
Abstract
Despite the development of implant-supported prostheses, there are still patients for whom conservative treatments such as resin-bonded fixed dental prostheses (RBFDPs) are more appropriate. This study’s objective was to analyze the available research on full-ceramic RBFDPs. In this study, Web of Science, MEDLINE/PubMed, Scopus, Embase, Cochrane Library, and Google Scholar databases were searched for articles published in English between 2010 and 2020. A total of 14 studies were reviewed based on the eligibility criteria. The results showed that using a cantilever design with one abutment had an advantage over two abutments. Additionally, it was proposed that preparations designed with retentive aids, such as a proximal box, groove, and pinhole, could improve RBFDP survival rates. IPS e.max ZirCAD, In-Ceram alumina, and zirconia CAD/CAM were the most commonly used framework materials. Most studies used air abrasion, salinization, or hydrofluoric acid for surface treatment. Adhesive resin cements were the most frequently used type of cement. The survival rate of In-Ceram ceramics (85.3%–94.8%) was lower than that of In-Ceram zirconia and IPS e.max ZirCAD. Debonding, followed by framework fracture, was the leading cause of failure. Following 3–10 years follow-up, the survival percentage of all-ceramic RBFDPs ranged from 76% to 100%. Although RBFDPs have demonstrated satisfactory success as a conservative treatment, long-term follow-ups and higher sample sizes in clinical research are required to gain more reliable outcomes on the clinical success rate of various RBFDP designs.
Keywords
Introduction
Resin-bonded fixed dental prostheses (RBFDPs) were first introduced in 1970 by Rochette et al. 1 as an interim minimally invasive fixed dental prosthesis (FDP) for the replacement of the lost anterior teeth. 1 In 1980, the Maryland bridge was introduced to the market following the electroetching technique of nickel-chromium alloys, which allowed micromechanical bonding of resin cements to metal surfaces. 2 RBFDPs with metal framework have long been used as an alternative to conventional bridges when the abutments are sound or have insignificant carious lesions.1–4 The main advantage of RBFDPs is their conservative design, requiring minimum/no tooth preparation design, compared to conventional FDPs. Moreover, RBFDPs may serve as a potential substitute for dental implants in juvenile patients or those with anatomical or financial limitations for dental implant treatment. 5 The durability of RBFDPs has increased with new abutment tooth preparation techniques and the improvement of resin bond to metal by different chemical and mechanical techniques.1,6–8 However, there are still some drawbacks to this therapeutic approach. For example, the failure rate of RBFDPs is relatively higher than that of conventional FDPs 9 and implant-supported single restorations 10 due to debonding or fracture of restoration. Thus, RBFDPs were first introduced as an interim restoration; however, they are no longer considered an interim treatment due to the advances in dental materials, cements, and clinical techniques. Nonetheless, metal-ceramic RBFDPs have shortcomings, such as compromising the translucency of the prepared tooth and pontic, notably in the anterior esthetic zone. 11 Esthetic problems due to the grayish color of metal, poor biocompatibility following corrosion, and induction of allergic or even mitogenic reactions have been reported following the placement of these restorations.12–15 Full-ceramic RBFDPs (Figure 1) were introduced as metal-free restorations to overcome the abovementioned shortcomings. Significant advances in material science led to the development of full-ceramic restorations with desirable optical and biomechanical features, which soon gained popularity.

A clinical case of a resin-bonded fixed dental prosthesis to replace bilateral missing spaces in the lower anterior region.
The first metal-free full-ceramic RBFDP was introduced by Kern et al. 7 Different ceramic systems were used to fabricate RBFDPs. 17 In brief, there are three classes of dental ceramics,16,18 including (I) glass, 19 particle-filled glass, and (III) polycrystalline ceramics (Figure 2). Glass-ceramics, composed primarily of feldspar, have limited flexural strength and are not appropriate for restoring load-bearing sites (molar teeth). Leucite and aluminum oxide, as filler particles, have been added to glass ceramics to enhance their optical and mechanical properties. As reported, particle-filled glass ceramics can also be used in fixed partial dentures; however, they may not have a satisfactory prognosis. 20 Polycrystalline ceramics devoid of the glass phase are much harder than glass ceramics. 21 For example, yttria-stabilized tetragonal zirconia polycrystalline ceramic has high flexural strength (900–1400 MPa) and can be used in fabricating FDPs for the posterior regions. 22 RBFDPs made of glass ceramics have higher esthetics, wear resistance, and lower plaque accumulation; however, they require a specific bonding protocol before cementation. 23 Glass ceramics reinforced with leucite and lithium disilicate and infiltrated ceramics such as In-Ceram and zirconia have been used for this purpose. The main advantages of zirconia include its high flexural strength, optimal esthetics, favorable biocompatibility, and higher durability compared with other materials. 24 The first all-ceramic RBFDPs demonstrated high fracture rates, mainly at the connector area. 25
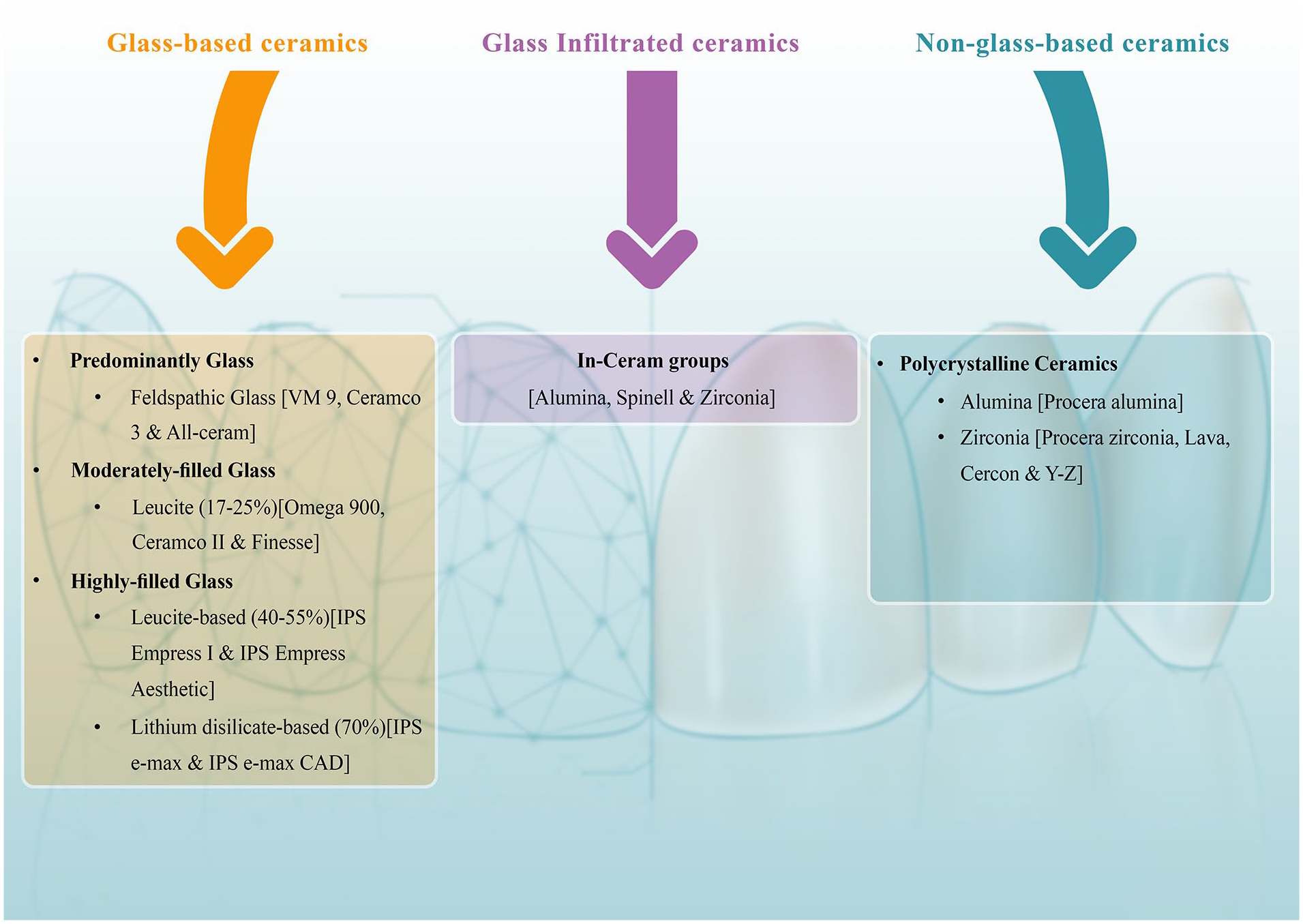
Classification of ceramic materials used in dentistry.
