
Abstract
Background:
Chronic pelvic pain (CPP) is a common disorder in women that includes complex interactions between biological, psychological, and social factors. Accessibility to interprofessional, biopsychosocial CPP care remains a challenge for many patients. There is a lack of knowledge regarding the experiences of women using health services for CPP care and the impact of waiting for interprofessional CPP care. This study explores the perceptions and experiences of Canadian women with CPP interacting with the health system while waiting for interprofessional CPP care.
Methods:
Our qualitative study included women with CPP waiting for interprofessional care in Ontario, Canada. Data were obtained through semi-structured interviews which were transcribed verbatim and analyzed inductively using established methods for thematic analysis.
Results:
Ten women (median age of 38.5 years, age range 28–57) participated in in-depth semi-structured interviews. Three main themes were identified: (1) feeling adrift in the health system, (2) feeling “On hold,” uncertain, and in need of guidance, and (3) feeling reliant on a system that does not understand. Within these themes, women with CPP describe tangible strategies and recommendations for improving health system navigation and care.
Conclusion:
Our study highlights the need for improved access to interprofessional CPP programs, enhanced and targeted training for health professionals in CPP management, and better health system navigation support. Specific recommendations were provided from the perspectives of women with CPP and included providing information on what to expect and prepare for their appointment and engaging patients in education resources while they wait.
Introduction
Chronic pelvic pain (CPP) is a highly prevalent (5.7%−26.6% of women), 1 debilitating condition that disproportionately affects women.1–3 It accounts for substantial personal suffering and has a direct impact on individuals’ marital, social, and professional life.2,4 Given the multifactorial components that contribute to CPP, a review of clinical care guidelines recommend that therapeutic strategies should follow a biopsychosocial approach which includes an interprofessional clinical team and a multimodal treatment plan that address the biological, psychological, and social factors related to CPP. 3 While the biopsychosocial model of care for CPP can improve quality of life outcomes 5 and is endorsed by most clinical care guidelines, 3 the recommendations for implementation are often vague 6 and research and adoption of this model of care for CPP is sparse. Furthermore, wait times for interprofessional clinics (staffed with professionals from a minimum of three different disciplines 7 ) for chronic pain management can range from 6 months to 2.5 years.8,9 Long wait times can lead to a deterioration in patients’ health, functioning, and quality of life,10,11 and waiting for interprofessional care negatively impacts treatment outcomes once patients do receive treatment from an interprofessional pain clinic. 12
While previous studies have described the negative impact of waiting for chronic pain on health outcomes,8,10–12 very few studies have explored the perceptions of individuals waiting for interprofessional care. 13 Furthermore, little is known about the patient experience related to navigating and interacting with the health care system while they seek CPP care. Foundational work describing the experiences of women seeking care in New Zealand for chronic pelvic pain describe a medical interaction that “acts primarily to disempower the woman.” 14 The current experience of women with chronic pelvic pain interacting with the Canadian health system, a universal and publicly funded system, is also unknown. Understanding women’s past experiences with the healthcare system, and how they relate to current expectations is an important foundation for identifying opportunities for health system improvement. Therefore, we aimed to explore the experiences and perceptions of Canadian women with CPP navigating the health system while waiting for interprofessional care.
Methods
Study design
We employed a qualitative descriptive study design to gain a better understanding of the perceptions and experiences of women with CPP who were on the waitlist for an interprofessional pain clinic. Participants were enrolled in a larger study examining the feasibility of an online self-management program for women with CPP waiting for care at an interprofessional pain clinic. The project was approved by the Women’s College Hospital (WCH) Research Ethics Board [2020-0055-E]. Informed consent was obtained from each participant prior to their participation in this research study. The study is reported according to COREQ Guidelines. 15
Participants
Participants were eligible for the study if they: (1) were women who had any CPP that persisted for more than 3 months, (2) were fluent in English, (3) had internet access, (4) could provide consent, and (5) were referred to an interprofessional CPP clinic by their primary care provider and currently on the waitlist. Exclusion criteria included individuals who experienced severe cognitive impairments that would prevent them from participating in an interview. Considering the concept of information power as a guide for sample size, we expected to require 9–12 participants to address the depth of description required in our analysis given the density and specificity of the available information that could be provided our sample. 16 Consistent with recommendations of Braun and Clarke, 17 we have provided our conceptualization of saturation and description of the process of coding and theming provided in the analysis section to support our justification for the number of participants included.
