
Abstract
Introduction:
The aim of this study was to compare the subjective theories of illness in patients with fibroids and patients with endometriosis, and to identify potential factors influencing them.
Methodology:
Participating patients were recruited via three specialized centers for fibroids and endometriosis. To assess their subjective theories concerning the cause of their illness, we used a questionnaire based on the revised Illness Perceptions Questionnaire (IPQ-R). We also gathered and evaluated data relating to sociodemographic factors and psychological distress or possible anxieties using the Kessler Psychological Distress Scale (K10) and the Generalised Anxiety Disorder Assessment (GAD-7).
Results:
We were able to analyze data from 201 patients with fibroids and 212 patients with endometriosis. About 94.4% of the patients had one or more subjective theories concerning the cause of their illness. Both groups perceived “stress or worry” to be the most probable cause of their illness. Compared to endometriosis patients, patients with fibroids were more likely to assume “aging” and “heredity” as the cause of their illness. Endometriosis patients, on the other hand, were more likely to choose theories pertaining to the “environmental influences and immune system” category. The patients’ age, formal education, and conspicuous score values in the K10 or GAD-7 questionnaire proved to be important factors influencing their beliefs about the cause of illness.
Conclusion:
Patients perceive stress and psychological strain as possible causes for their illness. It might be beneficial to take this information into account in conversations between doctors and patients and when drawing up psychosomatic-gynecological treatment plans.
Keywords
Introduction
According to Leventhal’s “Common-Sense-Model of Illness Representation,” subjective illness theories comprise all personal considerations regarding the identity, cause, consequences, timeline, and controllability of an illness.1,2 It is believed that most patients form a unique subjective theory of illness during the course of their disease. 3 These theories are dynamic concepts and adapt to changes in the patients’ lives and are influenced by personal, sociodemographic as well as illness-specific factors.4–8 Normally, these theories are not discussed during medical consultations, but during the last decades researchers were able to show that they can have a considerable impact on the health behavior of patients, both positive and negative, especially regarding adherence to therapy.4,9,10
Previous research on subjective theories of illness in gynecology has mainly focused on malignant diseases. 11 Very few studies are available internationally on subjective theories of illness in patients with fibroids or endometriosis, even though, fibroids and endometriosis are the most common benign chronic proliferative illness in gynecology.12–16 Moreover, Symptoms related to fibroids and endometriosis can have a significant impact on the quality of life of the women affected.17–20
Consequently, the objective of our own cross-sectional study was to answer two main questions: What kinds of subjective theories of illness do patients with fibroids and patients with endometriosis have? And which sociodemographic factors influence these theories?
Methodology
Study population
From June to December 2017, all first-time patients who visited one of two outpatient clinics specialized in fibroids and endometriosis at Charité-Universitätsmedizin Berlin (M.D. and S.M.) or one selected gynecological practice specialized in endometriosis (A.D.E.) in Berlin were invited to participate in the study. The inclusion criteria were: at least 18 years of age, sonographically detected fibroids or clinically and symptomatically confirmed endometriosis and sufficient knowledge of German or English to answer the questionnaire. Since medical consultations might influence the patients believes about an illness, we only included patients at their first consultation of a specialized doctor in fibroids and endometriosis. 6 To differentiate between subjective theories of illness in patients with fibroids and endometriosis, women affected by both fibroids and endometriosis were excluded from this study. The number of cases necessary for the study was estimated based on the occurrence of genetic predisposition as suspected cause of illness in patients with fibroids in the study of David et al. 14 since genetic predisposition is a known risk factor for both fibroids and endometriosis that has been verified in literature.21,22 67.3% of patients in the cohort of David et al. 14 believed a genetic predisposition was the cause of their fibroids. Our hypothesis was that this figure would be lower in patients with endometriosis and therefore allowed for 15% lower prevalence in this group. It was thus estimated that we would need to interview at least 182 women in each the endometriosis and the fibroids group, with a power of 80%. Taking into account an expected drop-out rate of 10%, we determined a final number of 200 patients to be interviewed per group.