Nonetheless, their survival rate improved by improving the mechanical properties of materials 11 and single abutment designs.26,27 The survival rate of these restorations varies in different studies, ranging from 73.9% to 100%. This variability can be due to differences in tooth preparation design, framework design, ceramic surface treatment, and cement type.18,27–32 For instance, tooth preparation should create a suitable surface for bonding and minimize tensile forces. It may vary from no preparation to conservative or invasive preparation with grooves or wrap-around style.12,33 Despite higher esthetics, all-ceramic RBFDPs have demonstrated shortcomings, including an increased risk of debonding and framework fracture. 33 The type of ceramic plays a fundamental role in such complications.14,34 Since minimally invasive dentistry is a logical approach that needs to be considered in diagnosis and treatment planning, using all-ceramic RBFDPs is currently a promising option for replacing lost teeth in case of trauma or congenital missing of the teeth in adolescents. 35 Despite the availability of clinical studies on all-ceramic RBFDPs,1,10,11,20,22,36 a comprehensive review regarding the restoration design, tooth preparation, type of ceramics used for RBFDPs, ceramic surface treatments, type of cement, survival rate, and complications of RBFDPs has not been performed. Thus, this review study aimed to address these topics.
Materials and methods
Study design and principal question
This study was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and Cochrane Handbook for systematic reviews. 22 The review protocol was registered at the Open Science Framework (https://doi.org/10.17605/OSF.IO/A7K5J). “What are the current concepts regarding the application of all-ceramic resin-bonded bridges as a fixed tooth-replacement option in esthetic dentistry?” was the principal research question formulated for this study based on the established “population, intervention, comparison, and outcome” criteria (PICO; P: Need for an esthetic and fixed anterior tooth-replacement restoration, I: All-ceramic resin-bonded restorations, C: Not applicable, O: Indications, contraindications, advantages, disadvantages, preparation design, retentive factors, ceramic type, restoration and tooth surface preparation, cementation, factors involved in their clinical success, survival rate, and failure rate).
Search strategy
In this study, data were collected by electronic search of the Web of Science, PubMed, Scopus, Embase, Cochrane Library, and Google Scholar databases for relevant articles published between January 2010 and September 2022. The following keywords were searched in quotation marks and by using the Boolean operators of <AND> and <OR>: “Denture, Partial, Fixed, Ceramics, Bridge, Fixed Partial Denture, Resin-Bonded Ceramics, Resin-Bonded Bridge, Resin-Bonded Acid-Etched Fixed Partial Denture, Maryland Bridge, Resin-Bonded Fixed Partial Denture, All Ceramic Acid Etched Bridges, All Ceramic Resin Bonded Bridges, All Ceramic Adhesive Bridges, and Ceramic Bonded, Denture, Partial, Fixed, Resin-Bonded, Ceramics, All Ceramic Acid Etched Bridges, All Ceramic Resin Bonded Bridges, All Ceramic Adhesive Bridges, Survival Rate, Bridge, Resin Bonded, and Ceramic Bonded.” Records were imported into a reference management platform (Endnote 20; Clarivate Analytics) for further screening.
Eligibility criteria
Clinical trials, cohort studies (prospective and retrospective), literature/systematic reviews, and meta-analyses published in English and peer-reviewed journals formed the inclusion criteria. Doctoral dissertations, letters to editors, editorials, short communications, histological studies, animal studies, in vitro studies, clinical reports, case reports, book chapters, expert opinions, studies published in non-English languages, studies with insufficient data, and those that did not meet the eligibility requirements were all excluded.
Study selection and data extraction
The title/abstract screening stage was performed independently by two reviewers (SAM and FK) in the EndNote 20 software, removing duplicated records and those irrelevant to the topic of this study. The screening procedure was concluded by the same screeners cross-referencing the full texts of the remaining possibly eligible publications with the inclusion/exclusion criteria. Before starting the evaluation process, 10% of the articles up for screening were reviewed randomly to calibrate the screeners. The reference list of the included articles was also manually searched to find any other potentially relevant articles. During the screening process, disagreements between the two reviewers were settled by consensus or consulting with a third author (SH). Cohen’s Kappa coefficient was used to assess the inter-reviewer reliability for the screening processes. The cut-off point was set at 80%, and the kappa value (к) was determined by considering the frequency of exact agreements among reviewers.
Author, publication year, title, study design, follow-up duration, number of patients, mean age and age range of patients, number of excluded patients, survival rate, failure rate, framework design, tooth preparation design, surface treatment of prosthesis, and cement type were retrieved from the selected articles. A third author (AH) helped to settle conflicts in the data extraction process.
Quality assessment
Two reviewers (SAM and FK) evaluated each study’s risk of bias (RoB). The JBI critical appraisal checklist (https://jbi.global/critical-appraisal-tools), 37 a scoring system based on yes/no/unclear ratings, was used for systematic reviews.
Version 2 of the Cochrane risk-of-bias tool for randomized trials (RoB 2) 38 was used for the quality assessment of clinical trials. The guideline evaluates five domains of bias: randomization, deviations from intended interventions, missing data, outcome measurement, and selection of reported results. Risk-of-bias VISualization (robvis), 39 a web app for visualizing risk-of-bias assessments, was used to create the associated graph.
The RoB in the cohort studies was assessed using the Newcastle–Ottawa Assessment Scale (NOS). 40 (1) study group selection, (2) group comparability, and (3) outcome measurement were the three domains that were taken into account in the assessment. Each study could receive up to nine points using this rating system (selection: up to 4, comparability: up to 2, and outcome: up to 3), and the overall scores were deciphered as follows: very high RoB (0–3 points), high RoB (4-6 points), and low RoB (7–9 points). 41
Results
Study selection
A total of 936 articles were retrieved by electronic search of databases, and eventually, 14 studies were found to be eligible for inclusion in this review (Figure 3). Cohen’s Kappa coefficient results for both screening phases showed almost perfect inter-rater agreements (к1 = 0.86 and к2 = 0.94).