Recruitment
Participants were selected based on a purposive sampling approach and all were recruited from an interprofessional tertiary referral center for CPP in Toronto, Ontario, Canada. Clinicians sent a letter of information about the study to participate based on demographic (sex, gender), and context (waiting for services) criteria. Potential participants in the study were contacted by phone by the research team, introduced to the researchers, screened for eligibility, and written consent (electronic) was obtained.
Data collection
Data were obtained through semi-structured interviews and a demographic survey was administered prior to each interview. Data was collected in June 2021. We developed a semi-structured interview guide to elicit data relating to our two study objectives. 18 Interviews occurred between the interviewer and participant over zoom, 19 and were conducted by a research coordinator EB with lived experience of pelvic pain (female, MHE candidate, with qualitative research training). All interviews were audio-recorded, transcribed verbatim, and verified for accuracy. Field notes were documented during each interview to capture verbal and non-verbal responses as well as interviewer impressions and observations.
Data analysis
Data were analyzed inductively using established methods for thematic analysis to capture themes describing the experiences of participants while on the waitlist for interprofessional CPP care. 20 NVivo software was used for data management and storage (Nvivo 12, QSR International Pty Ltd.). Researchers (RB, EB, RW, NM) independently reviewed three transcripts, identified key codes from each interview and together reached common understanding of the main codes and developed a master code list. Coding saturation was determined to be reached when new codes were not added from the narrative of successive interviews and sufficient context was established to describe the experiences of women with CPP. Once code saturation was reached in principle, the codes were applied to the remaining transcripts (EB, reviewed by RB) 21 for confirmation. Together, the research team developed categories that captured related aspects of the content, conducting a back-and-forth review of supporting elements of the narrative to ensure categories were representative of the codes each represented. Lastly, the research team identified themes consistent with groupings of categories. An example of related codes, categories, and theme is provided in Supplemental Table 2. The data from each transcript were again reviewed considering the categories and themes to ensure consistency, accurate representation of the data and rigor in our analysis. 18 Exemplars were selected that captured the essence of the data within each category.
