foundation Questionnaire–minimum endometriosis patient questionnaire (EPQ-M), captured general pelvic pain, as well as pelvic pain during periods, intercourse, bowel movement and urination. 29 Participants rated each symptom’s intensity on an 11-point NRS and selected the most bothersome symptom. The EPQ-M questionnaires also assessed pelvic pain frequency, interference and quality (the McGill Pain Questionnaire (SF-MPQ)). 29 Additional secondary outcomes were measured using the Pain Catastrophising Scale (PCS), 30 the Pain Anxiety Symptoms Scale (PASS), 31 and the Pain Self-Efficacy Questionnaire (PSEQ). 32
Pelvic floor muscle morphometry outcomes
Clinical outcomes were measured at baseline and immediately after the last intervention session. A blinded investigator used three- and four-dimensional transperineal ultrasound (3/4D TPUS) to measure PFM morphometry (anorectal angle (ARA), levator hiatus area (LHA), and anterior-posterior diameter of levator hiatus (LH-AP; Appendix 4)). 33 Imaging was performed after bladder emptying, with participants in a supine position, hips abducted and flexed to 60 ° and knees flexed.
PFM morphometry was assessed using a 4–9 MHz perineal ultrasound transducer (GE Healthcare) at rest and during maximum voluntary contraction (MVC). Three consecutive cineloops were recorded at rest and three during MVC. Image analyses were conducted by the same investigator offline.
Sample size
Sample size was calculated based on the primary feasibility outcome (retention rate) using data from a previous multimodal physiotherapy interventional study of 30 women with EAPP. 19 Assuming 86% of women completed 8-weeks of pelvic floor physiotherapy intervention and both baseline and post-intervention assessments, a 95% confidence interval (CI) and a margin of error of 0.1, the required sample size was 46 women in total. To account for potential dropouts (15%), 19 a total of 56 (28 per group) participants were required.
Randomisation
Randomisation occurred pre-intervention in a 1:1 ratio using random permuted blocks (sizes 4 and 6) from a computer-generated list. A research team member not involved in either participant recruitment or administration of outcome measures managed a concealed randomisation list and assigned participants into groups.
Statistical method
Descriptive statistics were reported for participant demographics, summary scores from pain questionnaires and feasibility data. Continuous data were visually assessed for normality. Differences in demographic characteristics (severity of endometriosis and presence of PFM tenderness) and baseline variables (pelvic pain intensity—general pelvic pain, dysmenorrhoea, dyspareunia, dyschezia, and dysuria—as well as PFM morphometry parameters) between the two groups were examined using Mann–Whitney U-test for continuous data and chi-square test for categorical data.
Post-intervention differences in continuous outcomes between groups were computed using one-way analysis of covariance (ANCOVA) with the baseline values (pelvic pain intensity and PFM morphometry parameters) included as covariates. Multiple linear regression analyses were also performed to examine changes in pain symptoms and PFM morphometry findings while adjusting for endometriosis severity. Endometriosis stage was collapsed to minimal-mild (stage I + stage II), and moderate-severe (stage III + stage IV). 22 Logistic regression models were used to examine the changes in categorical variables between the two groups, while controlling for baseline values (pelvic pain intensity and PFM morphometry parameters). All analyses were conducted using an intention-to-treat approach. Variables with missing data were imputed with mean score from each group. 34 Comparisons between pre-and post-intervention measures were made using paired t-tests. All analyses were tested with a significance level of p < 0.05 using SPSS 20.0 software (IBM Corp, Armonk, NY).
Results
Flow of participants through the study
As shown in Figure 1, 95 participants were assessed for eligibility, 45 expressed interest and were eligible for randomisation. Four women randomised to either the PFMC + R or the PFMR group withdrew before the first intervention session.