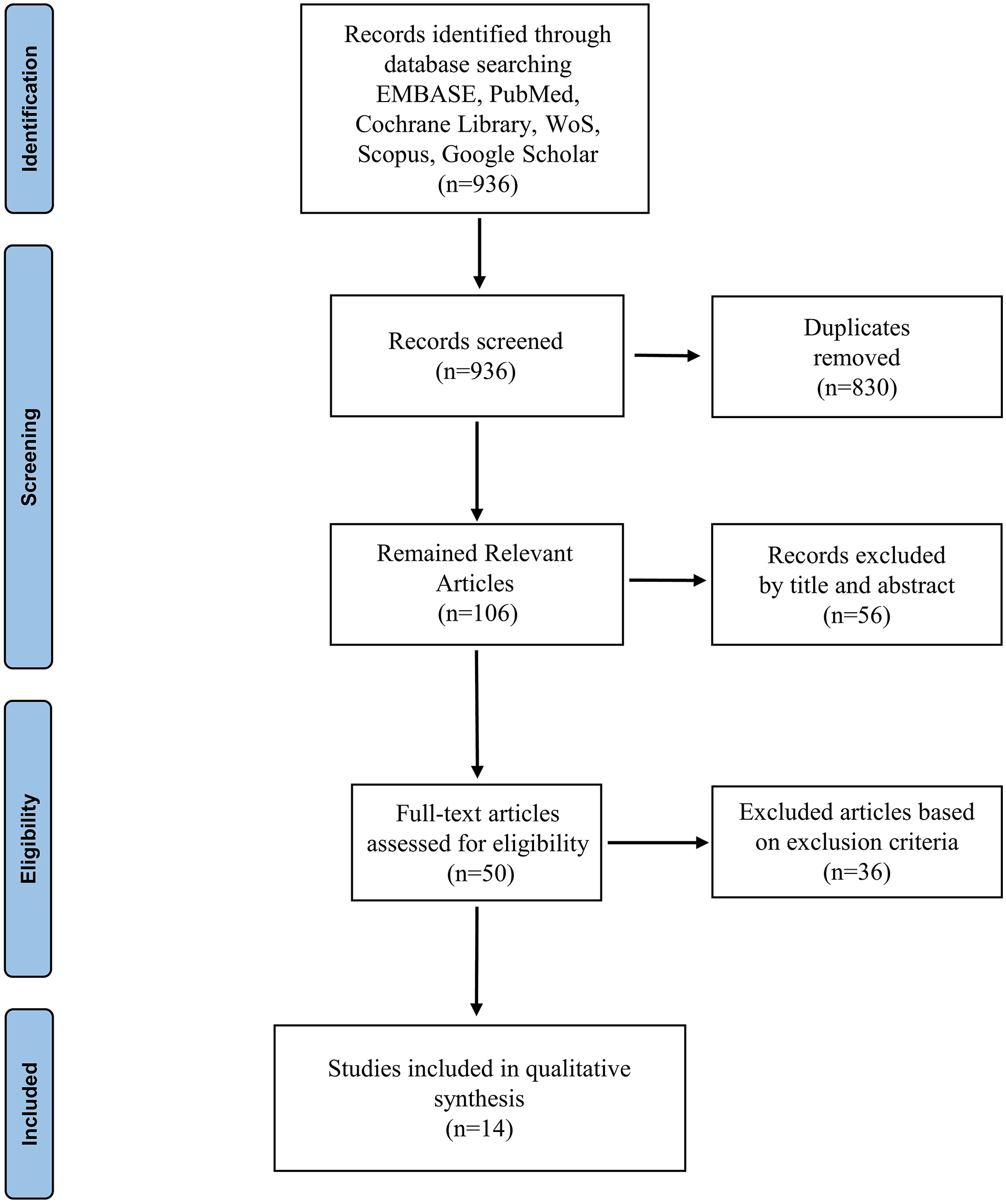
Flowchart of the screening processes.
Study characteristics
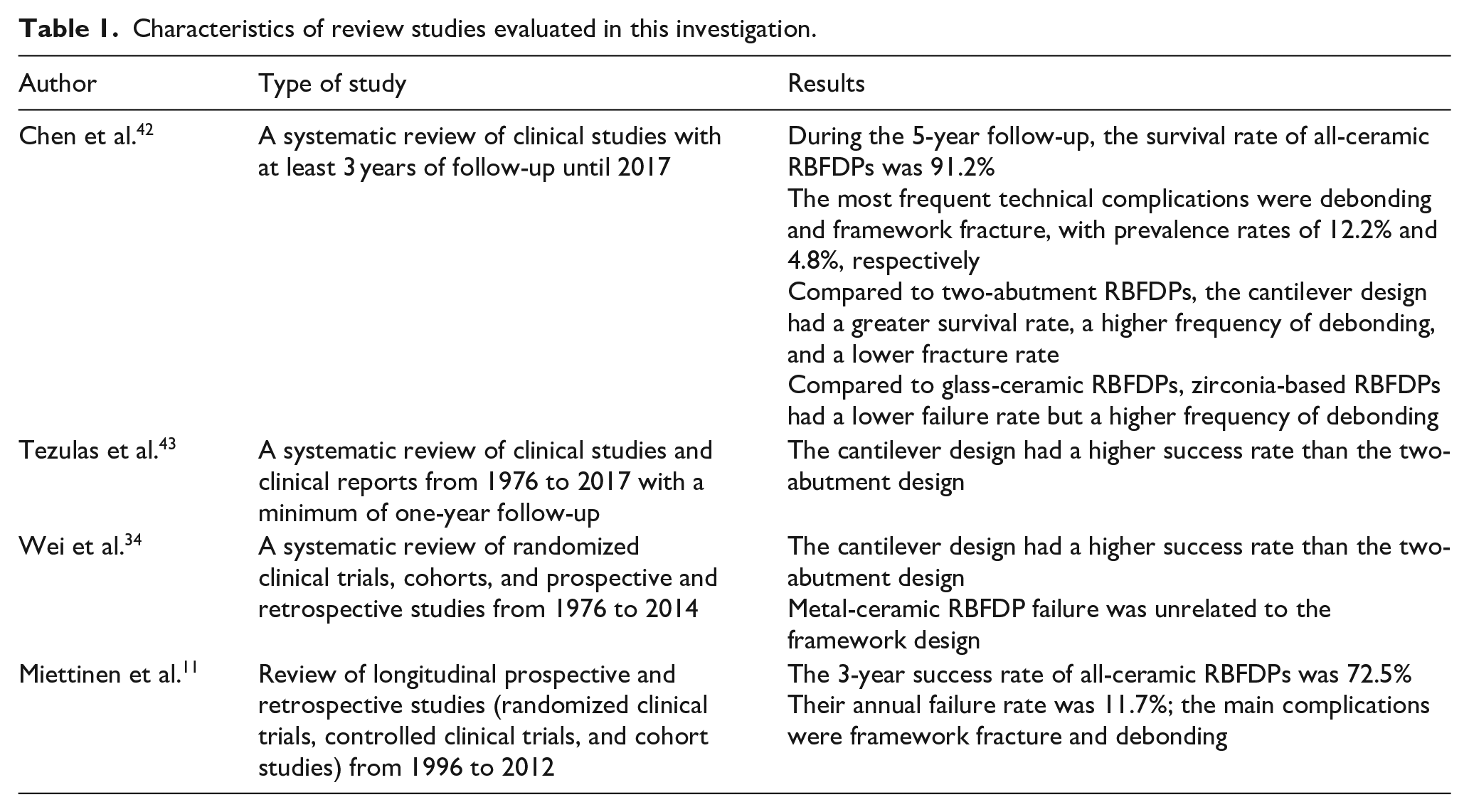
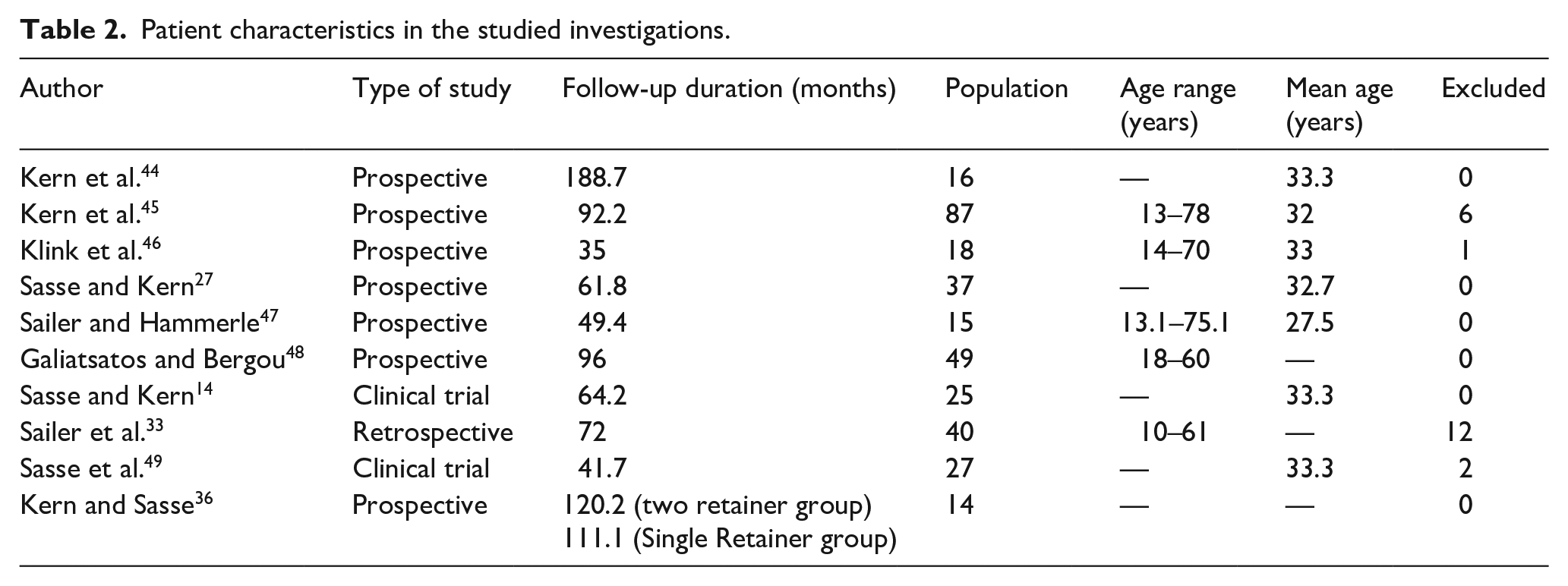
Table 1 presents the systematic reviews evaluated in this study. Two articles were retrospective, two were clinical trials, and six were prospective. The duration of follow-up ranged from 1 to 10 years, and the patients were aged 13–78 years (Table 2).
Characteristics of review studies evaluated in this investigation.
Patient characteristics in the studied investigations.
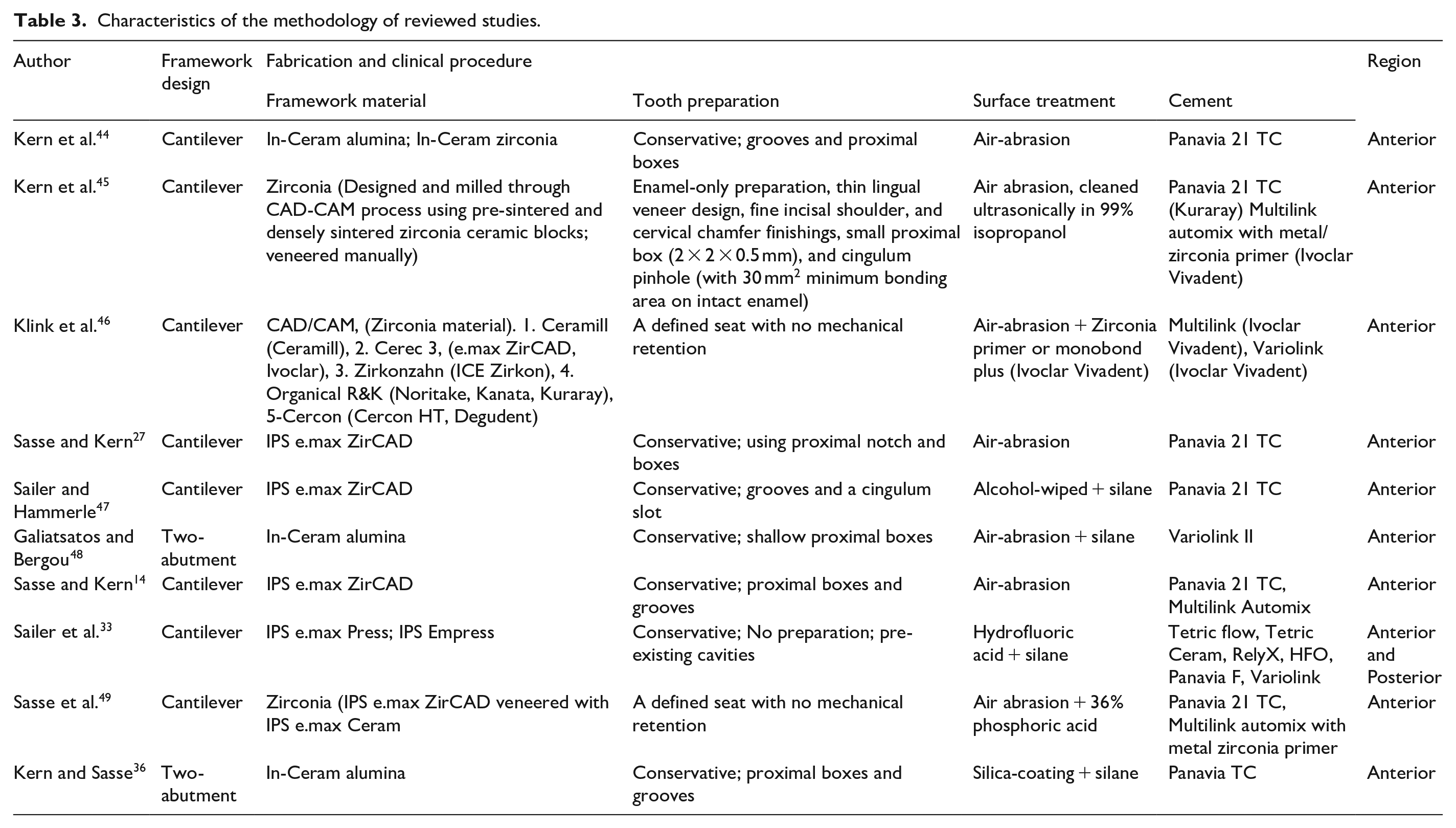
Regarding the framework design, two articles reported the two-abutment design, and eight reported the cantilever design of restorations. The most commonly used framework material was IPS e.max ZirCAD in three articles, In-Ceram alumina in three articles, CAD/CAM zirconia in two, In-Ceram zirconia in one, and IPS e.max Press also in one study. Tooth preparation was conservative, with grooves and proximal boxes in most studies. Air abrasion was used for surface treatment in all studies. Panavia cement was used in eight, Multilink in five, Variolink in two, and Tetric Flow in one study. All analyses were conducted on anterior teeth, and only one assessed both anterior and posterior teeth (Table 3).