Questionnaire set
A German language questionnaire consisting of 69 items was employed to survey the subjective theories of illness. The “cause” section of the revised Illness Perception Questionnaire (IPQ-R) provided the basis for the questionnaire, to which we added the items “fate” and “influence of (a) god,” following Barnes et al. 23 and Moss-Morris et al. 24 The patients were asked to assess each item of the IPQ-R relating to possible causes of their illness using a five-point Likert scale (“strongly disagree” to “strongly agree”). The isolated use of only one section of the IPQ-R was endorsed by its originator.
We also recorded numerous factors which are believed to potentially influence the subjective theories of illness, such as various sociodemographic factors, the type of disorder as well as the self-assessed level of knowledge about the illness.5,6 In addition, we recorded whether patients had an unfulfilled desire to have children in order to investigate possible effects on the subjective theories of illness. The Kessler Psychological Distress Scale questionnaire (K10) and the Generalized Anxiety Disorder 7 questionnaire (GAD-7) were used to identify possible anxiety disorders and other forms of psychological distress that might have an impact on the theories of illness.25,26
Statistics
We relied on IBM SPSS Statistics version 25 for the statistical evaluation of the questionnaires. We performed an exploratory analysis of the data, determining statistical parameters such as median and interquartile range as well as absolute and relative prevalence. In order to assess the level of agreement for each of the IPQ-R items, we performed a dichotomization: The answers “agree” and “strongly agree” were classified as agreement, the answers “neither agree nor disagree,” “disagree,” and “strongly disagree” were not classified as agreement. For the comparison of the fibroid patients and the endometriosis patients as well as for the comparison of two groups, we used the Mann-Whitney U test for continuous data, Kendall’s tau-b coefficient for ordinal data and Fisher’s exact test for dichotomous data. The statistical significance was set at p < 0.05.