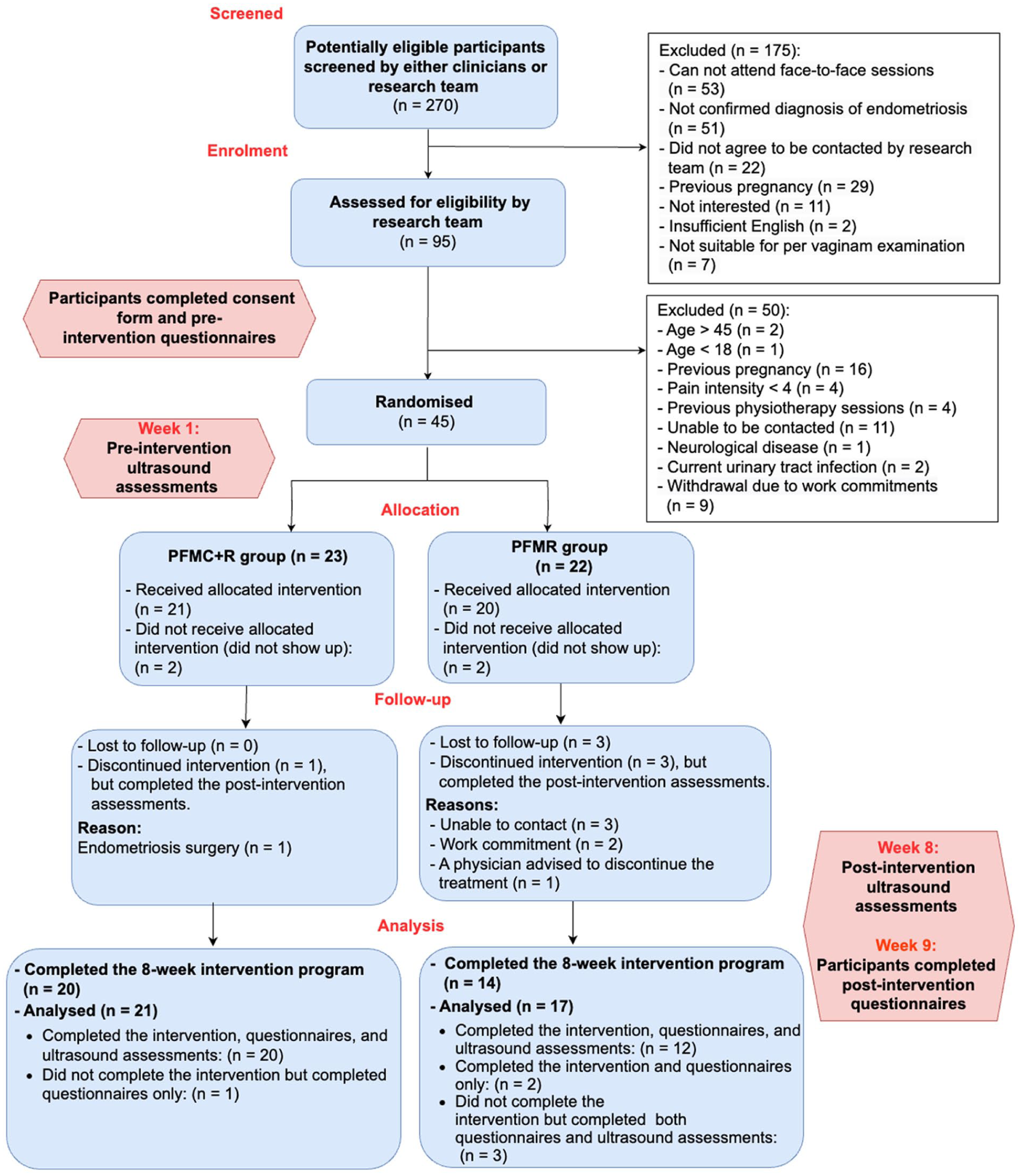
Flow of participants through the trial.
Participant chracteristics
Participant demographic and clinical characteristics are presented in Table 2. No significant differences were seen in most of the characteristics between the two groups at baseline. However, the PFMC + R group had a more severe stage of endometriosis (n = 13/23, 56% vs n = 2/22, 9%; p < 0.001) and recorded a higher prevalence of levator ani muscle tenderness (n = 20/23, 86% vs n = 6/22, 27%; p < 0.001) than the PFMR group.
Participant baseline demographic and clinical characteristics.