Characteristics of the methodology of reviewed studies.
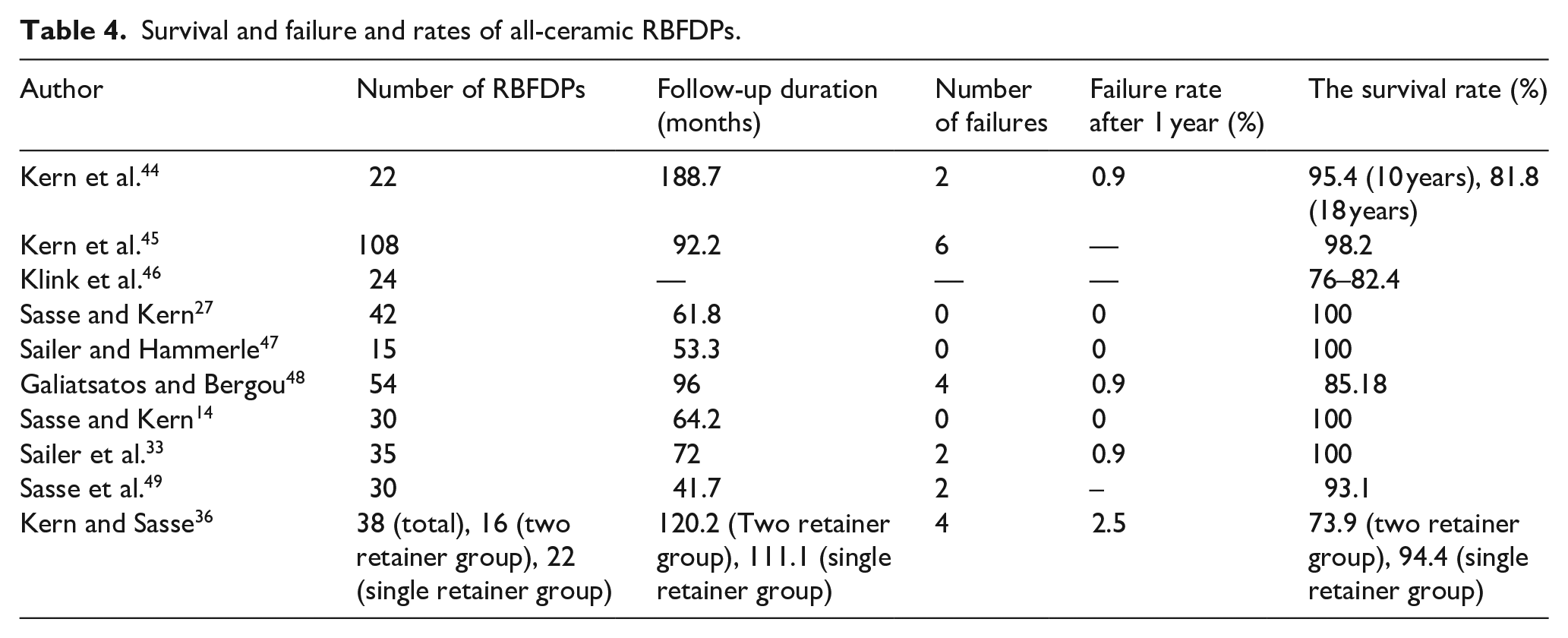
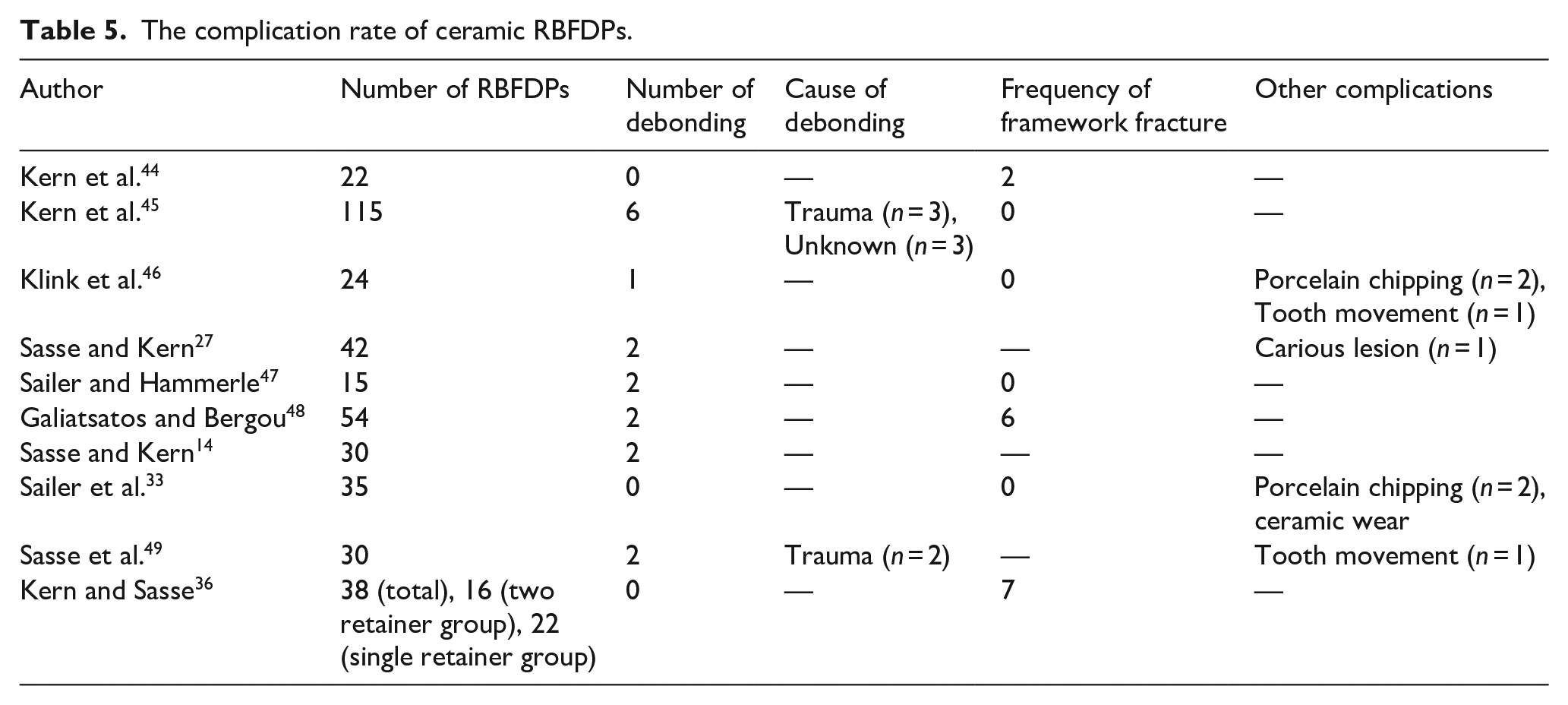
The survival rate of all-ceramic RBFDPs after 3–10 years of follow-up ranged from 76% to 100%. Tables 4 and 5 show that the frequency of debonding of all-ceramic RBFDPs ranged from 0 to 6.
Survival and failure and rates of all-ceramic RBFDPs.
The complication rate of ceramic RBFDPs.
Quality assessment
Table 6 presents the quality assessment results of the systematic reviews included in this study. All studies provided adequate clinical recommendations supported by the reported data; however, none succeeded in applying methods to minimize errors in the data extraction step and assessing the risk of publication bias.
Systematic reviews’ quality assessment using the JBI critical appraisal checklist.
