
Abstract
Clinical case
A 40-year-old with a history of stage IV endometriosis presented with right lower quadrant pain without bowel or bladder symptoms. She previously underwent four surgeries for treatment of endometriosis including total hysterectomy, unilateral salpingo-oophorectomy, excision of pelvic and abdominal wall endometriosis, rectosigmoid resection with reanastomosis, and ileal resection with reanastomosis. At the time of her most recent surgery, superficial bladder endometriosis was noted laparoscopically and excised. Cystoscopy was also performed at that time and was negative for intra-vesicular lesions. Postoperatively, the patient declined hormonal therapy. Following her most recent surgery, she noted improvement of her symptoms, however three years later, she developed recurrent cyclical right lower abdominal pain. Upon re-presentation, pelvic magnetic resonance imaging (MRI) was completed to evaluate for deep infiltrating endometriosis given her history of extensive disease. This revealed multiple areas concerning for deep infiltrating endometriosis including a T1 hyperintense focus involving the anterior bladder wall. Decision was made to perform repeat excision of endometriosis with temporary ureteral stent placement to aid in identification of the ureters in preparation for potential removal of bladder endometriosis.
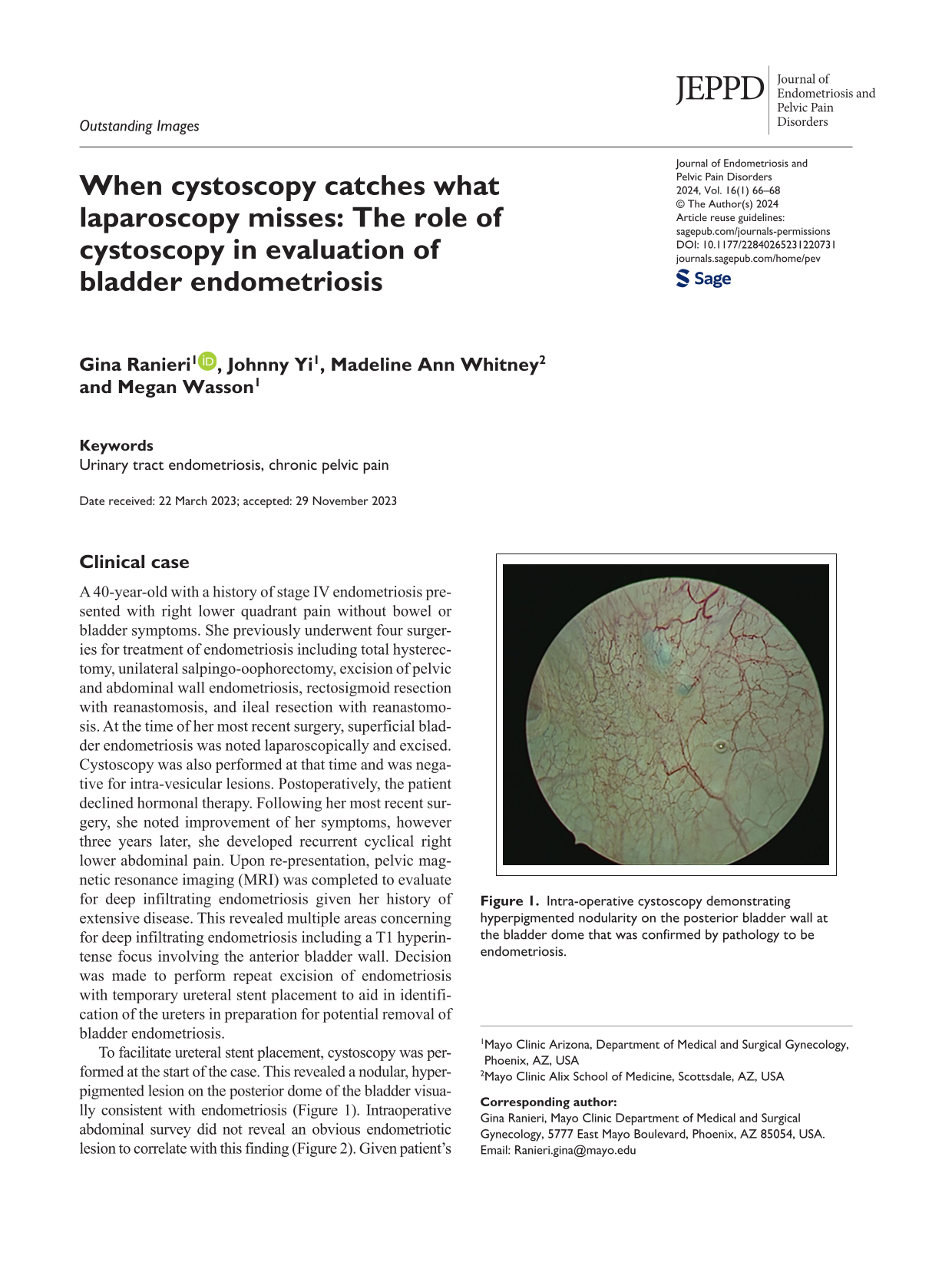
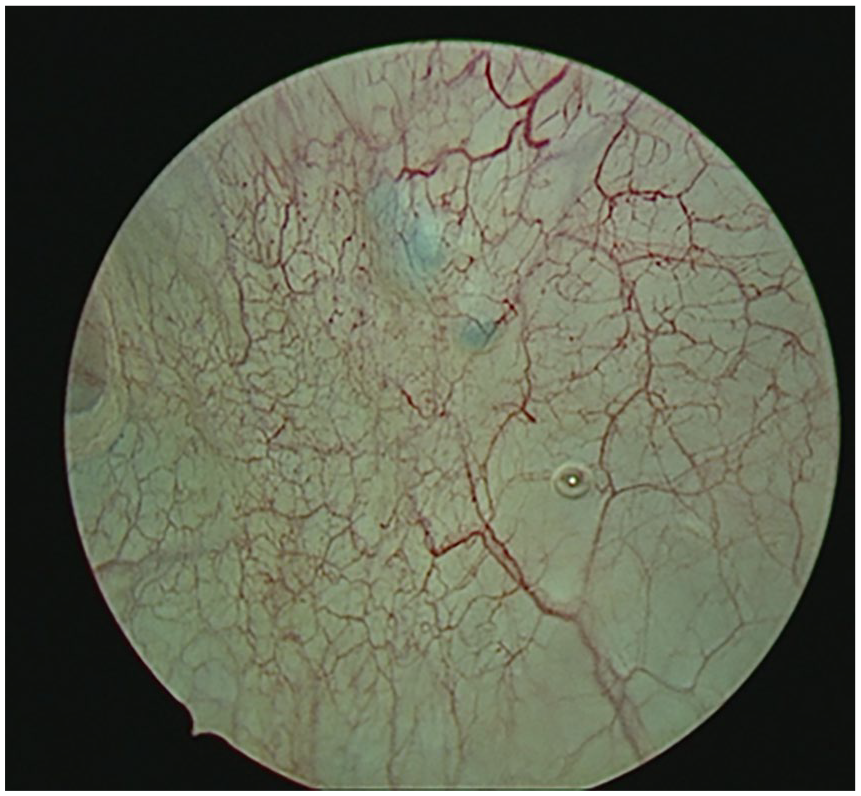
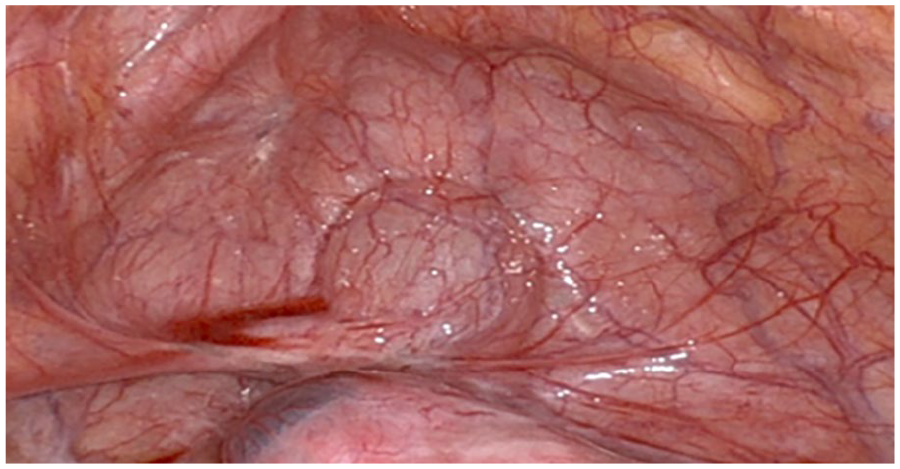
To facilitate ureteral stent placement, cystoscopy was performed at the start of the case. This revealed a nodular, hyperpigmented lesion on the posterior dome of the bladder visua-lly consistent with endometriosis (Figure 1). Intraoperative abdominal survey did not reveal an obvious endometriotic lesion to correlate with this finding (Figure 2). Given patient’s history of advanced stage endometriosis and recurrent symptoms, decision was made to remove the lesion to decrease risk of persistent endometriosis and endometriosis related pain. Intentional cystotomy was performed allowing intra-abdominal visualization of the bladder nodule and to aid in excision (Figure 3). The cystotomy was subsequently repaired with 3-0 delayed absorbable barbed suture in a two-layered running fashion. A double J ureteral stent was then placed in the left ureter to assist in maintenance of ureteral patency. Histopathology examination confirmed endometriosis.