We performed the factor analysis for both groups together and limited the number of factors to four. We then established four scales, which were subjected to reliability analysis for internal consistency. In order to compare the scales and the single items for fibroid and endometriosis patients, we performed a multivariate analysis comprising several confounding variables (age, migration background, formal education, and self-assessed level of knowledge about the illness). Linear regressions were used to calculate the continuous variables (scales). The ordinal single items were dichotomized (see above) and analyzed using logistic regressions.
Ethics and data protection
The study was approved by the ethics committee of the Charité-Universitätsmedizin Berlin (application number: EA4/088/17). The requirements of the Charité for good scientific practice and the Berlin Data Protection Act were both adhered to.
Results
In total, 225 patients with fibroids and 242 patients with endometriosis were invited to participate in the study, 201 fibroid and 212 endometriosis patients completed the questionnaire set (see Figure 1). Drop-out rates were similar at 10.7% for fibroid patients and 12.4% for endometriosis patients (p = 0.567). For a summary of all sociodemographic data, see Table 1.
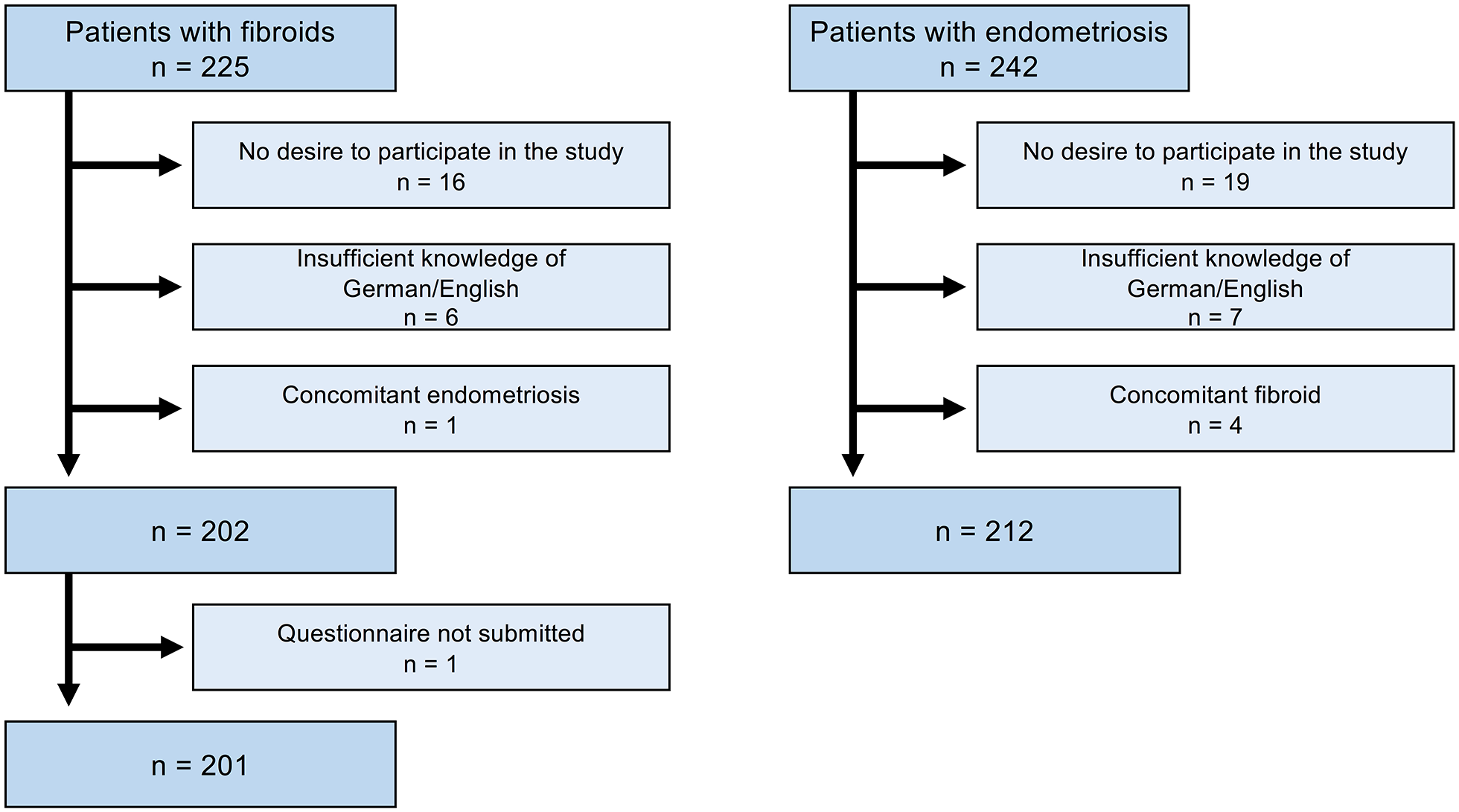
Drop-out rate among patients with fibroids and patients with endometriosis.
Sociodemographic characteristics of patients with fibroids and patients with endometriosis.
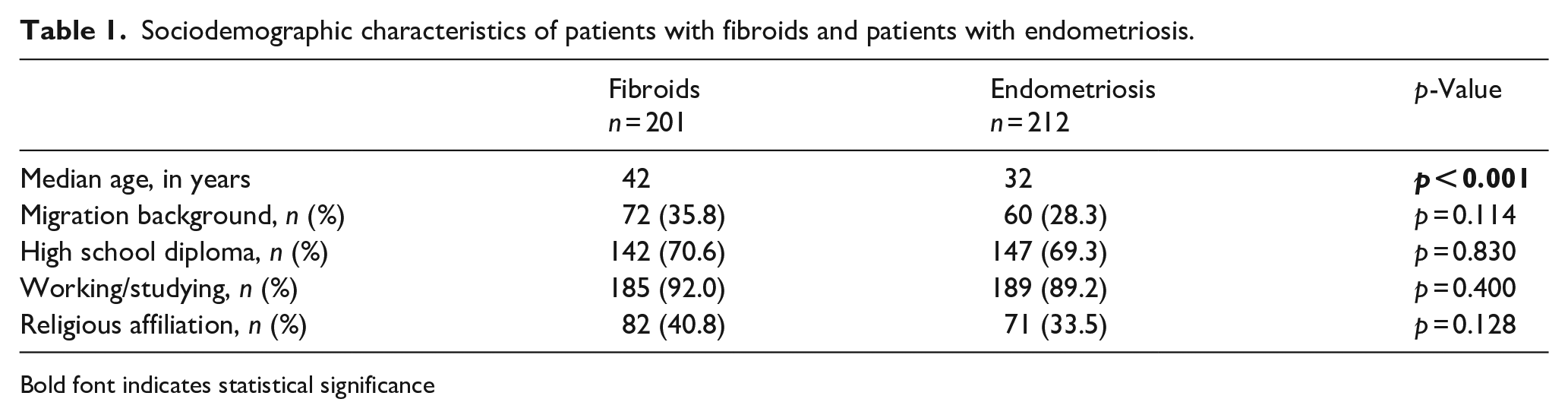
Bold font indicates statistical significance
Causal beliefs of patients with fibroids and endometriosis
About 60.2% of the participants reported having thought about the cause of their illness. Endometriosis patients were less likely to talk about these thoughts with their gynecologist than patients with fibroids (26% vs 39%) (p = 0.039). One in six endometriosis patients, as well as nearly one in eleven fibroid patients indicated that they were uncomfortable expressing their personal thoughts on the cause of illness to their physician (p = 0.127).