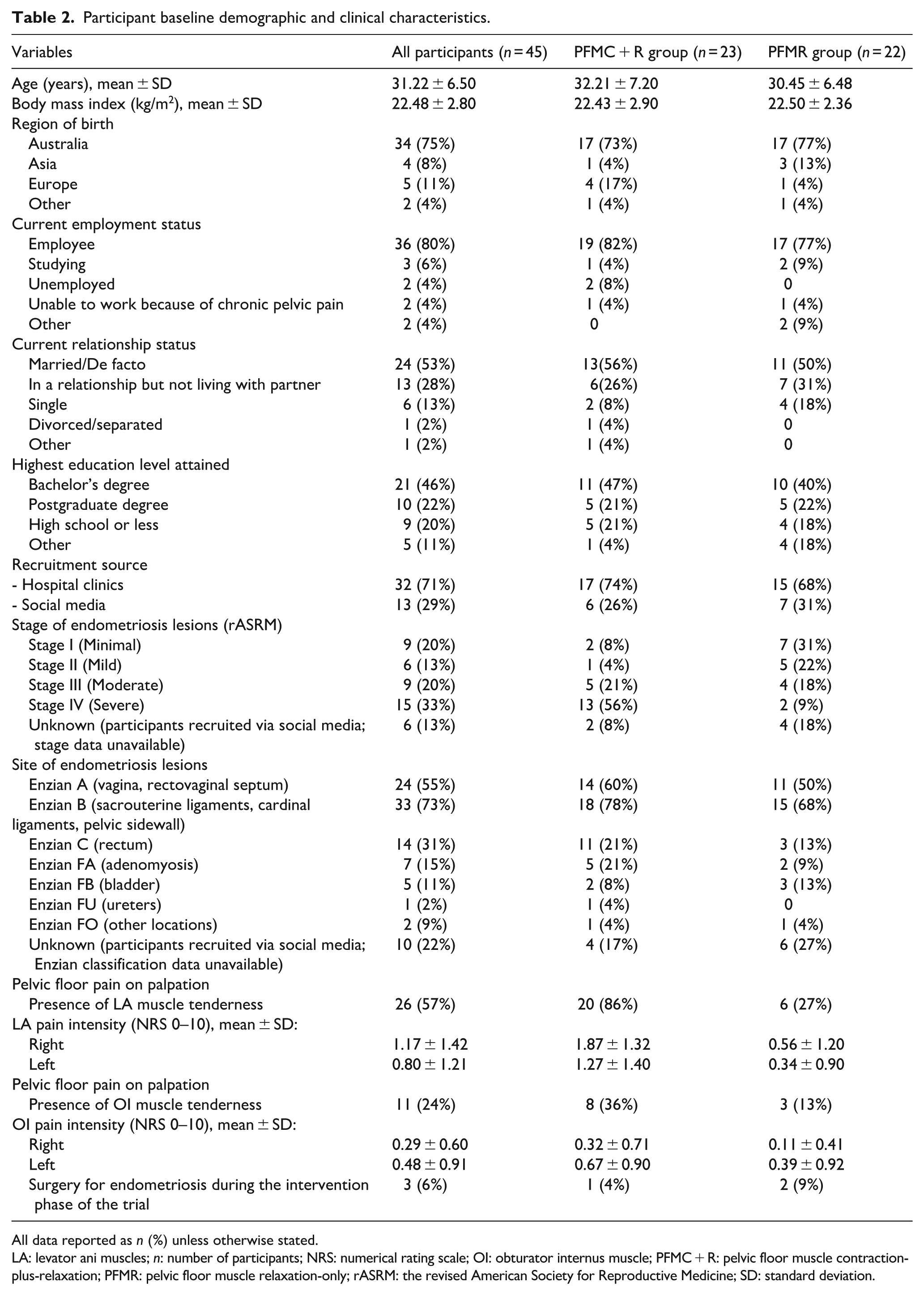
All data reported as n (%) unless otherwise stated.
LA: levator ani muscles; n: number of participants; NRS: numerical rating scale; OI: obturator internus muscle; PFMC + R: pelvic floor muscle contraction-plus-relaxation; PFMR: pelvic floor muscle relaxation-only; rASRM: the revised American Society for Reproductive Medicine; SD: standard deviation.
Study feasibility
The retention rate was higher in the PFMC + R group (n = 20/23, 86%) than the PFMR group (n = 14/22, 63%), as shown in Table 3 and Figure 1.
Feasibility and acceptability outcomes.