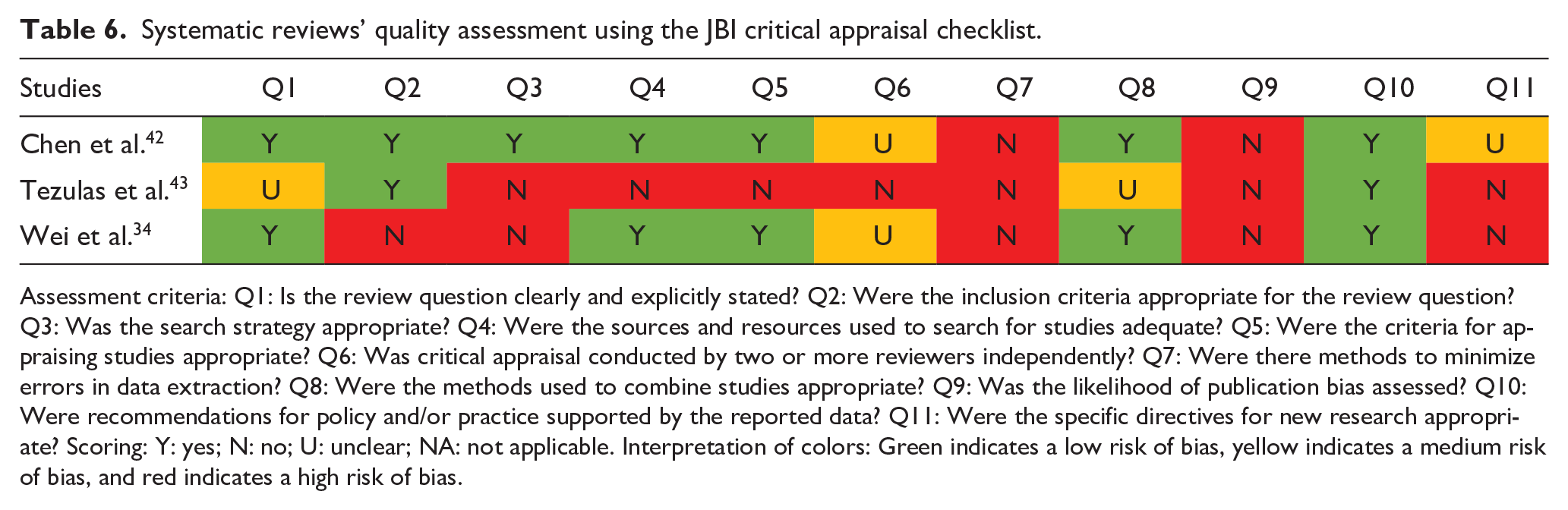

Assessment criteria: Q1: Is the review question clearly and explicitly stated? Q2: Were the inclusion criteria appropriate for the review question? Q3: Was the search strategy appropriate? Q4: Were the sources and resources used to search for studies adequate? Q5: Were the criteria for appraising studies appropriate? Q6: Was critical appraisal conducted by two or more reviewers independently? Q7: Were there methods to minimize errors in data extraction? Q8: Were the methods used to combine studies appropriate? Q9: Was the likelihood of publication bias assessed? Q10: Were recommendations for policy and/or practice supported by the reported data? Q11: Were the specific directives for new research appropriate? Scoring: Y: yes; N: no; U: unclear; NA: not applicable. Interpretation of colors: Green indicates a low risk of bias, yellow indicates a medium risk of bias, and red indicates a high risk of bias.
Figure 4 also displays the results of the clinical trials’ quality assessment using the RoB 2 tool; both included studies demonstrated some concerns following the evaluation.
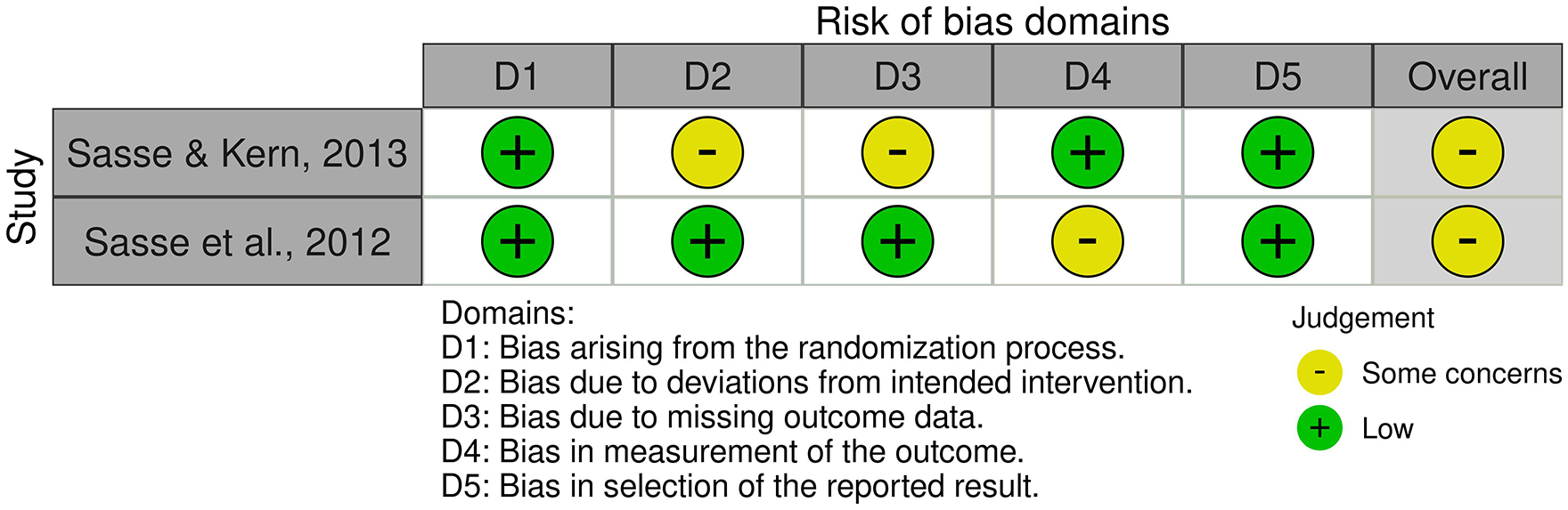
The traffic light plot demonstrates the quality assessment of the clinical trials using the RoB 2 tool.
Table 7 details the scoring methodology used for the included cohort studies. None of the cohort studies demonstrated a low RoB; no star ranking was possible for the “comparability” domain since none described the baseline control for patient selection.
The cohort studies’ quality assessment results using the Newcastle–Ottawa Scale.