About 94.4% of the patients chose at least one of the 20 items of the IPQ-R as a possible cause of their illness. The three most common subjective theories of illness in patients with fibroids were “stress or worry” (58.2%), “aging” (54%), and “hereditary” (46.2%); in endometriosis patients, these were “stress and worry” (64.8%), “chance or bad luck” (51.2%), and “altered immunity” (45.8%) (see Figure 2).
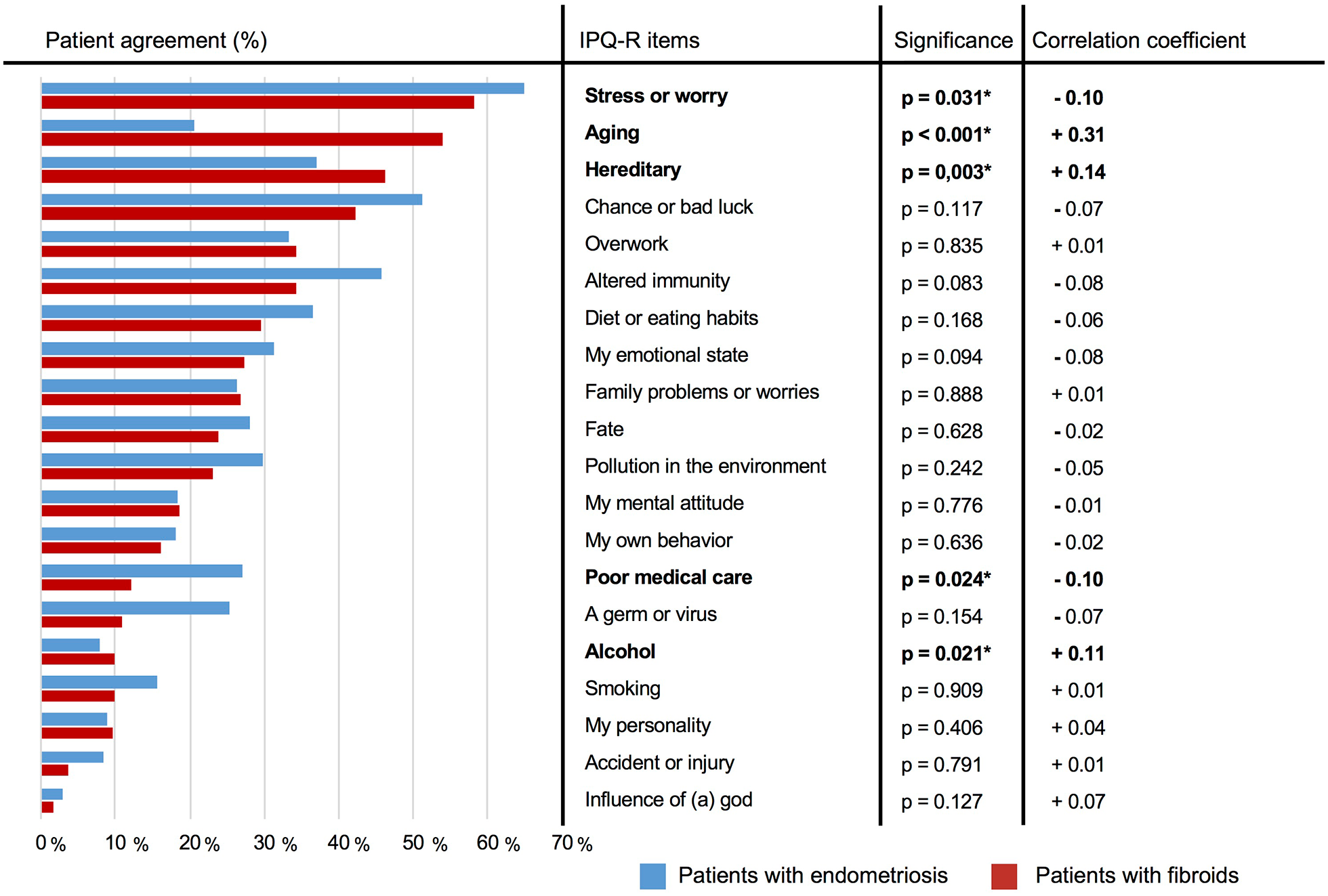
Patient agreement with the IPQ-R items.
Results of the factor analysis of the IPQ-R items
For the total population of patients, we were able to identify four factors that explained 54% of the variance within the data (see Table 2). “Hereditary” was the only item not clearly assignable to any of the categories. The four categories included: “psychological reasons,” “risk behavior and age,” “environmental