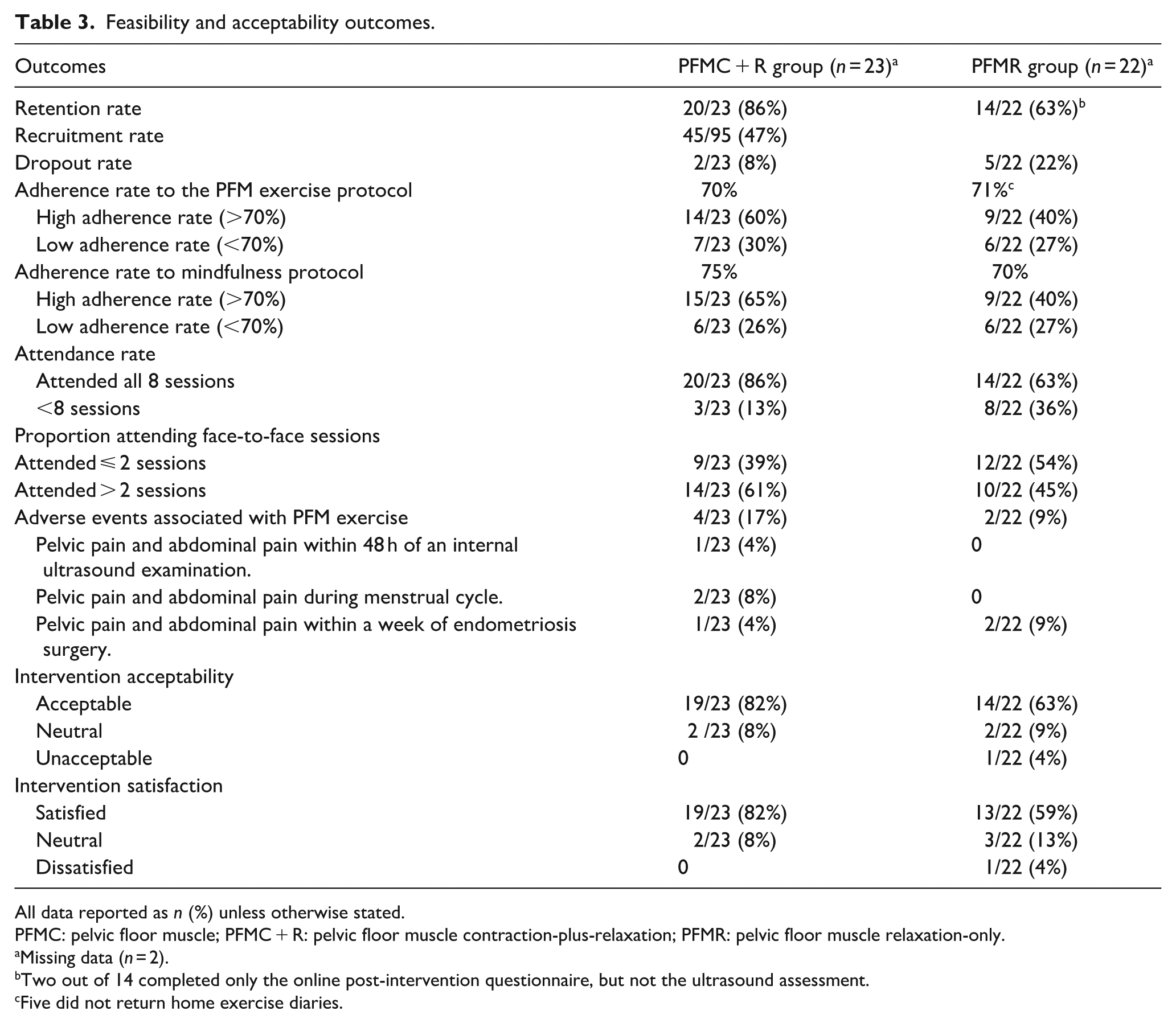
All data reported as n (%) unless otherwise stated.
PFMC: pelvic floor muscle; PFMC + R: pelvic floor muscle contraction-plus-relaxation; PFMR: pelvic floor muscle relaxation-only.
Missing data (n = 2).
Two out of 14 completed only the online post-intervention questionnaire, but not the ultrasound assessment.