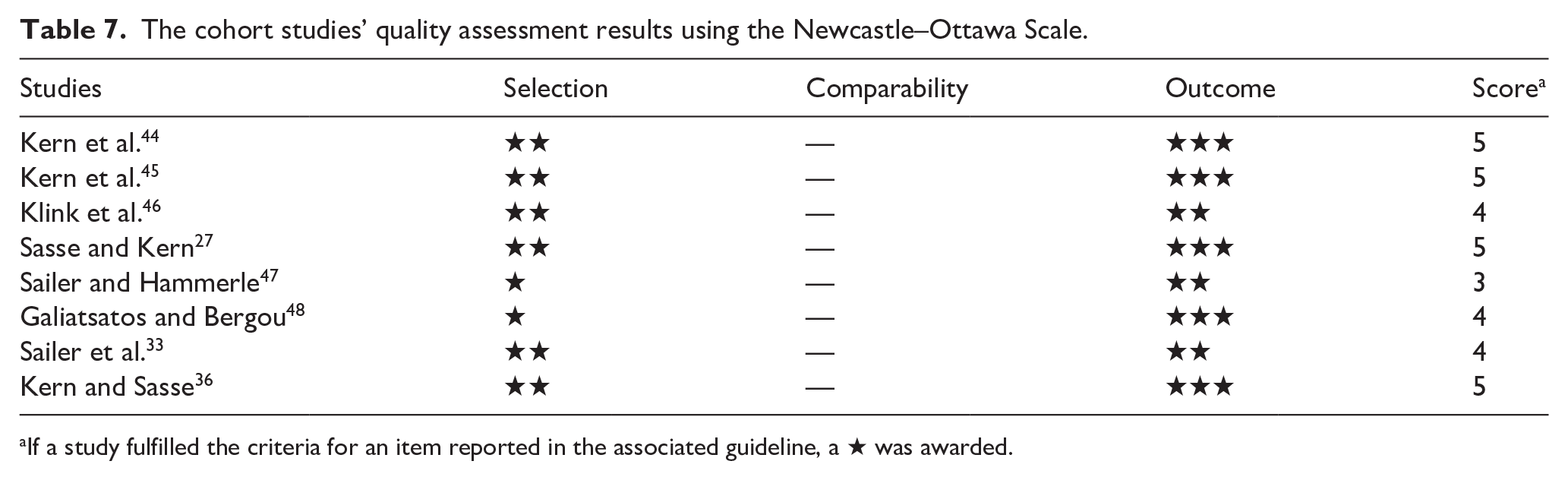
If a study fulfilled the criteria for an item reported in the associated guideline, a ★ was awarded.
Discussion
RBFDPs have long been used as an alternative to conventional bridges when the abutment teeth are sound or have insignificant caries.1–4 With improvements in the mechanical properties of ceramics and their optimal esthetics and biocompatibility, all-ceramic RBFDPs became increasingly popular. 42 All-ceramic RBFDPs are a conservative alternative for replacing missed anterior teeth. 48 Their clinical indications include sound abutments and short-span edentulism, including replacing a single tooth with minimal dynamic occlusal contacts.20,48,50 RBFDPs have many advantages resulting from a combination of composite resins’ (bonding, tooth structure preservation) and ceramics (high color stability, increased wear resistance, similar coefficient of thermal expansion to enamel, and optimal esthetics) advantages. 48 This review study aimed to assess all-ceramic RBFDPs regarding their indications, contraindications, advantages, disadvantages, preparation design, retentive factors, ceramic type, restoration and tooth surface preparation, cementation, factors involved in their clinical success, survival rate, and failure rate.
Cantilever design versus the two-abutment design
Cantilever all-ceramic RBFDPs may be preferred for several reasons. In contrast to the two-abutment design, the cantilever design is less susceptible to errors in preparation, impression technique, and technical procedure. Also, cantilever restorations only require the preparation of one tooth (and consequently have a lower risk of pulp involvement, caries, or fracture). In this design, changing the degree of movement of the abutment tooth does not affect the precision of the adhesive seal or future load distribution. Moreover, when debonding of a cantilever restoration occurs, the patient is immediately aware of it; thus, the risk of caries extension under the debonded retainer, often the case for two-abutment designs, is lower. 51 In the present study, articles that used the two-abutment design with 8 and 10 years of follow-up reported a survival rate of 85.3%–92.6%.36,48 Also, most studies used the cantilever design for all-ceramic RBFDPs and reported a survival rate of 91.7%–100%.27,33,44–47,49 It was demonstrated that the cantilever design was superior to the two-abutment method. Also, systematic reviews.34,42,43 reported that the cantilever design had a lower failure rate than the two-abutment design and was superior to it. The primary cause of the increased failure rate of the two-abutment design might be attributed to movement differences in abutment teeth in function, mainly when they are in protrusive and laterotrusion movements. 36 Nonetheless, the shearing and torsion on pontics and connectors are reduced by the cantilever design due to the simultaneous movements of the pontic with the abutment tooth in function. 34
Abutment preparation
Optimal tooth preparation while preserving the enamel may affect the retention properties of RBFDPs. The retentive and non-retentive preparation designs have been variable in different studies. Proximal boxes/grooves and pin holes have been recommended as retentive aids to increase the RBFDPs’ survival rate. 34 The proximal boxes enable adequate connector thickness and define an insertion path for the proper seating of RBFDPs. They must, therefore, be prepared parallel to the abutment teeth. The lingual fossa’s central cingulum grooves improve the exact placement of the framework three-dimensionally. 43 When using resin cement, a retentive form may not be required. However, a lingual rest would be recommended to seat the restoration precisely. Nonetheless, due to inadequate clinical data, a definite conclusion cannot be drawn in this respect. 34 In the present study, retentive forms were not used in three studies, including a retrospective study, 33 a prospective study, 46 and a clinical trial. 49 The survival rate ranged from 76% to 93.1% in studies that did not use a retentive form.33,46,49 while this range was 85.3%–100% in studies that used retentive forms.27,36,44,45,47,48,50
Restoration surface treatment
Different methods are used for the surface treatment of all-ceramic restorations. Tribochemical silica-coating, a combined form of surface conditioning in which one layer of silica is formed by airborne-particle abrasion with alumina particles coated with silica, could be applied to ceramic restorations, including RBFDPs. Additionally, airborne particle abrasion using aluminum oxide particles under air pressure at a specific distance is used to treat the intaglio surfaces of ceramic RBFDPs. Dual-cure resin cements containing phosphate monomers are recommended to achieve a solid bond to conditioned surfaces. 43 Most reviewed studies used air abrasion, silane, or hydrofluoric acid. The adhesive method may cause debonding of RBFDPs. 48 Kern and Thompson, 52 in their in vitro study, demonstrated that the application of silane after air abrasion of In-Ceram ceramics was not suitable compared with silica coating and silane application or use of resin-containing phosphate monomers after air-abrasion. Galiatsatos et al. 48 reported two cases of debonding of In-Ceramic ceramics and reported that air abrasion followed by silane application was probably the reason for debonding. Nevertheless, it has been reported that compared to conventional surface treatment approaches, silane heat treatments could enhance the bond strength between resin composite and ceramic. 53 Composite resin cement is another essential factor to consider. The failure at the resin-filler bonding interface may cause degradation within the resin structure, contributing to cement failure. This occurrence is caused by various circumstances, such as the polymerization shrinkage of composite resin, the dissolving of resin matrix in oral fluids, the loss of the marginal seal as a result of the polymerization shrinkage, or the removal of cement flashes using blunt instruments. 48 Concerning zirconia, the silica-coating may not optimally penetrate the condensed zirconia structure. Consequently, silane and silica-coating cannot form a solid bond. 42 According to recent studies,33,46,47 Strong bonding to zirconia ceramic in the high-stress and humid oral environment may be achieved through the combined application of luting cements having 10-methacryloyloxy-decyl dihydrogen phosphate and air-abrasion under moderate pressure.42,54–60
Hydrofluoric acid etching before bonding lithium disilicate crowns is recommended for conditioning lithium disilicate surfaces. Hydrofluoric acid-etching creates an irregular surface at the bonding interface of ceramic materials, which increases the bond of resin and ceramic cements. Hydrofluoric acid eliminates the glass matrix and secondary crystalline phase, creating irregularities in lithium disilicate crystals to provide proper bonding strength. Air abrasion using 50 µm aluminum oxide (Al2O3) particles is another suggested technique for conditioning ceramic surfaces to enhance mechanical retention. Airborne abrasion is the standard technique in dental laboratories/offices before delivering ceramic restorations. Silane should then be applied to air-abraded ceramic surfaces to form self-curing bonds between the inorganic ceramic and the organic phase of resin cement. 61
Ceramic type
Primary all-ceramic RBFDPs often break at the connector region. 42 In the reviewed studies, the survival rate of In-Ceram ceramic (85.3%–94.8%) was lower than In-Ceram zirconia and the e.max zirconia (Ivoclar). In-Ceram showed the highest rate of framework fracture.36,44,48,62–64 According to Pjetursson et al.’s 65 systematic review study, all-ceramic FDPs and glass-infiltrated alumina had a 5-year survival rate of 86.2%, which was lower than the rates for densely-sintered zirconia (90.4%) and reinforced glass ceramic (89.1%). Framework fracture frequently results when glass-infiltrated alumina is used as posterior restorations and when the connector diameter is less than 4 mm × 4 mm. 65 Chen et al. 42 reported a higher frequency of framework fracture in RBFDPs fabricated from glass ceramics such as silicate and alumina infiltrated; they have low flexural strength and thus need larger connectors. 42 Some in vitro studies recently used a densely-sintered zirconia-based framework for all-ceramic cantilever RBFDPs and reported 92%, 45 100%,14,47 and 82.4% 46 survival rates. These findings result from the fact that in all-ceramic cantilever RBFDPs fabricated from zirconia, overloading does not lead to fracture of the connector of restorations.