influences and immune system,” as well as “force majeure.” The internal consistency of the categories “psychological reasons” and “environmental influences and immune system” was satisfactory (see Table 2). The internal consistency of the “risk behavior and age” category was enhanced by excluding the item “aging” (Cronbach’s α = 0.746).
Factor analysis of the IPQ-R listing the items and their respective factor loading.
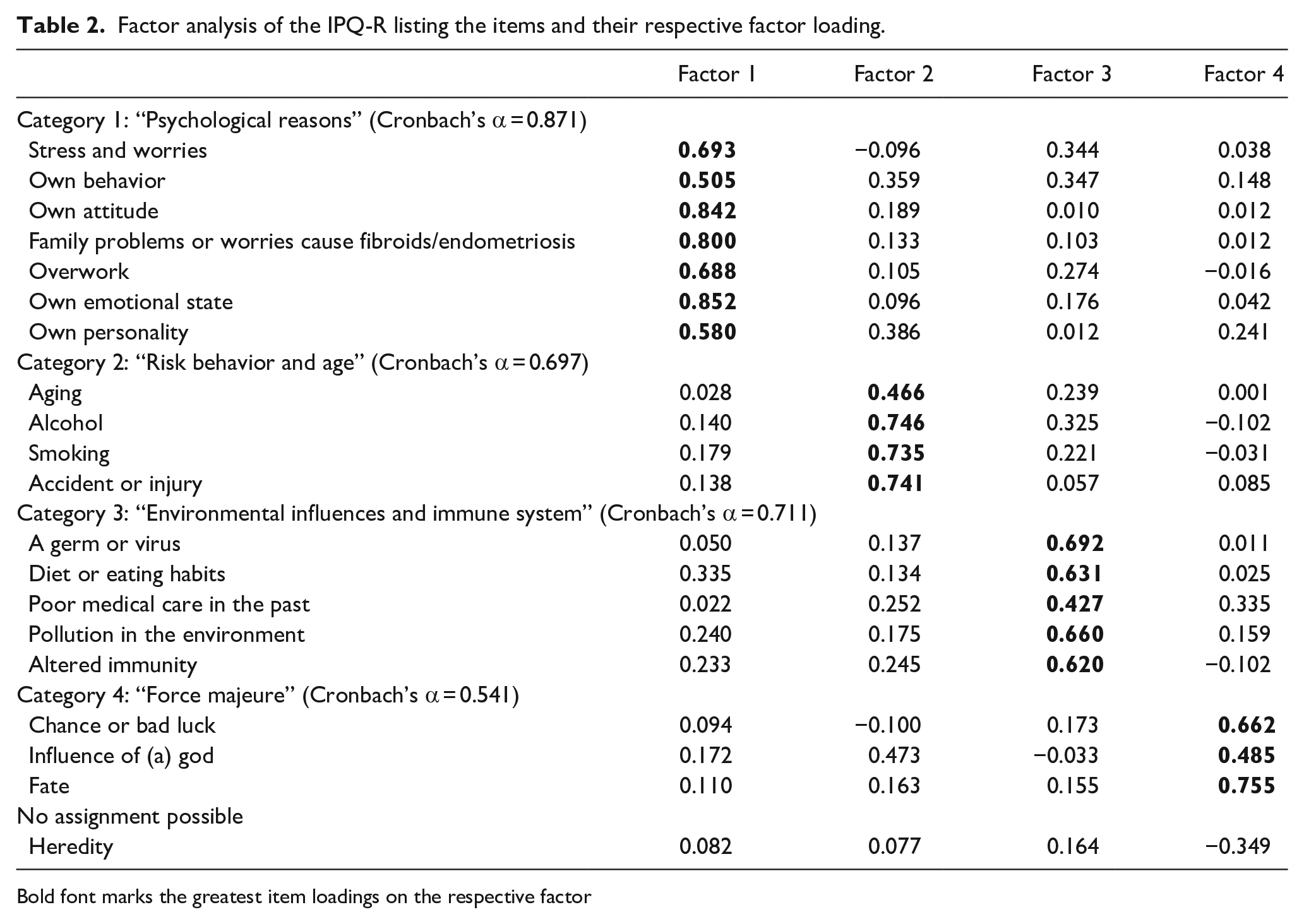
Bold font marks the greatest item loadings on the respective factor
Patients with endometriosis were more likely to agree to questions belonging to the category “environmental influences and immune system” than patients with fibroids (p = 0.009). Both groups showed the same agreement rate regarding the categories “psychological reasons” (p = 0.361) and “risk behavior” (p = 0.469).
Factors influencing patients’ IPQ-R responses
The results of a multivariate analysis revealed that potential influencing factors such as differences in age, migration background, self-assessed knowledge about the illness, or formal education had no effect on differences between the fibroid and the endometriosis groups. We then analyzed whether these factors had an impact on the responses regardless of the illness. We found that migration background and self-assessed knowledge did not affect the responses of patients in the overall collective. However, older patients were more likely to consider “aging” to be the cause of their illness (taub = +0.25; p < 0.001), while younger patients tended to attribute it more to “chance or bad luck” (taub = − 0.10; p = 0.010) (see Table 3).
Factors influencing the response behavior of patients in the IPQ-R.