Results
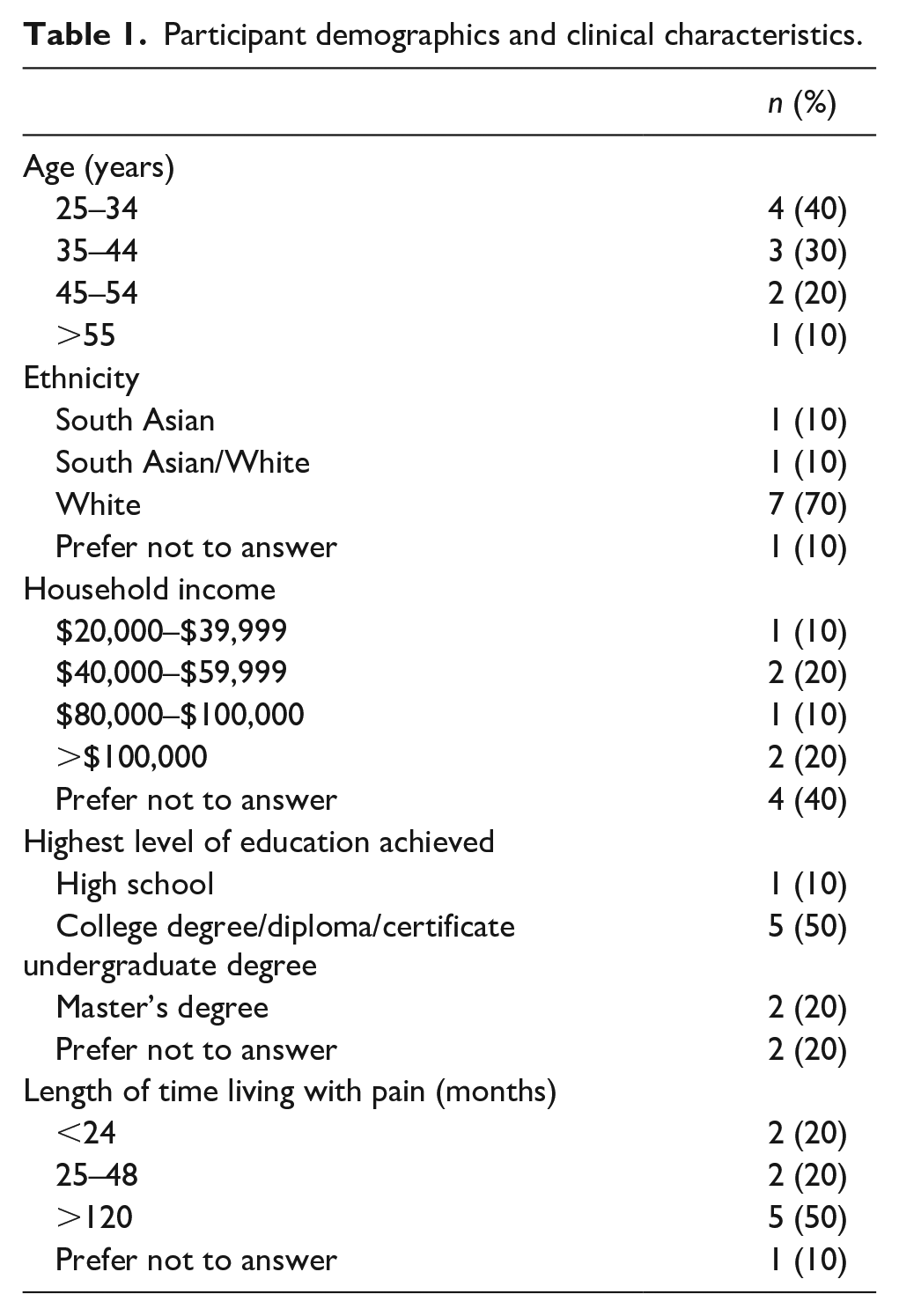
A total of 10 women with CPP, with a median age of 38.5 years and an age range of 28–57 (inclusive), participated in in-depth semi-structured interviews which were between 20 and 60 min in length. Participants had been waiting for interprofessional care for a median of 202 days (range 83–518 days). The average (SD) pain duration reported was 118 months (102 months). See Table 1 for detailed demographic information. One person declined participation in this study component due to time constraints and no participants dropped out of the interview.
Participant demographics and clinical characteristics.
Below we describe three identified themes relating to participants’ experiences and perceptions of navigating the Canadian health care system while on the waitlist for CPP care.
1. Feeling adrift in the health system
The theme, feeling adrift in the health system, was salient in the data; many participants emphasized the notion that the health care system is fractured resulting in participants having complicated relationships with treatments and the need for navigational support. Women with CPP described a long health care journey in which they were referred to multiple care providers at multiple clinics and had tried a plethora of treatments with limited success (Table 2, exemplar 1).
Additional exemplars highlighting each theme.
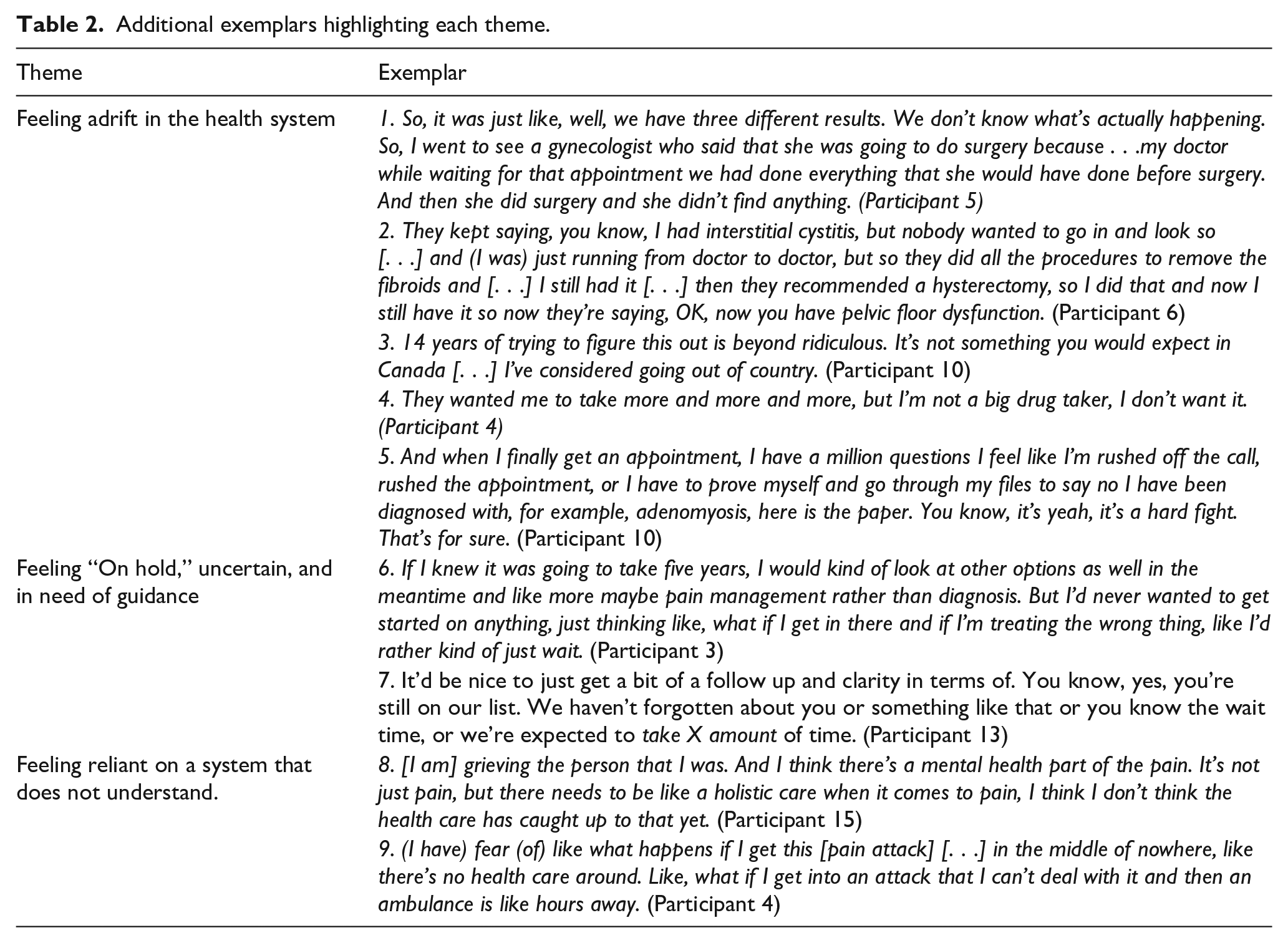
Participants acknowledged the complexity of CPP and related that after having “tried pretty much everything” (Participant 6), were left feeling that no one could determine an accurate diagnosis or appropriate treatment plan (Table 2, exemplar 2).
Participants also highlighted that there are a limited number of clinicians who focus on CPP and there are very few specialists in this area, stating that “it’s like you have to go see an endometriosis specialist which are few and far between across Canada” (Participant 10). Participants related how they had been referred to different specialty clinics only to be told by the specialist “no, this isn’t my specialty, but they can’t give me an answer on who I need to see” (Participant 3). They also expressed frustration and anger with the health care system in Canada and drew comparisons to other countries where they would have access to more specialists and could seek faster treatment (Table 2, exemplar 3).