Cement
Different cement types have been used in studies. Resin cements are the most commonly used cements. Panavia EX and Panavia 21 (Kuraray) were the most widely used types of cement. Following the manufacturers’ instructions and properly selecting a biocompatible material are crucial considerations in achieving an uneventful bonding. 66 Sailer et al. 33 assessed six different types of cement, namely Tetric Flow (Ivoclar Vivadent), Tetric Ceram (Ivoclar Vivadent), RelyX (3M ESPE), Panavia F (Kuraray), HFO (Optident), and Variolink (Ivoclar Vivadent) for anterior and posterior restorations; they did not observe any case of debonding. 33 In their study, Klink and Huttig 46 used Variolink and Multilink cements; they reported a 100% survival rate. Sasse et al. 49 evaluated the bonding strength of two types of resin cements (Multilink-Automix with metal/zirconia primer and Panavia 21) for bonding RBFDPs and found no significant differences. Regarding RBFDPs, experimental studies demonstrated that a reliable bond could be obtained by air-abrasion of the zirconia surface before bonding, followed by composite resins containing phosphate monomers. 67 Nonetheless, no significant differences were noted in the survival rate of RBFDPs using these bonding systems. 68
Occlusion
The reviewed studies did not mention anything about the occlusion of patients. However, the type of functional occlusion is highly determinant in using all-ceramic RBFDPs because loads may be concentrated on RBFDPs. In canine-guide occlusion, if the abutment tooth is the canine tooth, the load applied to the canine tooth may adversely affect the RBFDPs of the two abutments. While masticating, the load applied to the canine in the two-abutment design may be transmitted to the central incisor. 43 This might explain why researchers have reported a lower success rate of the two-abutment design than the cantilever design.36,43,48 Thus, the cantilever design can be a suitable treatment option because the canine tooth is subjected to lateral forces during mastication, and the pontic may shift towards the canine tooth. If the movements of the two teeth adjacent to the abutment differ, the cantilever design may be preferred. 43
Influential factors in the failure
Debonding is the leading cause of failure of RBFDPs. 69 In this study, the maximum frequency of debonding (n = 6) was reported by Kern et al., 45 half of which occurred due to trauma. The framework material in their study was zirconia. Regarding RBFDPs fabricated from zirconia ceramic, overloading, even due to traumatic effects, can cause debonding. Zirconia has a flexural strength twice that of glass-infiltrated alumina ceramic. Thus, re-bonding of zirconia RBFDPs is possible without complication, whereas failed alumina RBFDPs or those with framework fracture require replacement. 45 In a study by Sailer et al., 70 the most common cause of failure of FDPs fabricated from glass-ceramics or glass-infiltrated ceramics was a failure in the reconstruction of framework or the veneering ceramic; nonetheless, using zirconia as framework caused biological and technical failures primarily and not framework fracture. 70 Pjetursson et al. 71 reported debonding as the most frequent complication in 19.2% of RBFDPs in 5 years.
Survival
In the current review study, survival was defined as the ceramic RBFDPs remaining in place throughout the follow-up phase without experiencing repeated debonding. The overall survival rate of ceramic RBFDPs in the reviewed studies after 3–10 years of follow-up was 76%–100%. According to Sailer et al., 70 metal-ceramic FDPs had a considerably greater 5-year survival rate (94.4%) than all-ceramic FDPs (88.6%). Pjetursson et al. 71 reported the 5-year survival rate of RBFDPs at 87.7%. The survival rate was 85.15% for RBFDPs of anterior teeth in a study by Galiatsatos et al. 48 Pjetursson et al. 65 reported the 5-year survival rate of FDPs fabricated from reinforced glass ceramics to be 89.1%; this rate was 86.2% for glass-infiltrated FDPs and 90.4% for porous compact zirconia FDPs. Kern et al. 44 reported the 10-year and 15-year survival rates of all-ceramic RBFDPs to be 95.4%, with an 18-year survival rate of 81.8%. RBFDPs are an efficient short-term or medium-term restorative modality with high survival and low failure rates. However, it should be noted that not many clinical trials with long-term follow-ups have been conducted on RBFDPs.
Conclusion
Regarding RBFDPs, the cantilever approach is superior to the two-abutment design. Also, teeth incorporating retentive aids in the preparation increase the survival rate. The most commonly used framework material in the reviewed studies was IPS e.max ZirCAD, In-Ceram alumina, and CAD/CAM zirconia. All studies used air abrasion, silane, or hydrofluoric acid for surface treatment. Adhesive resin cements were the most commonly used cements. The use of silane after air abrasion in In-Ceram ceramics was unsuitable compared to silica-coating and silane or phosphate monomers-containing resin after airborne abrasion. In-Ceram ceramic’s survival rate was lower than In-Ceram zirconia and IPS e.max ZirCAD. The highest frequency of framework fracture was noted in In-Ceram. Debonding and framework fracture were the leading causes of failure. After 3–10 years of follow-up, the survival rate of ceramic RBFDPs generally ranged from 76% to 100%. Although RBFDPs are a conservative treatment option with acceptable treatment results, more precise information regarding the clinical success of different designs of these restorations requires more comprehensive clinical trials with prolonged follow-ups.
Footnotes
Acknowledgements
Not applicable.
Authors’ note
Gustavo Vicentis de Oliveira Fernandes is now affiliated to Missouri School of Dentistry & Oral Health, A. T. Still University, St. Louis, MO, USA.
Artak Heboyan is also affiliated to Department of Research Analytics, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai, India.
Author contributions
Conceptualization: SH and SAM; Methodology: SAM, FK, and SH; Software: SAM; Validation: SAM, AH, and SH; Formal analysis: FK; Investigation: FK and SAM; Resources: FK and SAM; Data curation: FK and SAM; Writing—original draft preparation: SH and FK; Writing—review and editing: AH; GVOF and SAM; Visualization: SAM; Supervision: SH; Project administration: AH. All authors have read and approved the published version of the manuscript.
Data availability statement
Not applicable.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent statement
Informed consent was obtained from the subjects whose clinical picture is included in the study.
Sample availability
Not applicable.