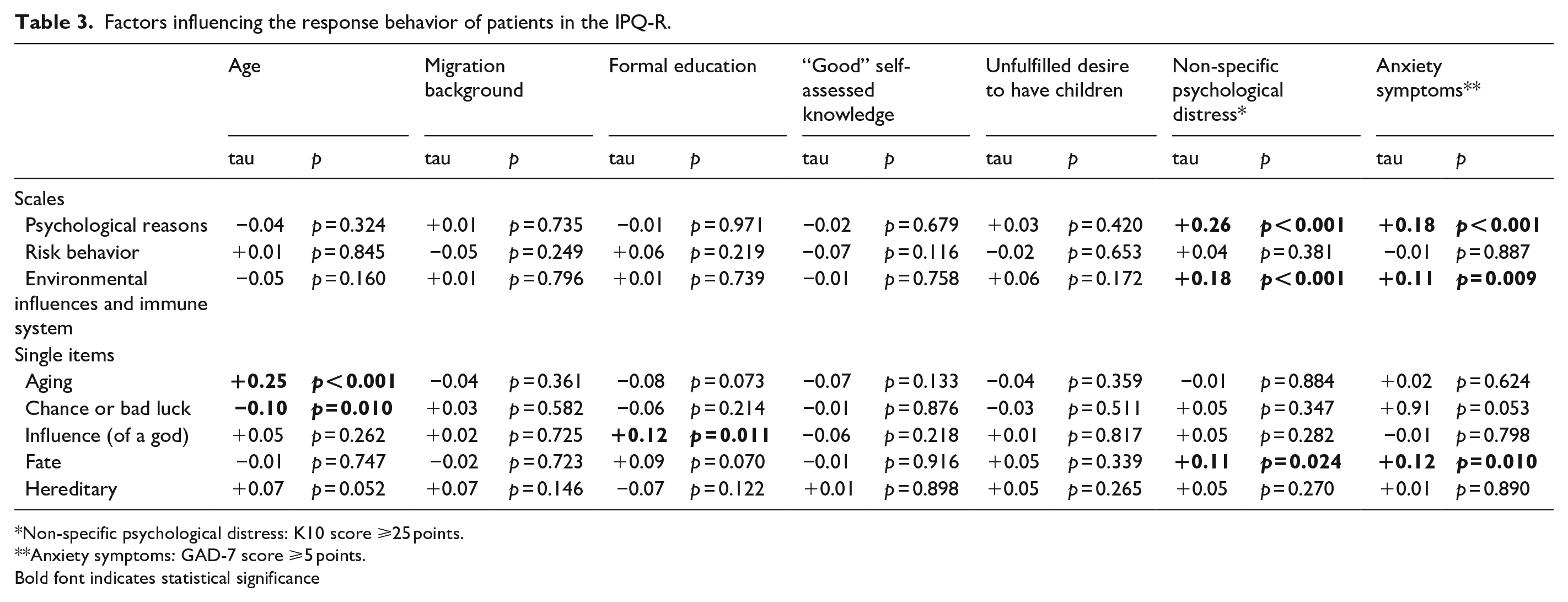
Non-specific psychological distress: K10 score ⩾25 points.
Anxiety symptoms: GAD-7 score ⩾5 points.
Bold font indicates statistical significance
Patients with a suspected diagnosis of a (moderately) severe mental disorder based on the K10 questionnaire (K10 score ⩾25 points) and patients with anxiety symptoms according to the GAD-7 (GAD-7 score ⩾5 points) were more likely to cite “psychological reasons,” “environmental influences and immune system,” and “fate” as cause of their illness (see Table 3).
Discussion
This is the first study that analyzes subjective theories of illness in patients with endometriosis using a standardized questionnaire and also the first study comparing subjective theories of illness in patients with endometriosis and fibroids. Research groups from various disciplines have successfully compared subjective illness theories for two illnesses with certain similarities, so it seems valid and reasonable to compare subjective illness theories in patients with fibroids and patients with endometriosis, since both are benign chronic proliferative illnesses in gynecology.27–30
As in other studies concerning patients with tumors, irritable bowel syndrome or fibroids, the proportion of patients who agreed to at least one possible subjective theory of illness when completing a standardized questionnaire such as the IPQ-R was very high (over 90%).14,31,32
One in six patients with endometriosis and one in eleven patients with fibroids reported feeling uncomfortable sharing personal thoughts about the cause of their illness with their physician. Many patients with endometriosis have experienced a long history of suffering as well as poor communication with physicians, resulting in frequent changes of their physician, which might be holding them back from sharing their subjective theory of illness.33,34
Among the IPQ-R questionnaire, “stress or worry” was the most commonly assumed cause of illness in both patients with fibroids and patients with endometriosis, while the latter were even more likely to perceive this as the main cause than patients with fibroids. A previous study on subjective theories of illness in fibroid patients also confirmed stress as a frequently mentioned factor. 14 According to the only published study on subjective theories of illness in endometriosis patients to date, one in eight women assumed that the cause of their illness was prioritizing their career. 16 Stress as a cause of illness is receiving more and more attention, and the notion of stress is now thought to be dominant in our culture.6,7,35,36 It is no surprise that this is also reflected in patients’ subjective theories of illness. Other studies on subjective theories of illness suggest that patients assuming psychosomatic causes tend to suffer from a higher rate of depression, guilt and an increased level of perceived emotional distress.36,37
Another commonly assumed risk factor in both groups was heredity. On the whole, patients with fibroids were more likely to attribute their illness to heredity than patients with endometriosis. According to current research, genetic factors do play a role in the development of both illnesses: Women with a positive family history of fibroids are three times more likely to develop the illness themselves. 21 The occurrence of endometriosis in first-degree relatives increases the personal risk of also developing the illness by a factor of 3–9. 22 Previous studies on the subjective illness theories of patients with fibroids confirm that patients frequently assumed “hereditary factors” to be the cause of their illness. 14 When patients believe that the cause of their illness cannot be influenced, they tend to worry less about their own (deficient) behavior. Perceiving one’s illness as hereditary can thus have a relieving effect. 38