Five did not return home exercise diaries.
Twenty-one participants in the PFMC + R group and 15 participants in the PFMR group returned the exercise diary. The mean adherence rate to the PFM protocol was 70% in the PFMC + R group and 71% in the PFMR group. The attendance rate for the intervention sessions over an 8-week period was higher (20/23, 86%) in the PFMC + R group than in the PFMR group (n = 14/22, 63%). During the 8-week intervention, mild and temporary AEs occurred in four participants in the PFMC + R group and in two participants in the PFMR group.
Acceptability and satisfaction of the intervention components
In the PFMC + R group, most participants (n = 19/23, 82%) rated the overall intervention as acceptable and were satisfied (Table 3). In the PFMR group, the majority of participants rated the overall intervention as acceptable (n = 14/22, 63%) and were satisfied with it (n = 13/22, 59%; Table 3). Additional acceptability outcomes for both groups are presented in Figure 2.
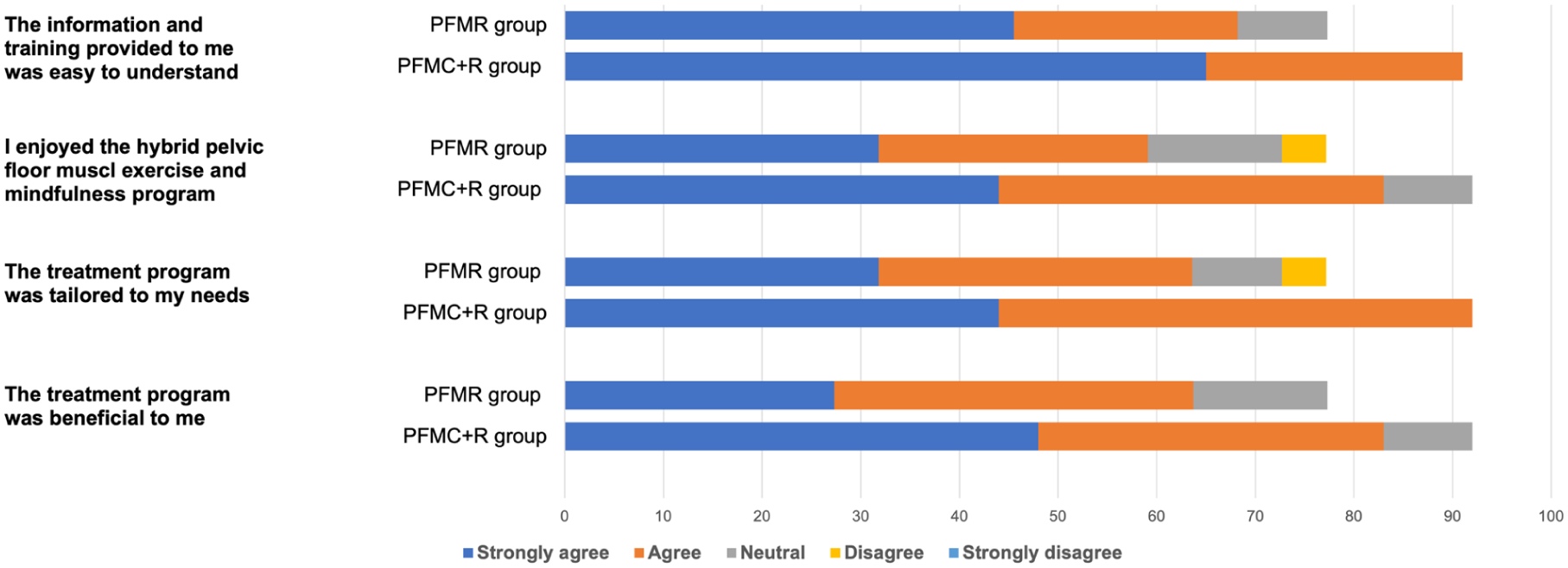
Acceptability outcomes for both PFM contraction-plus-relaxation and relaxation-only groups.
Outcomes of pelvic pain and related symptoms
The two groups were comparable at baseline on most patient and clinician-reported outcomes (Appendix 5). Table 4 presents the patient-reported outcomes of the two groups at baseline and post-intervention. After controlling for baseline pain values, the outcomes of the PFMC + R group revealed lower general pelvic pain intensity (p < 0.001) and dyspareunia (p < 0.001) than the PFMR group at post-intervention. These significant differences between the groups remained even after controlling for endometriosis stage.