Participants emphasized complicated relationships with treatment options, specifically around pain medication (Table 2, exemplar 4). While participants indicated that they are “always up for recommendations on what it might be because [they are] willing to go through anything at this point” (Participant 3), they also highlighted the need for multimodal therapeutic approaches stating that “pills, they’re good with giving you pills, like masking the problem, but [not] dealing with the issue” (Participant 7). Lastly, participants conveyed a desire for “a lot more research into it” (Participant 2) so that they could find answers.
Participants expressed challenges while navigating the health system. They indicated that “it would be great to have help with navigating all of that [the health system]. Emotionally it’s difficult to do it by yourself” (Participant 8). Participants spoke to the need to advocate for yourself and expressed that this could feel adversarial (Table 2, exemplar 5). However, they indicated that “the more education you have, the better you will be to advocate to the doctors for what you want and what you need for your own self” (Participant 9). They relayed that they required more information and education around their pain condition and treatment options.
2. Feeling “On hold,” uncertain, and in need of guidance
Participants expressed a lot of frustration around waiting for their appointment and described feeling “in the dark” once they had been referred to a specialist (Participant 3). They also shared concerns around waiting for a long period of time only to be denied care or sent for another referral to start waiting again. Several participants voiced the sentiment that it is a “waiting game . . .and, you know, in the meantime, life is on hold” (Participant 10). They indicated that the uncertainty around wait times left them unsure of whether they should seek alternative care options. They noted that their concerns around pursuing an inappropriate care path paralyzed them from moving forward in their pain care journey (Table 2, exemplar 6).
Several participants noted that an appointment with a pain care specialist was their “last resort” and that their primary care provider could not do anything else for them. Women described “feel[ing] like hopeless and helpless because there’s nothing that I can do in regards to the pain. I just have to sit and wait for the phone to call me or whatever” (Participant 5).