Patients with endometriosis were more likely to agree to questions from the category “environmental influences and immune system” than patients with fibroids. According to current research, it is likely that immunological changes play a role in the development of endometriosis. 39 The reason why almost one in two endometriosis patients believed that the immune system was involved in the development of their illness might be due to the fact that this knowledge is spreading among patients. According to a paper on the coverage of endometriosis in the press, endometriosis is frequently associated with autoimmune diseases and environmental pollutants in women’s magazines. 40 There has been an increase in subjective theories of illness involving environmental, nutritional and immune factors regarding other illnesses as well.7,36 It is assumed that patients are more likely to choose subjective theories of illness relating to topics that are currently debated in society, such as environmental pollution, the immune system, or a poor diet. This becomes especially apparent when applying a questionnaire to collect data. 36
Being aware of the factors that influence patients’ subjective theories of illness is important when identifying groups of patients who are particularly and adversely impacted by certain theories and who might benefit from support in coming to terms with them. 5
Age
Older patients are more likely to attribute their illness to aging than to chance. Studies relating to other medical conditions have confirmed that older people are more likely to attribute their health problems to age.41,42
In the first study on subjective theories of illness in patients with fibroids published in 1983, 9% of patients assumed that aging might be the cause of their illness. 15 In our study cohort, more than 50% assumed that there was a correlation.
Migration background
Although results from previous studies suggested that having a migration background might impact one’s subjective theory of illness, our study did not confirm this. According to some studies, patients with migration background were more likely to favor external causal attributions.14,35,43
Psychological irregularities
Patients with test scores indicative of general psychological distress (K10) or anxiety symptoms (GAD-7) were more likely to assume psychological reasons, environmental factors and disorders of the immune system as well as “fate” as the cause of their illness. A different study on heart failure patients showed that patients with an elevated GAD-7 score favored theories that attributed the cause of their illness to psychological reasons. 44 It is conceivable that patients who believe that their illness is rooted in their psyche are more likely to blame themselves for their illness and, as a result, develop more anxieties. 27 Considering that these patients seem to have difficulties in coping with their illness and tend to feel guilty, they should be offered psychosocial support.36,37
Strengths and weaknesses of the study
The study presented here is the first cross-sectional study assessing and comparing the subjective theories of illness of patients with fibroids and patients with endometriosis. The rate of patients who refused to participate in the survey was low (11.6%).
We collected the data by means of an established questionnaire (IPQ-R), which is considered to be a rather rigid survey instrument, but which ensures good comparability of the results obtained. The results presented here can only be generalized to a limited extent, as the participants were selected locally in a specialized outpatient clinic or practice.
Footnotes
Authors’ note
Parts of this manuscript are based on the first author’s dissertation.
Authorship
F.M. and M.D. researched literature and conceived the study. A.D.E., S.M., M.D., and F.M. were involved in patient recruitment. R.R. and F.M. were involved in data analysis. F.M. and M.D. wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Ethical approval
Ethical approval for this study was obtained from the ethics committee of the Charité-Universitätsmedizin Berlin (application number: EA4/088/17).
Informed consent to participate
Written informed consent was obtained from all participants before the study.
Informed consent to publish
Written informed consent was obtained from the patients for their anonymized information to be published in this article.