Intra-operative cystoscopy demonstrating hyperpigmented nodularity on the posterior bladder wall at the bladder dome that was confirmed by pathology to be endometriosis.
Intra-operative laparoscopic view of the bladder was not suggestive of deeply infiltrating endometriosis of the bladder.
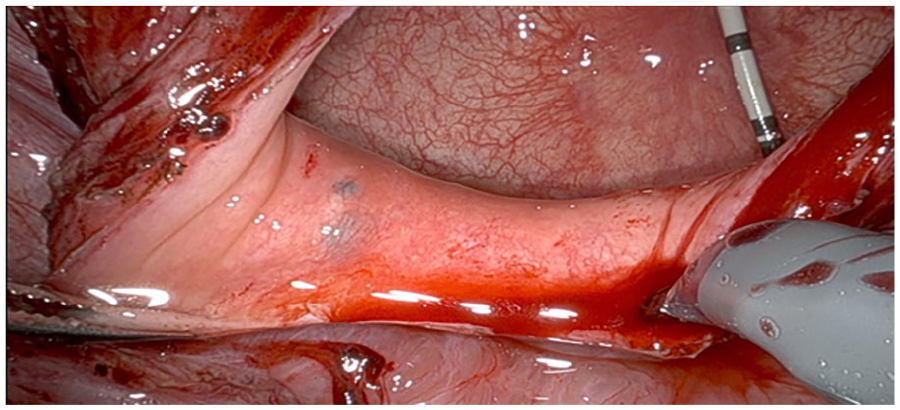
Intra-operative view of cystotomy and posterior bladder wall nodularity.
Discussion
The reported incidence of urinary tract endometriosis varies in the literature and is estimated to range from 0.3% to 12%. 1 The bladder is the most common site of urinary tract endometriosis with the dome and bladder base being the most frequent locations for lesions.2,3 Incidental detection of endometriosis involving the ureter occurs in 33% of cases and in 25% of cases with combined ureteral and bladder endometriosis. 3
Pre-operative imaging can be an essential step in facilitating operative planning and should be utilized to evaluate for genitourinary endometriosis in patients with chronic pelvic pain and urinary tract symptoms. When compared to MRI, ultrasound is associated with lower cost and similar accuracy for detection of endometriosis and is therefore recommended as the initial imaging modality.1,4,5 The sensitivity and specificity of ultrasound in detection of bladder endometriosis is 72% and 99%, respectively, while the sensitivity and specificity of MRI is 68% and 100%, respectively. 4
In this case, both MRI and laparoscopic survey failed to identify the intrinsic bladder disease. This highlights a limitation of laparoscopy in that extrinsic bladder lesions can be easily identified, but intrinsic disease is more easily missed. Typically, endometriosis lesions begin extrinsically, but intrinsic disease has been described.6,7 Therefore, cystoscopy to assess for bladder endometriosis is recommended when there is suspicion based on symptoms or imaging3,8 Performing cystoscopy during surgical evaluation of patients with chronic pelvic pain is a cost-effective method for detection of bladder endometriosis and can assist with delineation of endometriosis lesion margins.1,8 Cystoscopy should be performed for patients with symptoms or pre-operative imaging findings concerning for bladder endometriosis regardless of laparoscopic findings.
Footnotes
Authors contributions
GR was responsible for researching literature for this submission and for writing the first and final draft of this manuscript. JY contributed to writing of the manuscript and providing expertise. MAW was responsible for researching literature for this submission and contributing to writing of the manuscript. MW was responsible for the conception of this submission and writing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Ethical approval
The Mayo Clinic Institutional Review Board (IRB) acknowledges that based on the responses submitted for this new activity through the Mayo Clinic IRBe Human Subjects Research Wizard tool, and in accordance with the Code of Federal Regulations, 45 CFR 46.102, the above noted activity does not require IRB review.
Informed consent to participate
Written informed consent was not applicable to this submission.
Informed consent to publish
Written informed consent was not applicable to this submission.
Trial registration
N/A.