Participants also unanimously expressed uncertainty regarding expectations around their appointment with an interdisciplinary pain specialist clinic and the need for more support and clarity while on the waiting for care. Participants reported that they were unsure about the status of their appointment, how long the wait will be or even what to expect at that appointment. Many participants suggested that it would be helpful and even motivating to understand whether their referral was accepted, how long they can expect to wait for an appointment, and guidance around what they could or should do while they wait (Table 2, exemplar 7).
Participants also communicated that they had unclear expectations around their appointment. When asked about her expectations for her specialist appointment, participant 7 stated that she “(has) no idea (what to expect). I’ve learned a long time ago to not to try to run ahead and work everything out because the appointments don’t normally go how I envision or I’m just setting myself up for failure kind of thing like I’m more disappointed.” Participants indicated that being provided information such as, “this is what you should expect for your appointment” (Participant 6), and how to prepare for it would be helpful.
3. Feeling reliant on a system that does not understand
The emotional toll that participants expressed from requiring care from a health system that does not understand CPP or their needs as an individual was palpable. Participants expressed feelings of being misunderstood in the health care system. Participant 15 noted that “I really think that doctors really don’t understand pain, and I mean, even for me, as a [health care provider], I learned about pain (in) school, but learning about pain and experiencing pain like this is completely different. It’s not just pain. You have pain, but then you have fatigue. Then you have insomnia. Then you have a depression.” Some described feeling that health care providers are not listening to or understanding their needs. Participant 7 shared that “it’s been very frustrating when I bounced from doctor to doctor to doctor trying to find answers and I feel like nobody’s kind of listening to me.” Participants indicated that being passed from doctor to doctor left them feeling dismissed and alone. Participants also spoke about the emotional toll of attempting to access CPP care, specifically about the fear and anxiety they experience being uncertain about whether they would receive care and if the care plan would help them holistically manage their pain. They also describe the emotional toll associated with their mental health (Table 2, exemplar 8).
Lastly, participants also described feeling tethered to the health care system, relaying fears about having a pain attack away from health care services and noted how this impacted their ability to live their life the way that they want to (Table 2, exemplar 9).
Discussion
Our study captures the experiences of women on the waitlist for interprofessional CPP specialist care in Canada. Our findings detail health care journeys that are fragmented and challenging to navigate and reveal the frustrations women expressed around wait times that were considered too long. Women also highlight the need for enhanced access to CPP-specific interprofessional care and greater transparency during the navigational process such that there is less uncertainty around their care.
One of the most salient reports identified across participants was the sense that they felt “adrift in the health system” relating to their experience of being sent to multiple care providers and trying many treatments, often without achieving a clear diagnosis and/or little therapeutic success. Many participants expressed frustrations around the lack of access to specialists who had expertise in CPP. Our findings echo the sentiment raised by the World Health Organization which referred to CPP as “a neglected reproductive health morbidity.” 2 There is a dearth of research in physiopathology and treatment 1 and a lack of a standardized definition or diagnostic criteria which makes it challenging for clinicians to identify and treat CPP. Clinicians trained in obstetrics-gynecology have expressed that a lack expertise led to them feeling overwhelmed and inadequately trained to address the needs of women with CPP.22,23 Participants in our study called for tailored training for clinicians around CPP management, as well as research and innovation to improve diagnostic and biopsychosocial treatment options.
A common sentiment across our participant group was the feeling that the wait time for interprofessional CPP care was too long. It is well documented that waiting for care leads to deteriorations in health, including mental health, and has a negative impact on quality of life for individuals with chronic pain.8,10 The length of waiting for care has also been associated with poor response to treatment in individuals with rheumatic conditions. 12 Consistent with previous reports from individuals waiting for arthroplastic surgery, 24 our participants also indicated that they felt “on hold” with their lives and pain management while waiting for care. This related to hesitancy in trying any other management strategies or treatment options while on the waitlist out of concerns for “trying the wrong thing.” They felt that it was a “waiting game” and that they were “in the dark” until their appointment. This resulted in uncertainty around expectations, anxiety, and frustration. Deslauriers et al., 13 also report that participants with chronic pain criticized the lack of information given to them about their appointment. Participants recognized the need to self-navigate but expressed concerns around their level of knowledge and preparedness to assume a self-directed care role. They identified the opportunities for health system improvement so that patients can gain autonomy and make informed choices around their health management including (1) enhanced communication around how long the wait would be, (2) clarity around appointment expectations and a detailed description regarding what they can expect and how they can prepare, (3) resources and CPP self-management information and support while they wait for care.