Between-group differences in pain and pelvic floor muscle morphometry outcomes.
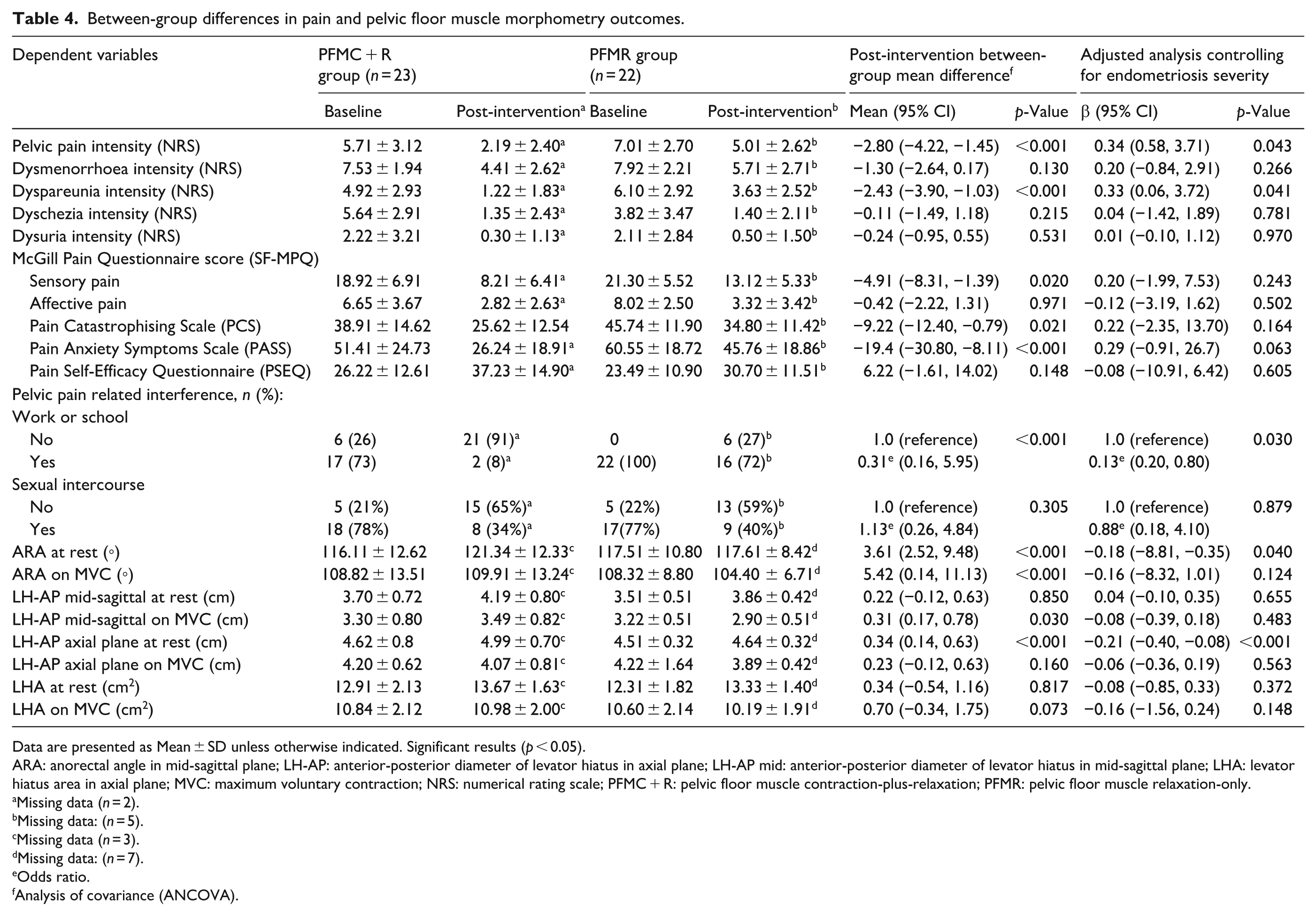
Data are presented as Mean ± SD unless otherwise indicated. Significant results (p < 0.05).
ARA: anorectal angle in mid-sagittal plane; LH-AP: anterior-posterior diameter of levator hiatus in axial plane; LH-AP mid: anterior-posterior diameter of levator hiatus in mid-sagittal plane; LHA: levator hiatus area in axial plane; MVC: maximum voluntary contraction; NRS: numerical rating scale; PFMC + R: pelvic floor muscle contraction-plus-relaxation; PFMR: pelvic floor muscle relaxation-only.
Missing data (n = 2).
Missing data: (n = 5).
Missing data (n = 3).
Missing data: (n = 7).
Odds ratio.
Analysis of covariance (ANCOVA).
The SF-MPQ (p = 0.020), PCS (p = 0.021), and PASS (p < 0.001) scores were lower in the PFMC + R group than in the PFMR group at post-intervention. However, these significant differences were not observed after controlling for endometriosis stage. The PFMC + R group was less likely (OR = 0.31, 95% CI: 0.16, 5.95) to experience pain-related interference with work/school than the PFMR group and this significant likelihood remained after controlling for endometriosis severity. Within-group analyses showed that both groups improved in all patient-reported outcomes immediately post-intervention (Appendix 6).
Pelvic floor muscle morphometry outcomes
The two groups were comparable at baseline on most PFM morphometry outcomes. After controlling for PFM morphometry variables at baseline, women undergoing PFMC + R protocol had larger resting ARA (p < 0.001) and LH-AP measurements obtained in the axial plane (p < 0.001) after the intervention compared with the PFMR group. These ARA and LH-AP findings suggest greater PFM relaxation in the PFMC + R than the PFMR group. These significant between-group differences remained even after controlling for the severity of endometriosis (Table 4).
During MVC, the PFMR group demonstrated smaller ARA (p < 0.001) and LH-AP measurements in the mid-sagittal plane (p = 0.030) post-intervention compared with the PFMC + R protocol group. This indicated greater PFM contraction in the PFMR group than in the PFMC + R group. However, no differences were observed in ARA and LH-AP measurements during MVC when we adjusted the analysis for endometriosis severity. Within-group analyses showed the PFMC + R group had statistically significant improvements in all PFM morphometry outcomes at rest, while the PFMR group demonstrated statistically significant improvement in AP (the mid-sagittal plane) and LHA measurements only (Appendix 7).
Discussion
This study has demonstrated that the PFMC + R protocol tested is a more feasible and acceptable intervention than the PFMR protocol for women with EAPP. Our feasibility hypothesis, requiring 86% completion of the 8-week intervention and assessments, was met in the PFMC + R group and is further supported by the low dropout rate and high acceptability and satisfaction, justifying progression to a fully powered RCT. However, only 45 participants were enrolled over 9 months due to recruitment challenges, including patient, trial, and recruitment-related barriers. Traditionally, feasibility studies often involve 20–50 participants per arm. 35 Therefore, a sample size of 45 participants (23 in the PFMC + R group and 22 in the PFMR group) was considered appropriate for assessing the feasibility and acceptability of the interventions, which were the primary aims of this study. Despite these challenges, the recruitment rate in this study was higher (45%) than the rate observed in a previous study (21%) 19 investigating the feasibility of physiotherapy to treat pelvic pain in Australian women with EAPP.
Evaluation of reported AEs indicated that the PFM protocols in this trial were low risk and temporary. Some participants in both groups reported pelvic pain and lower abdominal pain while performing PFM exercise within a week of an internal ultrasound examination, endometriosis surgery or during their menstrual cycles. One possible reason for experiencing pelvic pain whilst performing PFM contraction is viscero-somatic cross-sensitisation, as shared afferent and efferent pathways exist. 36 Nociceptive afferent stimuli from visceral structures may cross-sensitise PFM and vice versa 36 ; therefore, PFM contraction may stimulate the pelvic viscera and may lead to the perception of lower abdominal or pelvic pain. Pain during PFMR may result from increased attention to the pelvic area, potentially enhancing awareness of pelvic pain.