Finally, participants also expressed the feeling that they were reliant on a system that does not understand them. These findings are consistent with previous reports from patients which have identified physicians’ time, knowledge, and interest in CPP as key barriers to receiving adequate care. 25 Despite the recommendations for a biopsychosocial approach to CPP management delivered by an interprofessional team, unimodal or organ system focused silos in care remain standard. These siloed approaches to CPP care can result in patients being bounced around the health system without a coordinated care plan. 26 Women with CPP are often given several diagnoses, have their pain and suffering minimized by the system, and are left to feel disempowered, unheard, and disengaged from their care. 27
One of the main strengths of this study is the methodological approach, which involved conducting in-depth and semi-structured interviews that enabled us to explore complicated experiences and perceptions in a nuanced way that added to the richness of the data. 16 Limitations of the study included our narrow sample, specifically that it was limited to women who were already waiting for interprofessional CPP specialist services and therefore may not capture the breadth of experiences of women navigating the health system seeking CPP-related care. Another limitation was that, while all participants were diagnosed with CPP, we were unable to determine specific types of CPP as, due to the complex nature of CPP, many patients do not have specific diagnoses and are on the waitlist for interprofessional specialist CPP care to determine or confirm diagnoses. Furthermore, participants also differed in terms of how long they have lived with CPP which may impact their feelings and attitudes toward waiting for care. Finally, our data were collected in the context of waiting for care within a publicly funded health system and may not generalize to other health systems.
Conclusions
The findings from our study have important clinical, health system, and educational implications for the management of CPP. Firstly, we have identified areas to target for health system improvement including providing patients with navigation support and information around their appointment such as the current wait times and information about what they can expect, what is expected of them and how they can best prepare for their appointment. This could also include engaging patients in education and self-management resources while they wait. Secondly, our results point to a need for increased attention to training and education in CPP for healthcare professionals. While previous work has drawn attention to the lack of formal training in CPP management and the uncertainty and discomfort some practitioners express around diagnosis and management of CPP,22,28 our study highlights the downstream impact that this has on patients. A dearth of trained clinicians equipped to support patients with CPP contributes substantially to the long wait times. These long wait times further exacerbate the challenges around diagnosis and identifying the primary pain generator in the pelvis. 29 Finally, the results of our study emphasize the need for improved access to interprofessional, biopsychosocial approaches to CPP management. Despite numerous clinical guidelines and consensus statements recommending the early integration of interprofessional care models,3,28,30 participants faced significant barriers accessing interprofessional care. Greater investments in integrated funding models designed to promote interprofessional care are required to bridge the gap in women’s health and address this neglected reproductive and sexual health morbidity. 2
Supplemental Material
sj-pdf-1-pev-10.1177_22840265221148786 – Supplemental material for Fractured system, fractured care: The experiences of Canadian women with chronic pelvic pain waiting for interprofessional pain care
Supplemental material, sj-pdf-1-pev-10.1177_22840265221148786 for Fractured system, fractured care: The experiences of Canadian women with chronic pelvic pain waiting for interprofessional pain care by Rachael Bosma, Emeralda Burke, Nida Mustafa, Tania Di Renna and Rosemary Wilson in Journal of Endometriosis and Pelvic Pain Disorders
Supplemental Material
sj-pdf-2-pev-10.1177_22840265221148786 – Supplemental material for Fractured system, fractured care: The experiences of Canadian women with chronic pelvic pain waiting for interprofessional pain care
Supplemental material, sj-pdf-2-pev-10.1177_22840265221148786 for Fractured system, fractured care: The experiences of Canadian women with chronic pelvic pain waiting for interprofessional pain care by Rachael Bosma, Emeralda Burke, Nida Mustafa, Tania Di Renna and Rosemary Wilson in Journal of Endometriosis and Pelvic Pain Disorders
Supplemental Material
sj-pdf-3-pev-10.1177_22840265221148786 – Supplemental material for Fractured system, fractured care: The experiences of Canadian women with chronic pelvic pain waiting for interprofessional pain care
Supplemental material, sj-pdf-3-pev-10.1177_22840265221148786 for Fractured system, fractured care: The experiences of Canadian women with chronic pelvic pain waiting for interprofessional pain care by Rachael Bosma, Emeralda Burke, Nida Mustafa, Tania Di Renna and Rosemary Wilson in Journal of Endometriosis and Pelvic Pain Disorders
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Ontario Medical Association Innovation Fund.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.