This is the first published feasibility RCT to investigate the impact of an individualised PFM exercise in women with EAPP. A recent RCT tested the effect of a general exercise programme which incorporated group-based PFM training and found an improvement in current pelvic pain. 37 Previous RCTs have shown that PFM exercise, as part of a multimodal physiotherapy intervention, significantly improved pelvic pain in women with other pelvic pain conditions such as provoked vestibulodynia and dyspareunia.38–40 If PFM exercise is effective in non-endometriosis pelvic pain, this supports the value of future testing in EAPP. Therefore, our results provide valuable insights for the design of future fully powered studies to test the effect of PFM exercise therapies on pelvic pain in women with EAPP.
Both PFM protocols appeared to reduce pelvic pain symptoms in women with EAPP, with the PFMC + R protocol showing greater improvement in general pelvic pain and dyspareunia intensity than the PFMR protocol. These findings are important as there is a lack of studies assessing PFMC + R and PFMR on pelvic pain in this population. 41 Our TPUS results also indicated significantly larger improvements in ARA and AP in the PFMC + R group than the PFMR group, indicating a greater reduction in resting PFM tone with the PFMC + R. However, these findings, including pain and PFM morphometry outcomes, should be interpreted with caution due to the relatively small sample size and because we were not powered to detect a difference in these outcomes. Future studies should investigate the long-term effects of PFMC + R on pelvic pain symptoms and PFM tone.
Despite randomisation, we observed more severe disease in the PFMC + R group than in the PFMR group. Participants with a severe stage of the disease were likely to have deep infiltrating endometriosis lesions and adhesions, which affected a number of pelvic sites, such as rectum, rectovaginal space and vagina. 42 Lesions and adhesions may affect PFM morphometry and the movement of PFMs during MVC, which may explain the absence of differences in PFM morphometry in the PFMC + R group. Another explanation for this might be fatigue related to the sequence of our post-intervention TPUS assessments, which were performed immediately (within 5 min) after the final intervention session. Therefore, PFM contraction ability may have been compromised due to muscle fatigue effects in our protocol. For more accurate results, future studies should consider scheduling the final intervention and the final TPUS assessment sessions with appropriate resting time between the two sessions.
The strengths of this study include: (1) comparison of two PFM protocols in an RCT study design; (2) blinding of the clinical assessor to group allocation; and (3) measuring PFM morphometry using TPUS, which is an objective and reliable method. 43 The main limitation was that we did not achieve our target sample size. The small sample size may limit the generalisability of our findings, and our findings related to pelvic pain symptoms and PFM morphometry could be spurious. Therefore, future studies with appropriate power are needed to improve the validity and generalisability of the results. The imbalance in endometriosis severity between groups was unexpected but addressed in our analysis. Future studies may consider stratifying participants by endometriosis severity, as outcomes may vary by endometriosis stage.
Conclusion
This study demonstrated that an intervention involving PFMC + R combined with mindfulness, delivered via a hybrid (face-to-face and telehealth) approach, may be more feasible and potentially beneficial in reducing general pelvic pain intensity, dyspareunia intensity and resting tone compared to PFMR. Further studies are needed to test this intervention in an appropriately powered study based on clinical outcomes.
Supplemental Material
sj-docx-1-pev-10.1177_22840265251406141 – Supplemental material for Pelvic floor muscle contraction-plus-relaxation versus relaxation-only with mindfulness for women with endometriosis-associated pelvic pain: A randomised controlled feasibility study
Supplemental material, sj-docx-1-pev-10.1177_22840265251406141 for Pelvic floor muscle contraction-plus-relaxation versus relaxation-only with mindfulness for women with endometriosis-associated pelvic pain: A randomised controlled feasibility study by Shaza Kadah, Sze-Ee Soh, Melanie Morin, Udari N Colombage, Jim Tsaltas, Nyasha Gwata, Bethany White and Helena C Frawley in Journal of Endometriosis and Pelvic Pain Disorders
Footnotes
Acknowledgements
The authors gratefully acknowledge the women who participated in this study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations and consent to participate
This study was approved by the Monash Health Human Research Ethics Committee on February 23rd 2023 (ID: HREC/88754/MonH-2022-330436). Written informed consent for inclusion in this research was obtained from all participants prior to their participation.
Consent for publication
Written informed consent was obtained from the patient(s) for their anonymised information to be published in this article
Data availability
Research data is available upon request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.